COUNTERIRRITANTS (Hot Application) –
Purpose, Classification, Preliminary Assessment, Preparation of Patient and
Environment, Equipment, Procedure and After Care
A counterirritant is a substance which dilates
superficial blood vessels to relieve or counteract other deeper inflammation,
which is turn produce the constriction of deeper vessels.
Counterirritants
are drugs, when applied to the affected part, caused irritation on inflammation
thereby relieving deep seated pain, congestion and inflammation.
Purpose
To relieve congestion
To relieve irritation by promotion
free circulation in the part
To relieve pain
To cause absorption and removal of
inflammatory products
Classification of Counterirritants
Rubefacients: these merely redden the
skin by vasodilatation. These act quickly their action lasts for a short time,
e.g. mustard turpentine liniments
Vesicants: these help blister formation
on skin, e.g. Tr. Iodine
Escharotics: they destroy the tissues
and help them slough away, e.g. silver nitrate
Pustulants: they produce pustules on
skin and are rarely used, e.g. cotton seed oil and antimony
Preliminary Assessment
Check
The doctors order for any specific
precautions
General condition and diagnosis of
the patient
Self-care ability of the patient
Severity and extent of the injury
Type method and duration of
medication applied
Articles available in the unit
Preparation of the Patient and Environment
Explain the procedure to the patient
Provide privacy if needed
Arrange the articles at the bedside
Position the patient comfortably
Equipment
Adult-mixture of ½ dram turpentine
and 2/3 at sweet oil
Children – mixture of 1 part
turpentine and 10 part sweet
Swab sticks
Kidney tray and paper bag
Screen
Procedure
Hand wash
Fan folds the top bedding and exposes
the required part only
The mixture should be well mixed
Apply the warm oil mixture with swab stick
Apply it from xiphist sternum to the
symphysis pubis
Apply the mixture in a single layer
and do not rub it
Apply the hot compresses (medical
fomentation)
After 10 to 15 minutes, insert the
flatus tube and watch for the expulsion of gases
After Care
Remove the articles from the bedside
Position the patient comfortably
Replace the articles after cleaning
Hand washing
Record the procedure in nurse’s
record sheet
Thermotherapy widens blood vessels and increases blood flow to the skin. It relaxes superficial muscles, decreases muscle spasm and reduces stiffness of joints. Moist heat appears to be more effective in treating pain than dry heat, as the moisture allows the heat to penetrate more deeply into the muscle. Thermotherapy is frequently used combination with other therapies to relieve pain, such as hydrotherapy (water therapy). In many cases, cryotherapy (cold therapy) is used to reduce inflammation before thermotherapy is used to increase blood flow to muscles.
COUNTERIRRITANTS (Hot Application) – Purpose, Classification, Preliminary Assessment, Preparation of Patient and Environment, Equipment, Procedure and After Care
COLD PACK (Cold Application) – Definition, Purpose, General Instructions, Preliminary Assessment Check, Effects, Physiologic Effects, Indications, Preparation of the Patient and Environment, Equipment, Procedure, After Care and Contraindications
Cold pack is
defined as application of moist cold when temperature rises to 104 degree F and
above.
PURPOSE
To reduce temperature above 104
degree F
To treat heat stroke and malignancy
hyperthermia
GENERAL INSTRUCTIONS
The pack could be a wash cloth, flannel
or a piece of old linen depending up on the size of the body part to receive
the application
A basin of cold water is prepared and
the packs are immersed into it
When cooled, the excess water is
wrung out and the pack is applied to the body area. Replace the packs as
necessary to maintain
CONTRAINDICATION
Circulatory
disorders like peripheral vascular diseases
PRELIMINARY ASSESSMENT
Check
Check the doctor’s order for any
specific instructions
General condition and diagnosis of
the patient
Self-care ability of the patient
Duration of the treatment
Articles available in the unit
PREPARATION OF THE PATIENT AND ENVIRONMENT
Explain the procedures to the patient
Provide privacy
Arrange the articles at the bed side
Place the patient in comfortable
position
Place the Mackintosh under the
patient
EQUIPMENT
Long Mackintosh
Bed sheet – 2
Bath towel – 6
Cold compress and ice cap equipments
Bucket of cold water
Bath thermometer
Bowl with crushed ice pieces
Hot water bag
PROCEDURE
Wash hands
Pour cold water into basin; add ice
cubes to bring temperature to 65 degree F and wet bath towels
Remove top sheet and protect bed with
long Mackintosh and big sheet
Remove patients cloths, cover with
wet bath towel from chest to pubic area
Place compress on forehead, ice cap
on head and hot water bag at feet
Wrap hand and legs with wet towel
Check the temperature every 15
minutes and replace wet towels
Continue procedure for 30 minutes
AFTER CARE
After completing procedure, remove
towels and dry patient thoroughly
Remove Mackintosh and sheet change
wet sheets
Dress patient and cover with top
sheet
Keep patient in a comfortable
position
Replace the articles after cleaning
Wash hands
Record the procedure in nurse’s
record sheet and vital signs in TPR sheet
Cold, moist compresses are used to reduce swelling and inflammation in soft tissue injuries or after tooth extraction. The size of the compress depends on the area to be treated. Gauze 4 multiply 4 inch pads are frequently used for tooth pain. They are applied externally and are changed frequently because they warm rapidly, thereby losing their effectiveness. In practice, the ice cap, ice collar, or ice bag is a dry cold application. The ice cap, used for the head, has a wide opening that allows it to be filled easily with ice chips, as does the ice collar, a narrow bag curved to fit the neck. Single-use ice bags are frequently used. The primary provider may prescribe dry cold to treat a specific area of the body
COLD PACK (Cold Application) – Definition, Purpose, General Instructions, Preliminary Assessment Check, Effects, Physiologic Effects, Indications, Preparation of the Patient and Environment, Equipment, Procedure, After Care and Contraindications
NEPHROLITHIASIS – Etiology, Risk
Factors, Pathophysiology, Types, Signs and Symptoms, Diagnostic Evaluation and
Management
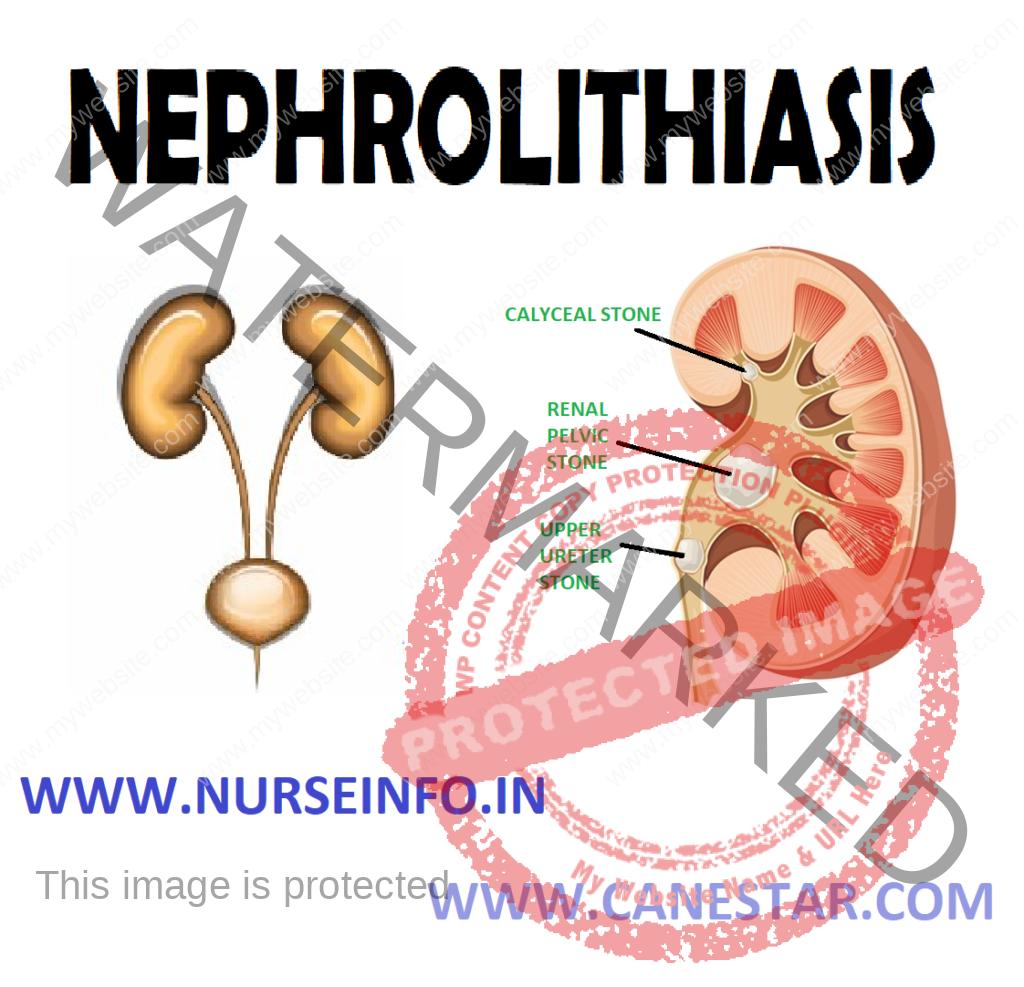
Nephrolithiasis
is also called the renal calculi, are hard, usually small stones that form
somewhere in the renal structure. The stones are masses of crystals and protein
that form when the urine became supersaturated with a salt capable of forming
solid crystals.
Symptoms
occur when the stone become impacted in the urinary tract. When stones are
found in the kidneys, the condition is called nephrolithiasis.
ETIOLOGY
Hypercalcemia and hypercalciuria
caused by hyperparathyroidism
Chronic dehydration, poor fluid
intake and immobility
Chronic infection with urea-splitting
bacteria (proteus vulgaris)
Chronic obstruction with stasis of
urine, foreign bodies within the urinary tract
RISK FACTORS
Metabolic: abnormalities that result
in increased urine levels of calcium, oxaluric acid, uric acid or citric acid
Climate: warm climate that cause
increased fluid loss, low urine volume and increased solute concentration in
the urine
Diet
Large intake of dietary proteins that increases uric acid excretion
Excessive amounts of tea or fruit juices that elevate urinary level
Large intake of calcium and oxalate
Low fluid intake that increases urinary concentration
Genetic factors: family history of
stone formation, cystinuria, gout, or renal acidosis
Lifestyle: sedentary occupation,
immobility
PATHOPHYSIOLOGY
Due to any
cause —- slow urine flow —- resulting supersaturation of the urine with the
particular element —- first become crystallized —- later become stone
TYPES
Calcium oxalate, calcium phosphate,
or mixture
Incidence: 90%
Feature: account for two-third of stones. Small, rough, and hard. Shaped
like needles, colors vary from gray to white
Causes: cystine-containing crystals appear in the urine
Predisposing factors: acid urine
SIGNS AND SYMPTOMS
Costovertebral angle pain
Groin pain
Renal colic because renal stones
produce an increase in hydrostatic pressure and distention of the renal pelvis
and proximal ureters causing renal colic. Pain relief is immediate after stone
passage
Flank pain radiating to genitalia
Hematuria
Anuria
Restlessness
Pallor
Temperature
Nausea vomiting, diarrhea, abdominal
discomfort due to renointestinal reflexes
DIAGNOSTIC EVALUATION
History collection
Physical examination
Kidney radiography may show stone
IVP (intravenous pyelogram),
retrograde pyelogram is used to localize the degree and site of obstruction or
to confirm the presence of a radiolucent stones, such as uric acid or cystine
calculus
Urinalysis: may indicate gross or
microscopic hematuria and could indicate abrasion of the urinary tract
Ultrasonography can be used to
identify a radiopaque or radiolucent calculus in the renal pelvis, calyx, or
proximal ureters. But it is less useful when attempting to locate stones
trapped in the midureter
A CT scan may be used to
differentiate a non-opaque stone from the tumor
Lab test: serum calcium, phosphorus,
sodium, potassium, bicarbonate, uric acid, BUN and creatinine levels are also
measured
MANAGEMENT
Medical
Management
The goals of management are to
eradicate the stone, determine the stone type, prevent nephrons destruction,
control infection, and relieve any obstruction that may be present
The immediate objective of treatment
of renal colic is to relieve the pain until its cause can be eliminated
Opioid analgesic agents are
administered to prevent shock and syncope that may result from the excruciating
pain
Nonsteroidal anti-inflammatory drugs
(NSAIDs) are effective in treating renal stone pain because they provide
specific pain relief. They also inhibit the synthesis of prostaglandin E,
reducing swelling and facilitating passage of the stone
Hot baths or moist heat to the flank
areas may also be helpful
Nutritional
Therapy
Nutritional therapy plays an
important role in preventing renal stones
Fluid intake is the mainstay of most
medical therapy for renal stones
Patient with renal stones should
drink eight to ten ounce glasses of water daily or have IV fluids prescribed to
keep the urine dilute
A urine output exceeding 2 L/day is
advisable
International
Procedures
If the stone
does not pass spontaneously if complications occur, common intervention
includes endoscopic or other procedure. For example:
Ureteroscopy
Extracorporeal shock wave lithotripsy
(ESWL)
Endourologic (percutaneous) stone
removal
Ureteroscopy
It involves first visualizing the
stone and then destroying it
In this inserting an ureteroscope
into the ureter and then inserting a laser, electrohydraulic lithotripter, or
ultrasound device through the ureteroscope to fragment and remove the stones
Extracorporeal
shock wave lithotripsy
It is used for most symptomatic,
nonpassable upper urinary stones. Electromagnetically generated shock waves are
focused over the area of the renal stone
The high energy dry shock waves pass
through the skin and fragment the stone
Endourologic
(Percutaneous) stone removal
It is used for most symptomatic,
nonpassable, upper urinary stones. Electromagnetically generated shock waves
are focused over the area of the renal stone
The high energy dry shock waves pass
through the skin and fragment the stone
Endourologic
(Percutaneous) stone removal
It is used to treat the larger stones
A percutaneous tract is formed and a
nephroscope is inserted through it. Then the stone extracted or pulverized
Electrohydraulic
lithotripsy
It is a similar method in which an
electrical discharge is used to create a hydraulic shock wave to break up the
stone
A probe is passed through the
cystoscope and the tip of lithotripter
is placed near the stone
This procedure is performed under
topical anesthesia
The most common complications are
hemorrhage, infection and urinary extravasations
Chemolysis
Stone dissolution using infusions of
chemical solutions (e.g. alkylating agents, acidifying agents)
Surgical
Management
Today surgery is performed in only 1
to 2% of patients. It is indicated if the stone does not respond to other forms
of treatment
If the stone is in kidney, the
surgery performed maybe a nephrolithotomy (incision into the kidney with
removal of the stone) or a nephrectomy, if the kidney is nonfunctional
secondary to infection
Stones in the kidney pelvis are
removed by pyelolithotomy
COMPLICATION
Obstruction: from remaining stone
fragments
Infection: from dissemination of
infected stone particles or bacteria resulting from obstruction
Impaired renal function: from
prolonged obstruction before treatment and removal
Perirenal hematoma: from bleeding
around the kidney caused by trauma of shock waves or laser treatments
Nursing
Management
Nursing
Assessment
Obtain history focusing on family
history of calculi, episodes of dehydration, prolonged immobility, UTI,
dietary, bleeding history, and medication history
Assess pain location and radiation;
assess level of pain using a scale of 1 to 10. Observe for presence of
associated symptoms nausea, vomiting, diarrhea, abdominal distension
Monitor for signs and symptoms of
UTI, such as chills, fever, dysuria, frequency. Examine urine for hematuria
Observe for signs and symptoms of
obstruction, such as frequent urination of small amounts, oliguria, anuria
Nursing
Diagnosis
Acute pain related to the presence
of, obstruction or movement of a stone with in urinary system
Impaired urinary elimination related
to blockage of urine flow by stones
Risk for infection related to
obstruction of urine flow and instrumentation during treatment
Anxiety related to hospitalization
Fear related to deficient knowledge
regarding the disease
Deficient knowledge related to lack
of knowledge about prevention of recurrence, diet and symptoms of renal calculi
Acute pain related in the presence of
obstruction or movement of a stone with in urinary system
Interventions
Ask severity, location and duration
of pain using a pain scale. Pain is typically in the flank or costovertebral
angle and may radiate to the pelvic, groin, or abdominal area
Encourage fluid intake, unless
contraindicated, to promote the passage of stone, dilute the urine, and reduce
the risk of further stone formation
Administer pain medication as ordered
to promote comfort
Apply heat to flank pain area to
reduce pain and promote comfort
Impaired urinary elimination related
to blockage of urine flow by stones
Interventions
Monitor total urine output and
pattern of voiding. Report oliguria or anuria
For outpatient treatment, patient may
use a coffee filter to strain urine
Help patient to walk, if possible
because ambulation may help move the stone through the urinary tract
Teach patient to drink eight ounces
of liquid with meals, between meals and in early evening to provide fluids for
hydration but not to an excess that may increase renal colic
Risk for infection related to
obstruction of urine flow and instrumentation during treatment
Interventions
Administer parenteral or oral
antibiotics, as prescribed during treatment, and monitor for adverse effects
Assess urine for color, cloudiness,
and odor
Obtain vital signs, and monitor for
fever and symptoms of impending sepsis (tachycardia, hypotension)
Health
Education
Encourage fluids to accelerate
passing of stone particles
Teach about analgesics that still may
be necessary for colicky pain, which may accompany passage of stone debris
Warn that some blood may appear in
urine for several weeks
Encourage frequent walking to assist
in passage of stone fragments
Teach patient to strain urine through
a coffee filter or stone strainer and to save for analysis
Teach patient to take alpha-adrenergic
blockers to help dilate ureters, thus improve stone passage
NEPHROLITHIASIS – Etiology, Risk Factors, Pathophysiology, Types, Signs and Symptoms, Diagnostic Evaluation and Management
DIABETES MELLITUS – Types, Signs and Symptoms, Diagnostic Evaluation and Management
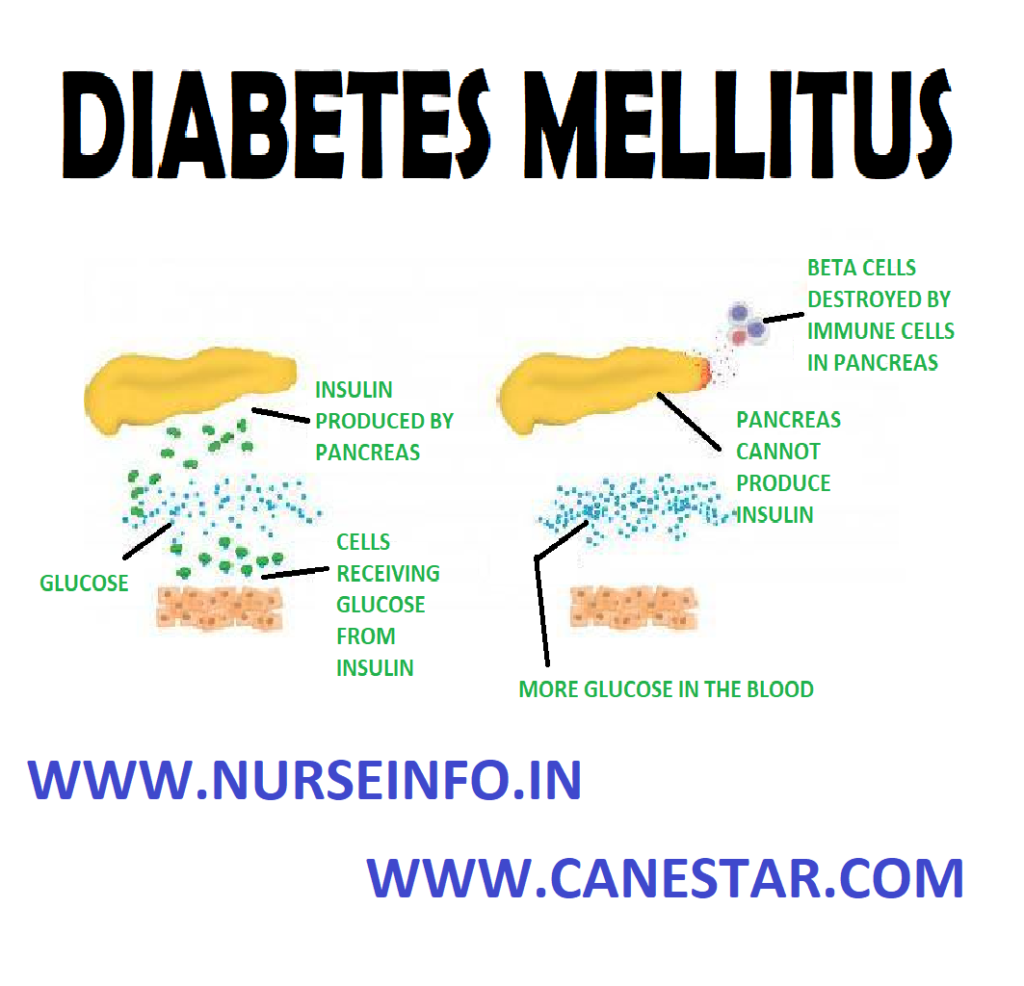
Diabetes
mellitus is a group of metabolic diseases in which a person has high blood
sugar, either because the pancreas does not produce enough insulin, or because
cells do not respond to the insulin that is produced. This high blood sugar
produces the classical symptoms of polyuria (frequent urination), polydipsia
(increased thirst) and polyphagia (increased hunger). Hyperglycemia does not
cause symptoms until glucose values are significantly elevated-above 200
milligrams per deciliter (mg/dL).
Diabetes mellitus
is a group of chronic disorder of endocrine pancreas. This disease
characterized by increased levels of glucose in blood (hyperglycemia) resulting
from defects in insulin secretion, insulin action, both.
There are three main types of diabetes mellitus (Type-1 DM)
TYPE-1 Diabetes Mellitus: Type 1 DM
results from the body’s failure to produce insulin, and currently requires the
person to inject insulin or wear an insulin pump. It is also called
‘insulin-dependent diabetes mellitus’ (IDDM) or ‘juvenile diabetes’. The immune
system mistakenly manufactures antibodies and inflammatory cells that are
directed against and cause damage to patients’ own body tissues. In persons
with type 1 diabetes, the beta cells of the pancreas, which are responsible for
insulin production, are attacked by the misdirected immune system. Exposure to
certain viral infections (mumps and coxsackie viruses) or other environmental
toxins may serve to trigger abnormal antibody responses that cause damage to
the pancreas cells where is made. Some of the antibodies seen in type 1
diabetes include anti-islet cell antibodies, anti-insulin antibodies and
anti-glutamic decarboxylase antibodies
TYPE-2 Diabetes mellitus: Type 2 DM
results from insulin resistance, also referred to as non-insulin-dependent
diabetes mellitus (NIDDM) or ‘adult-onset diabetes.’ In type 2 diabetes,
patients can still produce insulin, but do so relatively inadequately for their
body’s needs. In many cases the pancreas produces larger than normal quantities
of insulin. A major feature of type 2 diabetes is a lack of sensitivity to
insulin by the cells of the body (particularly fat and muscle cells)
Gestational diabetes: gestational
diabetes, occurs when pregnant women without a previous diagnosis of diabetes
develop a high blood glucose level. Gestational diabetes (or gestational
diabetes mellitus, GDM) is a condition in which women without previously
diagnosed diabetes exhibit high blood glucose levels during pregnancy
(especially during their third trimester)
SIGNS AND SYMPTOMS
Increased thirst (polydepsia)
Frequent urination (polyuria)
Increased hunger (polyphagia)
Weight loss
Fatigue
Blurred vision
Slow-healing sores or frequent
infections
Dark skin
DIAGNOSTIC EVALUATION
Glycated hemoglobin test: this blood
test indicates average blood sugar for the past two to three months. It
measures the percentage of blood sugar attached to hemoglobin, the
oxygen-carrying protein in red blood cells. A normal level is below 5.7 percent
Random blood sugar test: a blood sample
will be taken at a random time. Regardless of when you last ate, a random blood
sugar level of 200 mg/dL (11.1 mmmol/L) or higher suggests diabetes, a blood
sugar level less than 140 mg/dL (7.8 mmol/L) is normal.
Fasting blood sugar test: a blood sample
will be taken after an overnight fast. A fasting blood sugar level from 100 to
125 mg/dL (5.6 to 6.9 mmol/L) is considered prediabetes. If it is 126 mg/dL (7
mmol/L) or higher on two separate tests, indicates diabetes.
Oral glucose tolerance test: it is
rarely used test for hyperglycemia, patient is asked to fast overnight, and the
fasting blood sugar level is measured. Then drink a sugary liquid, and blood
sugar levels are tested periodically for the next two hours. A blood sugar
level less than 140 mg/dL (7.8 mmol/L) is normal. A reading of more than 200
mg/dL (11.1 mmol/L) after two hours indicates diabetes. A reading between 140
and 199 mg/dL (7.8 mmol/L and 11.0 mmol/L) indicates prediabetes.
Urine glucose and ketone levels:
these are not as accurate in monitoring, changes in blood glucose as serum or
blood levels. The presence of glucose in urine indicates hyperglycemia.
COMPLICATIONS
Cardiovascular disease
Nerve damage (neuropathy)
Kidney damage (nephropathy) or kidney
failure
Damage to the blood vessels of the
retina (diabetic retinopathy), potentially leading to blindness
Clouding of the normally clear lens
(cataract)
Feet problems caused by damaged
nerves or poor blood flow that can lead to serious infections
Bone and joint problems, such as
osteoporosis
Skin problems, including bacterial
infections, fungal infections and non healing wounds
Teeth and gum infections
Dawn phenomenon: It is rise of blood
glucose between 4 am to 8 am that is not a response to hypoglycemia. This
condition occurs in people both DM1 and DM2. Cause is unknown but due to
hormone variation.
Diabetic ketoacidosis: diabetic
ketoacidosis develops when there is too little insulin in body. Without enough
insulin, sugar cannot enter in cells for energy. Blood sugar level rises and
body begins to break down fat for energy. This process produces toxic acids
known as ketones. Excess ketones accumulate in the blood and eventually ‘spill
over’ into the urine. Diabetic ketoacidosis can lead to diabetic coma that can
be life-threatening.
Diabetic hyperosmolar syndrome: this
condition occurs when production of insulin is normal, but it does not work
properly. Blood glucose levels may become very high-greater than 600 mg/dL (33
mmol/L). Because insulin is present but not working properly, the body cannot
use either glucose or fat for energy. Glucose is then dumped in the urine,
causing increased urination. If left untreated, diabetic hyperosmolar syndrome
can lead to coma and life-threatening dehydration
MANAGEMENT
Nutritional
Therapy
Nutrition,
meal planning and weight control are the foundation of diabetes management.
The main
objective is to control dietary caloric intake to maintain normal weight.
Medical nutrition therapy (MNT), nutritional management of diabetes is complex,
a registered dietician who understand dietary management has major
responsibilities for designing and teaching aspect of therapeutic plan.
Regular
blood sugar monitoring
Regular
exercise
Regular
diabetes medication or insulin therapy
Alcohol:
alcohol and the substances use to make mixed drinks can cause either high or
low blood sugar
Stress: the
hormones body may produce in response to prolonged stress may prevent insulin
from working properly
For women, fluctuations
in hormone levels: as hormone levels fluctuate during menstrual cycle, so cans
blood sugar level also, particularly in the week before period. Menopause may
trigger fluctuations in blood sugar level as well
Some people
who have type 2 diabetes need insulin therapy as well. Because normal digestion
interferes with insulin taken by mouth, insulin must be injected. Insulin
injections involve using a fine needle and syringe or an insulin pen injector –
a device that looks like an ink pen, except the cartridge is filled with
insulin
Types of
insulin are many and include rapid-acting insulin, long-acting insulin and
intermediate options. Examples include:
Insulin lispro (Humalog)
Insulin aspart (Novolog)
Insulin glargine (Lantus)
Insulin detemir (Levemir)
Insulin isophane (Humulin N, Novolin
N)
Life Style
and Home Remedies
Commit to managing your diabetes:
Make healthy eating and physical activity part of your daily routine. Establish
a relationship with a diabetes educator, and ask your diabetes treatment team
for help when you need it
Wear a tag or bracelet that says you
have diabetes. Keep a glucagon kit nearby in case of a low blood sugar emergency
and make sure your friends and loved ones know how to use it.
Schedule a yearly physical exam and
regular eye exams
Keep your immunizations up-to-date.
Get a flu shot every year, and get a tetanus booster shot every 10 years
Take care of your teeth. Diabetes may
leave you prone to gum infections. Brush your teeth at least twice a day, floss
your teeth once a day, and schedule dental exams at least twice a year
Pay attention to your feet. Wash your
feet daily in lukewarm water. Dry them gently, especially between the toes and
moisturize with lotion. Check your feet everyday for blisters, cuts, sores,
redness or swelling
Keep your blood pressure and
cholesterol under control
Quit smoking
If you drink alcohol, do so
responsibly
Take stress seriously
NURSING MANAGEMENT
Nursing
Diagnosis
Fluid volume deficit related to
osmotic diuresis, gastric loss, excessive diarrhea, nausea and vomiting,
limited input
Intervention
Monitor vital signs, note the
presence of orthostatic blood pressure
Assess breathing and breathe patterns
Assess temperature, color and
moisture
Assess peripheral pulses, capillary
refill, skin turgor and mucous membranes
Monitor intake output. Record the
urine specific gravity
Measure body weight everyday
Collaboration fluid therapy as indicated
Imbalanced nutrition, less than body
requirements related to insulin insufficiency.
Intervention
Measure body weight per day as
indicated
Determine the diet program and diet
of patients compared with food that can be spent on the patient
Auscultation of bowel sounds, record
the presence of abdominal pain/abdominal bloating, nausea, vomiting, keep
fasting as indicated
Observation of the signs of
hypoglycemia, such as changes in level of consciousness, cold/humid, rapid
pulse, hunger and dizziness
Collaboration in the delivery of
insulin, blood sugar tests and diet.
Risk for infection related to
inadequate peripheral defense, changes in circulation and high blood sugar
levels
Intervention
Observation for signs of infection
and inflammation such as fever, redness, pus in the wound, purulent sputum,
urine color cloudy and foggy
Increase prevention efforts by
performing good handwashing, each contact on all items related to the patient,
including his or her own patients
Maintain aseptic technique in
invasive procedures(such as infusion catheter foley, etc)
Attach catheter/perineal care do well
Give skin care with regular and
earnest. Massage depressed bone area, keep skin dry, dry linen and tight (not
wrinkled)
Position the patient in semifowler
position
Collaboration antibiotics as
indicated
Knowledge deficit: About condition,
prognosis and treatment needs related to misinterpretation of information; do
not know the source of information
Intervention
Assess the level of knowledge of the
client and family about the disease
Give an explanation to the client
about diseases and conditions now
Encourage clients and families to pay
attention to her diet
Ask the client and reiterated family
of materials that have been given
DIABETES MELLITUS – Types, Signs and Symptoms, Diagnostic Evaluation and Management
GLOMERULONEPHRITIS – Etiology, Types,
Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
INTRODUCTION
Immunological
processes involving the urinary tract predominantly affect the renal
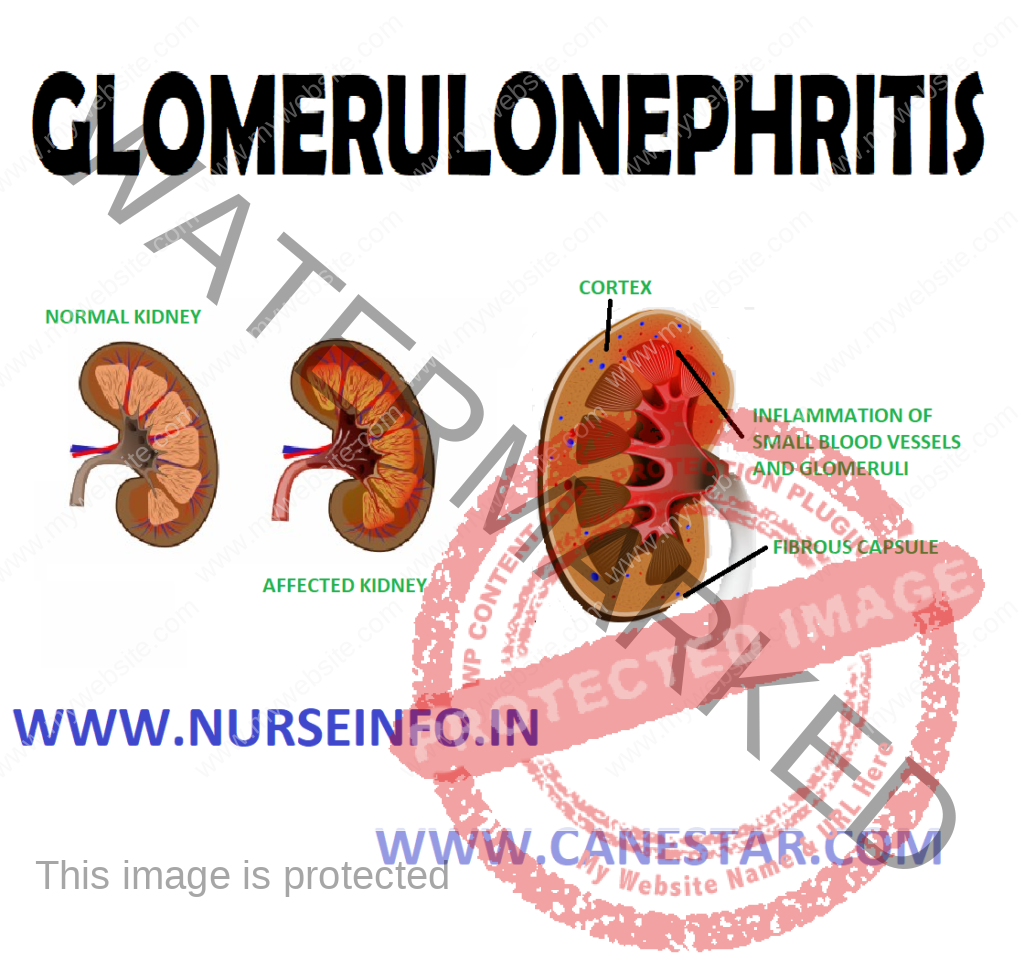
glomerulus, the disease process results in glomerulonephritis. It means
inflammation of glomeruli, which affects both kidneys equally. It is a type of
kidney disease in which the part of kidney (glomeruli) that helps in filter
waste and fluids from blood is damaged.
DEFINTION
Glomerulonephritis
means inflammation of glomeruli. It is an inflammation of tiny filters of
kidney (glomeruli) that helps to remove excess fluid, and waste from
bloodstream and pass them into the urine
TYPES
It is of two
types acute glomerulonephritis and chronic glomerulonephritis
ACUTE GLOMERULONEPHRITIS
It means
active inflammation in glomeruli. Acute glomerulonephritis is most common in
children and young adults, but all ages can be affected.
Each kidney
is composed of about 1 million filtering screens called glomeruli that remove
uremic waste products. The inflammatory process usually begins with the immune
system fights off the infection scars tissue forms
There are
many diseases that cause an active inflammation within glomeruli. When there is
active inflammation occur within the kidney scar tissue may replace normal
functional kidney tissue and cause irreversible renal impairment
ETIOLOGY
It is caused
when there is problem with immune system or diseases like HIV and lupus that
affect immune system. Disorders that attack several organs and can cause
glomerulonephritis
It occurs
after an infection elsewhere in the body or may develop secondary to systemic
disorders
An infection
with group A streptococci bacteria
PATHOPHYSIOLOGY
Due to
etiological factors, antigen (group A beta hemolytic streptococcus) —- throat
infection —- deposition of antigen antibody complex in glomerulus —- increased
production of epithelial cells lining the glomerulus —- leukocytes infiltrate
the glomerulus —- thickening of the glomerular filtration membrane —-
scarring and loss of glomerular filtration membrane —- decreased glomerular
filtration rate
SIGNS AND SYMPTOMS
The primary
presenting feature of acute glomerulonephritis is hematuria. The urine may be
cola, coffee colored because of RBCs and protein plugs
Proteinuria and elevated (BUN) blood
urea and nitrogen and serum creatinine
Other Manifestations
Oliguria
Edema fever
Shortness of breath or dyspnea.
Possible flank pain
Nausea and vomiting
Abdominal pain
Back pain, fatigue, weight gain
Headache, loss of appetite
Weakness, fatigue
High blood pressure
DIAGNOSTIC EVALUATION
History: assess and collect history
from patient regarding change in pattern of urination frequency, color or
volume
Ask patient for signs and symptoms like headache, nausea, vomiting and
loss of appetite
Ask for any history of flank pain
Physical examination: in physical examination assess for adequate intake
output
Check vital signs
Monitor weight of patient
Assess patient for edema and any signs and symptoms of infection
Urinalysis: for the presence of
hematuria. A urinalysis may show red blood cells in urine an indicator of
damage to the glomeruli. Urinalysis results may also show white blood cells, a
common indicator of infection and inflammation and increased protein which
results nephron damage.
Check patient BUN and serum
creatinine level. There is an increase in BUN and serum creatinine level
Needle biopsy: it reveals obstruction
of glomerular capillaries from proliferation of endothelial cells. It is a
diagnostic test that involves collecting small pieces of tissue, usually
through a needle, for examination with a microscope. In this we collect a
sample of kidney tissue, to check any unusual deposits, scarring, or infecting
organisms that would explain a person’s condition
MANAGEMENT
Management includes:
Antihypertensive’s to treat high blood pressure and diuretics, they
increase the renal blood flow by decreasing renal vascular resistance.
Provide antibiotics if infection is still present usually penicillin.
Helps to reduce infection and prevent further spread of infection
Steroids and other medicines will suppress the immune system.
Prednisolone and methylprednisolone is useful and most commonly prescribed
drug. It can suppress the inflammatory response in kidney and reduce the
permeability of renal blood vessels and reducing the proteinuria
Nutritional Therapy
Dietary protein should be restricted if BUN level is increased
Potassium and sodium should be avoided if edema is present
Dietary protein should be restricted if there is evidence of an increase
in nitrogenous wastes
Fluid intake should be restricted
Provide low protein diet to the patient
Provide vegetables, rice, cereals, dried beans, breads
Advise to avoid animal products they are rich source of protein
Eat healthy foods
Get proper rest and sleep
GLOMERULONEPHRITIS – Etiology, Types, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
CHRONIC GLOMERULONEPHRITIS –
Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and
Management
Chronic
glomerulonephritis is a kidney disorder caused by slow, cumulative damage and
scaring of tiny blood filters in the kidneys. These filters known as glomeruli,
remove waste products from the blood.
In
chronic glomerulonephritis, scarring of glomeruli impedes the filtering
process, trapping waste products in the blood while allowing red blood cells or
protein to escape into the urine, eventually producing the characteristic signs
of high blood pressure and swelling in legs and ankles
The disorder may first come to one’s
attention because of high blood pressure. In other, fluid retention or urine
may be first signs. Long-term inflammation and scarring of the kidneys may lead
to kidney failure in severe cases. Damage may progress without symptoms for months
or years by the months or year, by the time symptoms appear, the course of the
disorder maybe irreversible
ETIOLOGY
Specific
cause is unknown
Viral infections such as Hepatitis B,
C, HIV leads to chronic glomerulonephritis
Autoimmune disorder such as systemic
lupus erythematosus, vasculitis may cause chronic glomerulonephritis
Acute glomerulonephritis may after a
symptom less period of many years, reappear as chronic glomerulonephritis
PATHOPHYSIOLOGY
It is an
autoimmune disease caused by the loss of tolerance to self-antigens —-
glomeruli have varying degree of hypercellularity and become sclerosed
(hardened) —- size of kidney is decreases, and eventually tubular atrophy,
chronic interstitial inflammation occur —- kidney’s ability to regulate the
internal environment begins to decrease as glomeruli become scarred and
resulting in fewer functional nephrons —- results into various symptoms of
renal dysfunction that leads to edema, weight loss, irritability, poorly
nourished, high blood pressure, nocturia
SIGNS AND SYMPTOMS
Patient with
severe disease has no symptoms at all for many years. There condition may be
detected when BUN level and serum creatinine level are detected
Blood or protein in the urine
Swelling of legs or ankle and other
parts of body due to fluid accumulation (edema)
Shortness of breath due to less blood
Headache or blood pressure high
Fatigue, nausea, vomiting, loss of
appetite, abdominal pain
Nocturia (increased need to urinate
at night)
Crackles sound in the lungs, poorly
nourished, pale skin color
DIAGNOSTIC EVALUATION
History: collect any history of acute
glomerulonephritis if present
Ask patient for the history of urination changes in patient
Ask for the presence of signs and symptoms
Ask patient for history of abdominal pain, etc
Physical examination: assess patient for edema and swelling, check
patient body weight
Monitor patient blood pressure
Urinalysis and blood tests to know
about the elevated level of for the presence of hematuria. A urinalysis may
show red blood cells in urine an indicator of damage to the glomeruli.
Urinalysis results may also show white blood cells, a common indicator of
infection and inflammation and increased protein which results nephron damage
A blood test to measure protein and
creatinine level. Level of creatinine and protein is elevated
An ultrasound of kidneys maybe
performed to evaluate the size of kidneys and any blockages
CT scan or abdominal ultrasound can
be performed to show the damage to the glomeruli
Renal biopsy maybe performed, under
local anesthesia, to extract a small sample of tissue from kidney, to determine
the exact cause and the nature of the glomerulonephritis
MANAGEMENT
Antihypertensive drugs (propranol)
maybe prescribed to reduce high blood pressure
Diuretics (frusemide) may be
prescribed to reduce excess fluid retention and increase urine production
Steroid medications, if
immunosuppressive drugs (prednisolone and methyl prednisolone), maybe
prescribed for some patients. Prednisolone and methylprednisolone is useful and
most commonly prescribed drug. It can suppress the inflammatory response in
kidney and reduce the permeability of renal blood vessels and reducing the
proteinuria
In severe cases, where kidney failure
occurs, dialysis maybe necessary. Dialysis performs the function of the kidney
by removing waste products and excess fluid from the blood when kidney cannot
A kidney transplant is also an
alternative in case of kidney failure. A kidney transplant is a surgical procedure
performed to replace a diseases kidney with a healthy kidney from another
person
DIET MANAGEMENT
Provide low salt diet and provide low
protein diet, because it reduces the workload on the kidney
Nuts, dried beans, cereals,
vegetables, rice, breads are low in protein
Limit the amount of animal products
Take vitamin supplements
Fluid intake should be restricted
Provide adequate diet and fruits
Get proper rest
Take medication regularly
PREVENTION
In prevention it can be prevented by
limit the salts, fluids, protein
Control blood pressure, controlling
high blood pressure is the most important part of treatment
Maintain good hygiene practices
Practicing safe sex helps in
preventing the viral infection such as HIV infection and hepatitis which leads
to this illness
Take calcium supplements
NURSING MANAGEMENT
Nursing
Assessment
Observe patient for changes in fluid
and electrolyte status and for the signs and symptoms
Monitor vital signs of patient blood
pressure
Anxiety levels are often extremely
high for both the patient and family
Throughout the course of disease and
treatment, the nurse should gives emotional support by providing opportunities
for the patient and family to verbalize their concerns, have their questions
answered, and explore their options
Nursing
Diagnosis
Ineffective renal tissue perfusion
related to damage of glomerular infiltration
Excess fluid volume related to
compromised renal function
Imbalanced nutrition less than body
requirement related to anorexia, nausea, vomiting
Deficient knowledge regarding
condition and treatment
Activity intolerance related to
fatigue, retention of waste products
Excess fluid volume related to
compromised renal function, decreased urine output, retention of sodium and
water
Interventions
Assess the fluid status of patient
Check weight daily and record
Maintain intake output chart
Monitor vital signs
Limit fluid intake to the patient
Explain the rationale for restriction
of fluid
Assist patient to cope up with the
discomforts results from fluid restriction
Provide and encourage oral hygiene,
it minimizes the dryness of oral membranes
Imbalanced nutrition pattern less
than body requirements related to anorexia, nausea, vomiting
Interventions
Assess the nutritional status of the
patient
Monitor weight of patient daily and
record it
Assess the patient nutritional
dietary patterns-diet history, food preferences
Provide patients food preference within
dietary restrictions
Provide low salt and protein diet
Restrict fluids rich diet to the
patient
Encourage for proper rest
Provide pleasant surroundings at the
meal time
Deficient knowledge related to
disease condition and treatment
Interventions
Assess the understanding of patient
regarding disease condition and treatment
Provide explanation regarding renal
function and consequences of disturbed renal function at the level of patient
understanding and guided by patient’s readiness to learn
Assist patient to identify ways to
incorporate changes related to illness and its treatment into lifestyle
Provide oral and written information
as appropriate about: renal function, fluid and dietary restrictions
Clear all the doubts of the patient
Provide psychological support to the
patient
CHRONIC GLOMERULONEPHRITIS – Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
The most
important function of the respiratory system is to provide oxygen to the body
tissues and remove the carbon dioxide. The body relies primarily on the central
nervous system, the pulmonary system, the heart, and the vascular system to
accomplish the effective respiration. Respiratory failure develops when one or
more of these systems or organs fail to maintain optimal functioning.
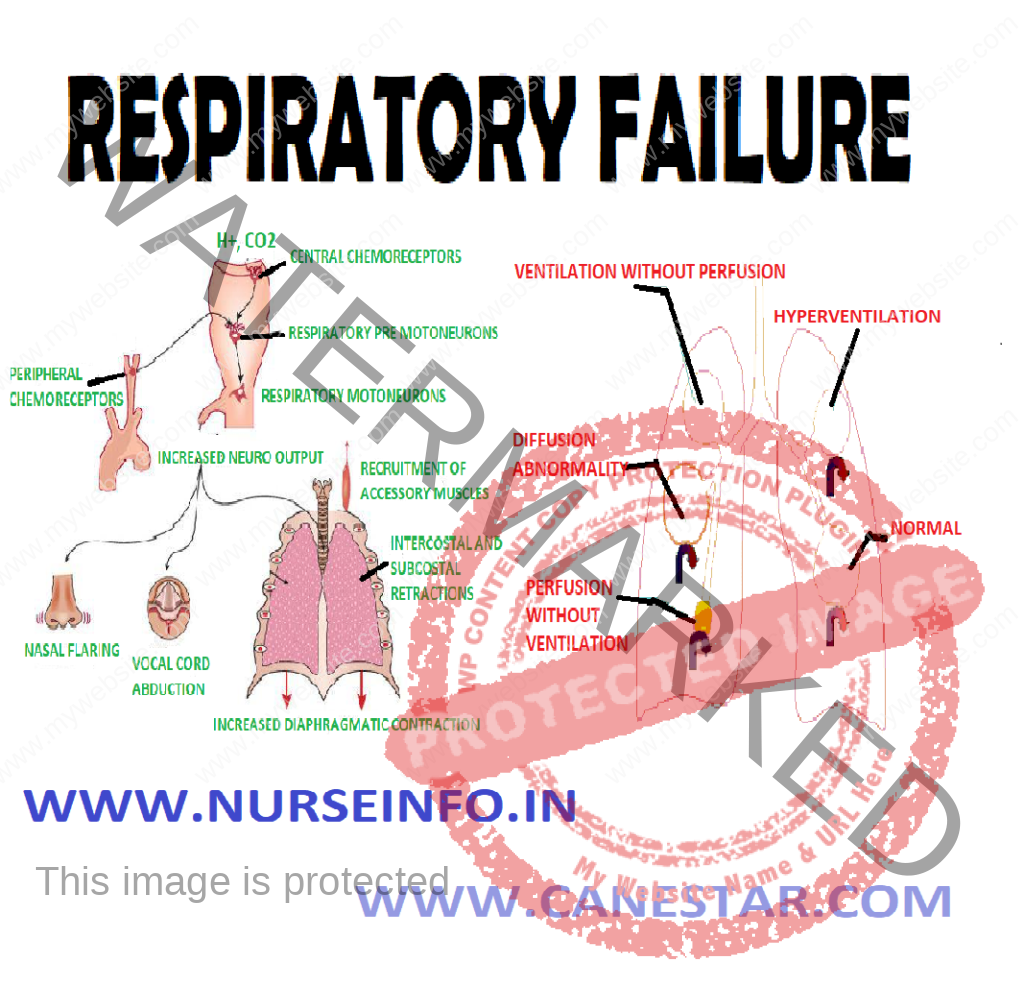
Respiratory
failure is a sudden and life-threatening deterioration of the gas exchange
functions of the lung and indicates failure of the lungs to provide adequate
oxygenation or ventilation for the blood. Acute respiratory failure is defined
as the decrease in the arterial oxygen tension to less than 50 mm Hg
(hypoxemia) and increase in the arterial carbon dioxide tension, i.e.
(hypercapina) to greater than 50 mm Hg, with the arterial pH of less than 7.35.
it is a condition in which there is inadequate gas exchange by the respiratory
system, with the result that arterial O2 and CO2 levels
cannot be maintained within their normal ranges.
DEFINITION
Acute respiratory failure is a
condition in which the patient’s breathing apparatus fails in the ability to
maintain arterial blood gases within the normal range.
Ventilatory failure is the inability
of the body to sustain respiratory drive or the inability of the chest wall and
muscles to mechanically move air in and out of the lungs. The hallmark of
ventilator failure is an elevated CO2 level.
A sudden inability of the lungs to
maintain normal respiratory function. The condition may be caused by an
obstruction in the airways or by failure of the lungs to exchange gases in the
alveoli.
Acute respiratory failure is defined
as the decrease in the arterial oxygen tension to less than 50 mm Hg
(hypoxemia) and increase in the arterial carbon dioxide tension, i.e.
(hypercapnia) to greater than 50 mm Hg, with an arterial pH of less than 7.35.
CLASSIFICATION OF RESPIRATORY FAILURE
It is
divided into two types:
Acute respiratory failure
Chronic respiratory failure
Acute
Respiratory Failure
Acute
respiratory failure is characterized by hypoxemia (PaO2 less than 50
mm Hg) and academia (pH less than 7.35). acute respiratory failure occurs
rapidly, usually in minutes to hours or days
Types of
Acute Respiratory Failure
It is
divided into two:
Type 1 acute respiratory failure
Type 2 acute respiratory failure
Type 1 acute respiratory failure:
Type 1 respiratory failure is defined as hypoxia without hypercapnia and indeed
the PaCO2 may be normal or low. It is typically caused by a ventilation/perfusion
(V/Q) mismatch, the volume of air flowing in and out of the lungs is not
matched with the flow of blood to the lungs.
Type 2 acute respiratory failure:
Type 2 respiratory failure is caused by inadequate ventilation, both oxygen and
carbon dioxide are affected and buildup of carbon dioxide levels (PaCO2)
that has been generated by the body.
Chronic
Respiratory Failure
Chronic
respiratory failure is characterized by hypoxemia and hypercapnea with the
normal pH (7.35 to 7.45). chronic respiratory failure occurs over a period of
months to a year – allows for activation of compensatory mechanism.
Chronic
respiratory failure may also be divided into:
Hypoxemic respiratory failure: when a
lung disease causes respiratory failure, gas exchange is reduced because of
changes in ventilation (the exchange of air between the lungs and the
atmosphere), perfusion (blood flow), or both. Activity of the respiratory
muscles is normal. This type of respiratory failure which results from a
mismatch between ventilation and perfusion is called hypoxemic respiratory
failure. Some of the alveoli get less fresh air than they need for the amount
of blood flow, with the net result of a fall in oxygen in the blood. These
patients tend to have more difficulty with the transport of oxygen than with
removing carbon dioxide. They often overbreathe (hyperventilate) to make up for
the low oxygen, and this results in a low CO2 level in the blood
(hypocapnia). Hypocapnia makes the blood more basic or alkaline which is
injurious to the cells.
Hypercapnic respiratory failure:
respiratory failure due to a disease of the muscles used for breathing (‘pump
or ventilatory apparatus failure’) is called hypercapnic respiratory failure.
The lungs of these patients are normal. This type of respiratory failure occurs
in patients with neuromuscular diseases, such as myasthenia gravis, stroke,
cerebral palsy, poliomyelitis, amylotrophic lateral sclerosis, muscular
dystrophy, postoperative situations limiting ability to take deep breaths, and
in depressant drug overdoses. Each of these disorders involves a loss or
decrease in neuromuscular function, inefficient breathing and limitation to the
flow of air into the lungs. Blood oxygen falls and the carbon dioxide increases
because fresh air is not brought into the alveoli is needed amounts. In
general, mechanical devices that help move the chest wall help these patients.
ETIOLOGY
Brain
Disorders
Stroke: a stroke is sudden loss of
brain function resulting from a disruption of blood supply to a part of the
brain
Brain tumors: a brain tumor is a
localized intracranial lesion that occupies space within the skull and tends to
cause a rise in intracranial pressure
Depression of respiratory drive with
drugs, e.g. narcotic tranquilizer
Chest Wall
Dysfunction and Neuromuscular Factor
Anesthetic blocking agent
Cervical spinal cord injury
Neuromuscular disorder
Neuromuscular blocking agent
Airway
Obstruction
Airway inflammation
Tumor
Foreign bodies
Asthma
COPD
Interstitial
Lung Diseases
Pneumonia
Pulmonary tuberculosis
Pulmonary edema
Pulmonary fibrosis
Pulmonary
Dysfunction
Asthma
Emphysema
Chronic obstructive pulmonary disease
Pneumonia
Pneumothorax
Pulmonary contusion
Hemothorax
Acute respiratory distress syndrome
(ARDS)
Cardiac
Dysfunction
Pulmonary edema
Cerebrovascular accident
Arrhythmia
Congestive heart failure
Valve pathology
Other
Fatigue due to prolonged tachypnea in
metabolic acidosis
Intoxication with drugs (e.g.
morphine, benzodiazepines, alcohol) that suppress respiration.
Traumatic
Causes
Direct thoracic injury may result in
a number of abnormalities that can lead to respiratory failure
Direct brain injury can result in
loss of respiration
PATHOPHYSIOLOGY
In alveolar
ventilation —- nerves and muscles of respiration drive breathing —- failure
in alveolar ventilation —- ventilation-perfusion mismatch —- hypercapnia
and acidosis during obstructive forms: the residual pressure in the chest
impairs inhalation —- increase in workload of breathing —- develops true
intrapulmonary shunt —- decreased lung compliance
Mechanism of
Pathophysiology
Respiratory failure can arise from an
abnormality in any of the components of the respiratory system, including the
airways, alveoli, central nervous system (CNS), peripheral nervous system,
respiratory acidosis, and chest wall. Patients who have hypoperfusion secondary
to cardiogenic, hypovolemic, or septic shock often present with respiratory
failure
Ventilatory capacity is the maximal
spontaneous ventilation that can be maintained without development of
respiratory muscle fatigue. Ventilatory demand is the spontaneous minute
ventilation that results in a stable PaCO.
Normally, ventilatory capacity
greatly exceeds ventilatory demand. Respiratory failure may result from either
a reduction in ventilatory capacity or an increase in ventilatory demand (or
both). Ventilatory capacity can be decreased by a disease process involving any
of the functional components of the respiratory system and its controller.
CLINICAL MANIFESTATIONS
Paroxysmal nocturnal dyspnea
Orthopnea
Pulmonary edema
Confusion and reduced consciousness
may occur
Neurological features may include
restlessness, anxiety, confusion, seizures or coma
Tachycardia and cardiac arrhythmias
Cyanosis
Polycythemia
Cor pulmonale
Pulmonary hypertension
Right ventricular failure
Hepatomegaly
Peripheral edema
DIAGNOSTIC EVALUATION
Arterial blood gas analysis:
confirmation of the diagnosis
Renal function tests and LFTs: may
provide clues to the etiology or identify complications associated with
respiratory failure. Abnormalities in electrolytes such as potassium, magnesium
and phosphate may aggravate respiratory failure and other organ dysfunctions
Serum creatine kinase and troponin I:
to help exclude recent myocardial infarction. Elevated creatine kinase may also
indicate myositis
Thyroid function test: hypothyroidism
may cause chronic hypercapnic respiratory failure
Spirometry: to evaluate lung capacity
Echocardiography: if a cardiac cause
of acute respiratory failure is suspected
Pulmonary function tests are useful
in the evaluation of chronic respiratory failure
ECG: to evaluate a cardiovascular
cause, it may also detect dysrhythmias resulting from severe hypoxemia or
acidosis.
Right heart catheterization: should
be considered if there is uncertainty about cardiac function, adequacy of
volume replacement, and systemic oxygen delivery
Pulmonary capillary wedge pressure
may be helpful in distinguishing cardiogenic from noncardiogenic edema
MANAGEMENT
Management
of acute respiratory failure is dependent upon the cause and its severity. The principle
of management of acute respiratory failure is the following:
Treat the cause
Maintain a patient airway
Provide adequate ventilation
Provide optimum oxygen
Carry out chest physiotherapy
The main goal of treating of respiratory failure is to get oxygen to
lungs and organs and remove the carbon dioxide from the body
The promoting effective airway clearance effective gas exchange
Preventive complication of immobility
Monitoring and documenting indication of altered tissue perfusion
Promoting comfort
Correction of hypoxemia
Correction of hypercapnia
Airway an another goal is to treat the underlying cause of the condition
Administration
of Oxygen
Nasal
prongs, nasal catheters, or face masks are commonly used to administer oxygen
to the spontaneously breathing patient
The actual
fraction of inspired oxygen depends upon:
Flow rate of oxygen
Degree of mouth breathing
Patency of nasal passage
Inspection of insertion of nasal
catheter
Positive End
Expiratory Pressure (PEEP)
Used with mechanical ventilation
Increases interthoracic pressure
Keeps the alveoli open
Decreases shunting
Improves gas exchange
Management
of Upper Airway Obstruction
As soon as
upper airway obstruction is diagnosed, measures must be taken to correct it.
The mouth is opened to see if tongue
has fallen back or if there are secretions, blood clot or any particles
obstructing the airway
Extension of the head is the simplest
way of relieving upper airway obstruction by the tongue falling back
If simple extension of the head is
not adequate to clear the airway, the mandible should be forced forward
Maneuver is designed to put further
tension on the musculature that supports the tongue. It is best executed by
standing behind the patient
If maneuver is not adequate and
partial airway obstruction still exists, then oral airway may have to be
inserted or end tracheal intubation be done
If assisted ventilation is required,
a resuscitator bag and mask are used initially prior to intubation and
mechanical ventilation
Medical
Management
Medical
management includes:
Antibiotics for pneumonia infection
Bronchodilators: reduce bronchospasm,
COPD
Diuretics for pulmonary edema
Chest physical therapy and the
hydration to mobilize secretions
Maintain fluid and electrolytes and
avoid fluid overload
Intubation and mechanical ventilation
COMPLICATIONS
Oxygen toxicity if prolonged high FIO2
required
Barotrauma may occur from excessive
intra-alveolar pressure
Ventilator-associated pneumonia
Infection to the lower respiratory
tract due to intubation
Dental or vocal cord trauma
Gastric complications: distension
from air entering the GI tract, stress ulcers from hyperacidity and inadequate
nutrition
Other complications include deep
venous thromboembolism, skin breakdown, malnutrition, stress and anxiety
NURSING MANAGEMENT
Nursing
Assessment
Note the changes suggesting increased
work of breathing or pulmonary edema
Assess breathing sound
Assess sign of hypoxemia and
hypercapnea
Analyze the ABG and compare the
previous values
Determine hemodynamic status and
compare it with previous value
Nursing
Diagnosis
Impaired gas exchange related to
inadequate respiratory center activity or chest wall movement, airway
obstruction, or fluid in lung
Ineffective airway clearance related
to increased or tenacious secretion
Acute pain related to inflammatory
process and dyspnea
Anxiety related to pain, dyspnea and
serious conditions
Nursing
Intervention
Improve gas exchange:
Administer oxygen to maintain PaO2 of 60 mm Hg, using devices
that provide increased oxygen concentration
Monitor fluid balance by intake and output measurement, urine-specific
gravity, daily weight measurement
Provide measures to prevent atelectasis and promote chest extension and
secretion clearance as per advice, spirometer
Elevated head level to 30 degrees
Monitor adequacy of alveolar ventilation by frequent measurement of
respiratory system
Administer antibiotic, cardiac medication and diuretics as prescribed by
doctor
Maintain airway clearance:
Administer medication to increase alveolar function
Perform chest physiotherapy to remove mucus
Administer IV fluids
Suction patient as needed to assist with removal of secretions
Relieving pain:
Watch patient for sign of discomfort and pain
Position the head elevated
Give prescribed morphine and monitor for pain-relieving sign
Reducing anxiety:
Correct dyspnea and relieve from physical discomfort
REHABILITATION OF DISASTER VICTIMS –
Challenges of Rehabilitation, Kinds of Reactions and Psychosocial Interventions
In the
post-disaster period, along with relief, rehabilitation and the care of
physical health and injuries, mental health issues need to be given importance.
Apart from material and logistic help, the suffering human beings will require
human interventions.
CHALLENGES OF REHABILITATION
Ensuring that people living in the
relief camps have access to regular food supplies, additional set of clothes,
sanitation drinking water, public health intervention immunization, preventive
health care, heat and rain proof shelters, child care and education facilities
and support.
Ensuring access to basic entitlements
in terms of their compensation, government schemes and credit institutions so
that they can rebuild their homes and livelihood back to the same levels as before
the disaster.
Ensuring livelihood reintegration
Ensuring legal right and social
justice to the disaster victims including filing of FIRs, investigation and
contesting cases in the court
Providing psychosocial counseling and
support for dealing with loss, betrayal and anger.
Community based rehabilitation for
widows orphans, elderly, children and physically disabled
Actively rebuilding a culture of
communal harmony and trust
KINDS OF REACTIONS SHOWN BY DISASTER VICTIMS
Physical impact: stomach aches,
diarrhea, headaches, and body aches, physical impairments (limbs, sight, voice,
hearing), injuries, fever, cough, cold, miscarriage etc.
Emotional reactions: anger, betrayal,
irritability, revenge-seeking, fear, anxiety, depression, withdrawal, grief,
addiction to pan masala, cigarette, beedi, drug abuse (flask back, numbness,
depression)
Socioeconomic impact: loss of trust
between communities, lack of privacy, single parent families, widows, orphan
state with loss of both parents, discontinuity in educational plans (e.g. loss
of employment, homelessness migration, disorganization of life routines, material
loss).
PSYCHOSOCIAL INTERVENTIONS
Principles
Ventilation
Empathy
Active listening
Social support
Externalization of interest
Lifestyle choice
Relaxation and recreation
Spirituality
Health care
Work with individuals (willing to
talk immediately unwilling to talk)
For people who are willing to talk immediately
Listen attentively
Do not interrupt
Acknowledge that you understand the pain and distress by learning forward
Look into the eyes
Console them by patting on the shoulders or touching or holding their
hand as they cry
Respect the silence during interaction; do not try to fill it in by talking
Keep reminding them I am with you. It is good you are trying to release
your distress by crying. It will make you feel better
Do not ask them to stop crying
For those
unwilling to talk (angry, or remain mute and silent)
Do not get
anxious or feel rejected, remain calm
Maintain
regular contact and greet them
Maintain
interaction
Acknowledge
that you understand they are not to blame
Tell them
you will return the next day or in a couple of days
Tell them
you are not upset or angry because he or she did not talk
Once the
person starts talking, maintain a conversation using the following queries like
how you are and how are your other family members, what can individuals do to
recover?
Work with
Families
Share their experience of loss as a
family
Contact relatives to mobilize support
and facilitate recovery
Participate in rituals like prayers,
keeping the dead persons photographs
Make time for recreation
Resume normal activities of the
pre-disaster days with the family
Try and do things together as a writ
and support one another
Be together as a family member. Do
not send women and children and the aged too far off places for the sake of
safety
Restart activities that are special
to your family like having meals together, praying, playing games, etc
Keep touching and comforting your
parents, children, spouse and the aged in your family
Keep in constant touch with the
family member who is hospitalized
Work with
the Community
Group mourning
Group meetings
Supporting group initiatives
Cultural aspects
Rally
Group participation for rebuilding
efforts
Sensitization process
Rehabilitation
of Special Groups
Aged people can be helped by
Keeping them with their near and dear
ones
Visiting them regularly and spending
time with them
Touching them and allowing them to
cry
Re-establishing their daily routines
Making them feel responsible by
giving them some work to carry out which is not too difficult
Getting them involved in relief work
by requesting for their suggestion and advice, etc.
Keeping them informed of positive
news
Attending to their medical ailments
Organizing small group prayer
meetings
Disabled
People
Removing them to places of safety
Keeping them informed what is
happening
Getting them involved in activities
Integrate them in group discussions
Attend to their specific needs (wheel
chairs, hearing aids)
Helping them overcome their feeling
of insecurity
Taking cognizance of the fact that
mentally challenged people, especially the women and children are vulnerable to
sexual abuse and help them
Women
Help them to be with their families
Keep informing them what is happening
Involve them in activities
Involving them in relief and
rehabilitation activities
Initiating self-help formation
Involve them in recreation
Making them to spend time with young
widows or people who have lost their children and supporting them
Children
Letting him/her to be close to adults
who are loved and familiar
Re-establishing some sort of a
routine for them like eating, sleeping, going for programs
Actions like touching, hugging,
reassuring them verbally
Allowing them to take about the event
Encourage them to play
Involve them in activities like
painting and drawing, where then can express their emotions
Organize story telling sessions,
singing, songs and games
Praising coping behavior
Provide referral if required
Spending time on their studies once
they return to school
Policies
Related to Emergency and Disaster Management
This policy
aims at:
Promoting a culture of prevention,
preparedness and resilience at all levels through knowledge, innovation and
education
Encouraging mitigation measures based
on technology, traditional wisdom and environmental sustainability
Mainstreaming disaster management
into the developmental planning process
Establishing institutional and
technological frameworks to create an enabling regulatory environment and a
compliance regime
Ensuring efficient mechanism for
identification, assessment and monitoring of disaster risks
Developing contemporary forecasting
and early warning systems backed by responsive and fail-safe communication with
information technology support
Ensuring efficient response and
relief with a caring approach towards the needs of the vulnerable sections of
the society
Undertaking reconstruction as an
opportunity to build disaster resilient structures and habitat for ensuring
safer living and
Promoting a productive and protective
partnership with the media for disaster management
Policy
Statement
To develop
and implement an integrated action plan that will create an effective disaster
management system at local, national and international levels.
Focus Areas
and Strategies for Intervention
Making disaster risk reduction a
development priority:
To incorporate disaster risk principles in the development agenda and
other country programme
To enhance institutional capacity in disaster risk reduction
To develop national platforms for disaster risk reduction
Improving early warning systems:
To monitor continuously the hazard and vulnerability threats
To develop standard risk and monitoring instruments
Do a risk and hazard mapping
To foster an understanding of disaster management mechanisms through
dissemination of information and advocacy
Addressing priority development
concerns to reduce underlying risk factors:
To integrate disaster risk reduction in poverty reduction strategy paper
To address sources of vulnerability especially outbreak of diseases and
pests (HIV/AIDS, Avian Flu, locusts, etc)
To sensitize both local and traditional authorities with a view to
understanding disaster prevention as a development challenge
Mainstream gender and youth policies in the development agenda
Effective disaster response through
disaster preparedness:
To promote contingency planning in all government departments
and all other sectors to ensure alignment of national, local and district
disaster management plans
To review and periodically rehearse national preparedness and
contingency plans for major hazards
To ensure that operational capacity exists within disaster
management systems to enhance community resilience
Policy
Implementation Agencies and Structures
The policy
will adopt various approaches to ensure that risk reduction in particular and
disaster management in general is a national and local priority with strong
involvement of local actors, the victims of disaster and institutional basis
for implementation
Agencies
NGOs
Civil Society Organizations
Government Agencies
UN Agencies
Private Sector
Functions
Identify, assess and monitor disaster
risks and enhance early warning systems
Use indigenous knowledge, innovation,
practices and education to build a culture a safety and resilience at all
levels
Strengthen disaster preparedness for
effective response at all levels
Creation of Disaster Prevention
Volunteer Corps at local and national levels to be fully trained and equipped
to identify, assess and monitor disaster events
Operational
Mechanism
This policy
will be implemented through the following strategic actions:
Sensitization programmes and advocacy
on disaster prevention
Mainstreaming disaster prevention and
management in school curricula and development programmes
Factor disaster scenarios into
economic planning and programmes
Capacity building and information
sharing
Monitoring and Evaluation
REHABILITATION OF DISASTER VICTIMS – Challenges of Rehabilitation, Kinds of Reactions and Psychosocial Interventions
EMERGENCY CONDITIONS – Shock
(Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and
Management)
SHOCK
Clinical
syndrome characterized by decreased tissue perfusion and impaired cellular
metabolism resulting in an imbalance between the supply and demand for oxygen
and nutrients
ETIOLOGY AND PATHOPHYSIOLOGY
Cardiogenic shock occurs when either
systolic or diastolic dysfunction of the pumping action of the heart results in
compromised cardiac output (CO).
Precipitating causes of cardiogenic shock include myocardial infarction
(MI), cardiomyopathy, blunt cardiac injury, severe systemic or pulmonary
hypertension, cardiac tamponade, and myocardial depression from metabolic
problems.
Hemodynamic profile will demonstrate an increase in the pulmonary artery
wedge pressure (PAWP) and pulmonary vascular resistance
SIGNS AND SYMPTOMS
Tachycardia, hypotension, a narrowed pulse pressure, tachypnea, pulmonary
congestion, cyanosis, pallor, cool and clammy skin, decreased capillary refill
time, anxiety, confusion, and agitation.
Hypovolemic shock occurs when there
is a loss of intravascular fluid volume
Absolute hypovolemia results when fluid is lost through hemorrhage,
gastrointestinal (GI) loss (e.g. vomiting, diarrhea), fistula drainage,
diabetes insipidus, hyperglycemia, or diuresis.
Relative hypovolemia results when fluid volume moves out of the vascular
space into extravascular space (e.g., interstitial or intracavitary space) and
this is called third spacing
The physiologic consequences of hypovolemia include a decrease in venous
return, preload, stroke volume and CO resulting in decreased tissue perfusion and
impaired cellular metabolism.
Clinical manifestations depend on the extent of injury or insult, age and
general state of health and may include anxiety, an increase in heart rate, CO,
and respiratory rate and depth, and a decrease in stroke volume, PAWP, and
urine output.
Neurogenic shock is a hemodynamic
phenomenon that can occur within 30 minutes of a spinal cord injury at the
fifth thoracic (T5) vertebra or above an last up to 6 weeks, or in response to
spinal anesthesia.
Immediate reaction causes massive vasodilation, release of
vasoactive mediators, and an increase in capillary permeability resulting in
fluid leaks from the vascular space into the interstitial space
Clinical manifestations can include anxiety, confusion,
dizziness, chest pain, incontinence, swelling of the lips and tongue, wheezing,
stridor, flushing, pruritus, urticaria and angioedema.
Septic shock is the presence of
sepsis with hypotension despite fluid resuscitation along with the presence of
tissue perfusion abnormalities
In severe sepsis and septic shock, the initiated body response to an
antigen is exaggerated resulting in an increase in inflammation and
coagulation, and a decrease in fibrinolysis
Endotoxins from the microorganisms cell wall stimulate the release of
cytokines and other proinflammatory mediators that act through secondary
mediators such as platelet-activating factor.
Clinical presentation for sepsis is complex. Patients will usually
experience a hyperdynamic state characterized by increased CO. Persistence of a high CO beyond 24 hours is ominous and
often associated with hypotension and multiple organ dysfunction syndrome
(MODS). Initially patients will hyperventilate as a compensatory mechanism,
resulting in respiratory alkalosis followed by respiratory acidosis and
respiratory failure. Other clinical signs include alteration in neurologic
status, decreased urine output, and GI dysfunction.
STAGES OF SHOCK
Compensatory Stage
Decrease in circulating blood volume
Sympathetic nervous system stimulated, release catecholamines
(epinephrine and norepinephrine), bronchodilation and increased cardiac output
occurs. To maintain blood pressure; increase heart rate and contractility
increases in peripheral vasoconstriction due to stimulation of beta adrenergic fibers
(cause vasoconstriction of blood vessels of skin and abdominal viscera) and
increase in heart rate and contractility.
Renin-angiotensin release of aldosterone-reabsorb H2O and
sodium. Get fluid shift from interstitial to capillaries due to decrease in
hydrostatic pressure in capillaries
Shunting blood from the lungs-ventilation-perfusion mismatch
Circulation maintained, but only sustained short time without harm to
tissues
Progressive Stage
Altered capillary permeability (3rd spacing)
In the lungs: alveolar or pulmonary edema, ARDS, increased pulmonary
artery pressures
Cardiac output decreases and coronary perfusion is decreased. Decreased
myocardial perfusion-arrhythmias and myocardial ischemia
Kidneys: elevated BUN and creatinine
Metabolic acidosis, anaerobic metabolism and kidneys cannot excrete acids
and reabsorb bicarbonate
GI-ischemia causes ulcers and GI bleed
Liver: cannot eliminate waste products, elevated ammonia and lactate,
bilirubin (jaundice) bacteria released in bloodstream
Increased capillary blood leak, worsens hypotension and tachycardia, also
get cerebral ischemia
Get profound hypotension and hypoxemia
Cellular death leads, tissue, death, vital organs fail and death occurs
(lungs, liver and kidneys result in accumulation of waste products. One organ
failure leads to another.
Recovery unlikely
DIAGNOSTIC EVALUATION
Blood: RBC, hemoglobin and hematocrit
Arterial Blood Gases: respiratory
alkalosis and metabolic acidosis
Electrolyte (Na level increased
early, decreased later if hypotonic fluid given) K decrease later increase K
with cellular breakdown and renal failure
BUN and creatinine increased,
specific gravity increased then fixed at 1.010
Blood cultures: identify causative
organism in septic shock
Cardiac enzymes: diagnosis of
cardiogenic shock
Glucose: increased early then
decreased
DIC screen: fibrinogen level,
platelet count, PTT and PT, thrombin time
Lactic acid: increased
Liver enzymes: ALT, AST and GGT
increased
MANAGEMENT
General management strategies for a
patient in shock begin with ensuring that the patient has a patient airway and
oxygen delivery is optimized. The cornerstone of therapy for septic,
hypovolemic and anaphylactic shock is volume expansion with the administration
of the appropriate fluid
It is generally accepted that
isotonic crystalloids, such as normal saline, are used in the initial
resuscitation of shock. If the patient does not respond to 2 to 3 L of crystalloids, blood administration and
central venous monitoring maybe instituted
The primary goal of drug therapy for
shock is the correction of decreased tissue perfusion
Sympathomimetic drugs cause peripheral vasoconstriction and
are referred to as vasopressor drugs (e.g. epinephrine and norepinephrine)
The goals of vasopressor therapy are to achieve and maintain
a mean arterial pressure (MAP) of 60 to 65 mm Hg and the use of these drugs is
reserved for patients unresponsive to other therapies
The goal of vasodilator therapy, as in vasopressor therapy,
is to maintain Mean arterial pressure at 60 mm Hg or greater
Vasodilator agents most often used are nitroglycerin (in cardiogenic
shock) and nitroprusside)
COLLABORATIVE CARE
Cardiogenic
Shock
Overall goal is to restore blood flow
to the myocardium by restoring the balance between oxygen supply and demand
Definitive measures include
thrombolytic therapy, angioplasty with stenting, emergency revascularization
and valve replacement
Care involves hemodynamic monitoring,
drug therapy (e.g. diuretics to reduce preload), and use of circulatory assist
devices (e.g. intra-aortic balloon pump, ventricular assist device)
Hypovolemic
Shock
The underlying principles of managing
patients with hypovolemic shock focus on stopping the loss of fluid and
restoring the circulating volume
Fluid replacement is calculated using
a 3:1 rule (3 ml of isotonic crystalloid for every 1 ml of estimated blood
loss)
Septic Shock
Patients in septic shock require
large amounts of fluid replacement, sometimes as much as 6 to 10 L of isotonic
crystalloids and 2 to 4 L of colloids, to restore perfusion
Vasopressor drug therapy maybe added
and vasopressin maybe given to patient’s refractory to vasopressor therapy
Intravenous corticosteroids are
recommended for patients who require vasopressor therapy, despite fluid
resuscitation, to maintain adequate BP
Antibiotics are early component of
therapy and are started after obtaining cultures
Drotrecogin alpha, a recombinant form
of activated protein C, has demonstrated promise in treating patients with
severe sepsis.
Glucose levels should be maintained
at less than 150 mg/dl
Stress ulcer prophylaxis with
histamine (H2)-receptor blockers and deep vein thrombosis prophylaxis with low
dose unfractionated heparin or low molecular weight heparin are recommended
Neurogenic
Shock
Treatment of neuogenic shock is
dependent on the tissue
In spinal cord injury, general measures to promote spinal stability are
initially used
Definitive treatment of the hypotension and bradycardia involves the use
of vasopressor and atropine respectively
Fluids are administered cautiously as the cause of the hypotension is
generally not related to fluid loss
The patient is monitored for hypothermia
Anaphylactic
Shock
Epinephrine is the drug of choice to
treat anaphylactic shock
Diphenhydramine is administered to
block the massive release of histamine
Maintaining a patent airway is
critical and the use of nebulization with bronchodilators is highly effective
Endotracheal intubation or
cricothyroidotomy maybe necessary
Aggressive fluid replacement,
predominantly with colloids, is necessary
Intravenous corticosteroids maybe
helpful in anaphylactic shock if significant hypotension persists after 1 to 2
hours of aggressive therapy
NURSING MANAGEMENT
Acute Intervention
The role of the nurse in shock involves
Monitoring the patient’s ongoing physical and emotional status to detect
subtle changes in the patient’s condition
Planning and implementing nursing interventions and therapy
Evaluating the patient’s response to therapy
Providing emotional support to the patient and family and
Collaborating with other members of the health team when warranted by the
patient’s condition
NURSING CARE
Neurologic status, including
orientation and level of consciousness, should be assessed every hour or more
often.
Heart rate, rhythm, BP, central
venous pressure and PA pressures including continuous cardiac output should be
assessed at least every 15 minutes.
The patient’s ECG should be
continuously monitored to detect dysrhythmias that may result from the
cardiovascular and metabolic derangements associated with shock. Heart sounds
should be assessed for the presence of an S3 and S4 sound or new murmurs. The
presence of an S3 sound in an adult usually indicated heart failure.
The respiratory status of the patient
in shock must be frequently assessed to ensure adequate oxygenation, detect
complications early and provide data regarding the patient’s acid base status.
Pulse oximetry is used to
continuously monitor oxygen saturation.
Arterial blood gases (ABGs) provide
definitive information on ventilation and oxygenation status, and acid base
balance.
Most patients in shock will be
intubated and on mechanical ventilation.
Hourly urine output measurements
assess the adequacy of renal perfusion and a urine output of less than 0.5
ml/kg/hour may indicate inadequate kidney perfusion.
BUN and serum creatinine values are
also used to assess renal function.
Tympanic or pulmonary arterial
temperatures should be obtained hourly if temperature is elevated or subnormal,
otherwise every 4 hours.
Capillary refill should be assessed
and skin monitored for temperature, pallor, flushing, cyanosis and diaphoresis
Bowel sounds should be auscultated at
least every 4 hours and abdominal distention should be assessed
If a nasogastric tube is inserted,
drainage should be checked for occult blood as should stools
Oral care for the patient in shock is
essential and passive range of motion should be performed three or four times
per day
Anxiety, fear and pain may aggravate
respiratory distress and increase the release of catecholamines
The nurse should talk to the patient,
even if the patient is intubated, sedated and paralyzed or appears comatose. If
the intubated patient is capable of writing, a pencil and paper should be
provided.
EMERGENCY CONDITIONS – Shock (Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management)
CEREBROVASCULAR ACCIDENT (STROKE) –
Etiology, Risk Factors, Signs and Symptoms, Diagnostic Evaluation and
Management
A cerebrovascular accident is also
called a CVA, brain attack, or stroke. It occurs when blood flow to a part of
the brain is suddenly stopped and oxygen cannot get to that part. This lack of
oxygen may damage or kill the brain cells. Death of a part of the brain may
lead to loss of certain body functions controlled by that affected part and it
last longer than 24 hours
A transient ischemic attack (TIA) –
also called a mini stroke, is a brief episode of symptoms similar to those have
in a stroke. A transient ischemic attack is caused by a temporary decrease in
blood supply to part of brain. It last less than five minutes.
ETIOLOGY AND TYPES
Ischemic Stoke
Any ischemic stroke occurs when a blood clot blocks a blood
vessel, preventing blood and oxygen from getting to a part of the brain. When a
clot forms somewhere else in the body and gets lodged in a brain blood vessel,
it is called an embolic stroke. When the clot forms in the brain blood vessel,
it is called a thrombotic stroke.
Hemorrhagic Stroke
A hemorrhagic stroke occurs when a
blood vessel ruptures, or hemorrhages, which then prevents blood from getting
to part of the brain. The hemorrhage may occur in a blood vessel in the brain,
or in the membrane that surrounds the brain. It maybe of the following types:
Intracerebral hemorrhage: in an
intracerebral hemorrhage, a blood vessel in the brain bursts and spills into
the surrounding brain tissue, damaging brain cells. Brain cells beyond the leak
are deprived of blood and damaged. High blood pressure, trauma, vascular
malformations, use of blood-thinning medications and other conditions may cause
intracerebral hemorrhage
Subarachnoid hemorrhage: in a
subarachnoid hemorrhage, an artery on or near the surface of brain bursts and
spills into the space between the surface of brain and skull. This bleeding is
often signaled by a sudden, severe headache. A subarachnoid hemorrhage is
commonly caused by the rupture of an aneurysm, a small sack-shaped or
berry-shaped outpouching on an artery in the brain.
RISK FACTORS
High blood pressure
Cigarette smoking or exposure to
second hand smoke
High cholesterol level
Diabetes
Overweight or obese
Physical inactivity
Obstructive sleep apnea
Cardiovascular disease, including
heart failure, heart defects, heart infection or abnormal heart rhythm
Use of some birth control pills or
hormone therapies that include estrogen
Heavy drinking
Use of drugs such as cocaine and
methamphetamines
Having regular checkups after being
diagnosed with preeclampsia
Personal or family history of stroke,
heart attack or TIA
Being age 55 or older
Race-Black has higher risk of stroke
than people of other races
Gender-stroke is more common in women
than men, and more deaths from stroke occur in women
PATHOPHYSIOLOGY
Due to thrombosis or embolism, some
neurons die because of lack of oxygen and nutrients —- infarction of the
cerebral vessels known as stroke —- tissue injury triggers an inflammatory
response which increases intracranial pressure —- the injury disrupts
metabolism leading to changes in ionic transport, localized acidosis, and free
radical formation —- calcium, sodium and water accumulate in the injured
cells and excitatory neurotransmitters are released —- continued cell
cellular injury and swelling both occurs resulting to further cell damage —–
Brain Death
Impaired cerebral tissue perfusion
(hemorrhagic) —- infarction of the cerebral vessels known as stroke —-
space-occupying blood clots put more pressure on the brain tissues —- the regulatory
mechanisms of the brain attempt to maintain equilibrium by increasing BP and
ICP —- the ruptured cerebral vessels may constrict to limit blood loss
however; this vasospam will result to further ischemia and necrosis of brain
tissues —- Brain Death
SIGNS AND SYMPTOMS
Difficulty walking
Dizziness
Loss of balance and coordination
Difficulty speaking or understanding
others who are speaking
Numbness or paralysis in the face,
leg, or arm, most likely on just one side of the body
Blurred or darkened vision
A sudden headache, especially when
accompanied by nausea, vomiting, or dizziness
DIAGNOSTIC EVALUATION
Physical examination
Personal and family history of heart
disease, TIA or stroke
Blood tests: to evaluate the clotting
time, bleeding time, etc
Computerized tomography scan: brain
imaging plays a key role in determining a stroke and what type of stroke maybe
experiencing. A CT scan uses a series of X-rays to create a detailed image of
brain. A CT scan can show a brain hemorrhage, tumors, strokes and other
conditions. A dye is injected into blood vessels to view blood vessels to view
blood vessels in neck and brain in greater detail
Magnetic resonance imaging: an MRI
uses powerful radio waves and magnets to create a detailed view of brain. An
MRI can detect brain tissue damaged by an ischemic stroke and brain hemorrhages
Carotid ultrasound: in this test,
sound waves create detailed images of the inside of the carotid arteries in
neck. This test shows buildup of fatty deposits (plaques) and blood flow in
carotid arteries
Cerebral angiogram: in this test, a
thin, flexible tube (catheter) is inserted through a small incision, usually in
groin, and guides it through major arteries and into carotid or vertebral
artery. A dye is injected into blood vessels to make them visible under X-ray
imaging. This procedure gives a detailed view of arteries in brain and neck
Echocardiogram: this imaging
technique uses sound waves to create a picture of heart. It can help to find
the source of blood clots
MANAGEMENT
Prevention
There are
many risk factors for having a stroke. Correspondingly, there are many measures
that can be taken to help prevent them. These preventive measures are similar
to the actions that you would take to help prevent heart disease, and include
the following:
Maintain normal blood pressure
Limit saturated fat and cholesterol
intake
Refrain from smoking and drink
alcohol in moderation
Control diabetes
Maintain a healthy weight
Get regular exercise
Eat a diet rich in vegetables and
fruits
Medical
Management
Aspirin, an antithrombotic drug, is
an immediate treatment after an ischemic stroke to reduce the likelihood of
having another stroke. Aspirin prevents blood clots from forming.
Other blood-thinning drugs, such as
heparin, warfarin, or aspirin in combination with extended release dipyridamole
may also be used, but these are not usually used in the emergency room setting.
Intravenous injection of tissue
plasminogen activator (TPA): some people who are having an ischemic stroke can
benefit from an injection of a recombinant tissue plasminogen activator (TPA),
also called alteplase, usually given through a vein in the arm. This potent
clot-busting drug needs to be given within 4.5 hours after stroke symptoms
begin if it is given into the vein. This drug restores blood flow by dissolving
the blood clot causing stroke
Carotid endarterectomy: in the
carotid endarterectomy, a surgeon removes fatty deposits (plaques) from carotid
arteries. In this procedure, a small incision along the front of neck, opens
carotid artery, and removes fatty deposits that block the carotid artery.
Angioplasty and stents: in an
angioplasty, a surgeon inserts a catheter with a mesh tube and balloon on the
tip into an artery in groin and guides it to the blocked carotid artery in
neck. Surgeon inflates the balloon in the narrowed artery and inserts a mesh
tube into the opening to keep artery from becoming narrowed after the
procedure.
Surgical clipping: a surgeon places a
tiny clamp at the base of the aneurysm, to stop blood flow to it. This can keep
the aneurysm from bursting
Coiling (endovascular embolization):
in this procedure, a surgeon inserts a catheter into an artery in groin and
guides it to brain using X-ray imaging. Then guides tiny detachable coils into
the aneurysm (aneurysm coiling). The coils fill the aneurysm, which blocks
blood flow into the aneurysm and causes the blood to clot
NURSING MANAGEMENT
Nursing
Diagnosis
Ineffective cerebral tissue perfusion
related to interruption of blood flow
Interventions
Determine factors related to
individual situation, cause for coma, decreased cerebral perfusion and
potential for increased ICP
Monitor and document neurological
status frequently and compare with baseline
Monitor vital signs, i.e.
hypertension/hypotension, compare BP readings in both arms, heart rate and
rhythm, auscultate for murmurs, respirations, noting patterns and rhythm, e.g.
periods of apnea after hypervenitilation, Cheyne-Stokes respiration.
Document changes in vision, e.g.,
reports of blurred vision, alternations in visual field and perception
Assess higher functions, including
speech, if patient is alert
Position with head slightly elevated
and in neutral position
Maintain bedrest, provide quiet
environment, and restrict visitors as indicated. Provide rest periods between
care activities, limit duration of procedures
Prevent straining at stool, holding
breath
Assess for nuchal rigidity,
twitching, increased restlessness, irritability, onset of seizure activity
Prepare for surgery, as appropriate,
e.g., endarterectomy, microvascular bypass, cerebral angioplasty
Monitor laboratory studies as
indicated, e.g., prothrombin time (PT), activated partial thromboplastin time
(aptt) time, dilantin level
Impaired physical mobility related to
neuromuscular abnormality
Assess functional ability of
impairment initially and on a regular basis
Change positions at least every 2
hour (supine, sidelying) and possibly more often if placed on affected side.
Position in prone position once or
twice a day if patient can tolerate
Prop extremities in functional
position, use footboard during the period of flaccid paralysis. Maintain
neutral position of head.
Use arm sling when patient is in
upright position, as indicated.
Evaluate use and need for positional
aids and splints during spastic paralysis, place pillow under axillae to abduct
arm, elevate arm and hand
Observe affected side for color,
edema, or other signs of compromised circulation
Inspect skin regularly, particularly
over bony prominences. Gently massage any reddened areas and provide aids such
as sheepskin pads as necessary
Begin active/passive range of motion
exercise to all extremities
Assist to develop sitting balance
(e.g. raise head of bed, assist to sit on edge of bed, having patient sue the
strong arm to support body weight and strong leg to move affected leg, increase
sitting time) and standing balance (e.g. put flat walking shoes on patient,
support patient’s lower back with hands while positioning own knees outside
patient’s knees, assist in using parallel bars/walkers).
Get patient up in chair as soon as
vital signs are stable, except following cerebral hemorrhage
Pad chair seat with foam or
water-filled cushion, and assist patient to shift weight at frequent intervals
Provide egg-crate mattress,
water-bed, flotation device, or specialized beds (e.g. kinetic), as indicated
Disturbed sensory perceptions related
to disturbed sensory reception and neuromuscular dysfunction
Eliminate extraneous noise and
stimuli as necessary
Speak in calm, quiet voice, using
short sentences. Maintain eye contact
Reorient patient frequently to
environment, staff, and procedures
Evaluate for visual deficits. Note
loss of visual field, changes in depth perception (horizontal/vertical planes),
and presence of diplopia
Approach patient from visually intact
side. Leave light on, position objects to take advantage of intact visual
fields. Patch affected eye if indicated
Assess sensory awareness, e.g.
differentiation of hot/cold, dull/sharp, position of body parts/muscle, joint
sense
Stimulate sense of touch; e.g. give
patient objects to touch, grasp
Protect from temperature extremes,
assess environment for hazards. Recommend testing warm water with unaffected
hand
Ineffective coping related to
situational crisis and cognitive perceptual changes
Interventions
Assess extent of altered perception
and related degree of disability. Determine functional independence measure
score
Identify meaning of the loss,
dysfunction and change to patient. Note ability to understand events, provide
realistic appraisal of situation
Determine outside stressors, e.g.
family, work, social, future nursing/healthcare needs
Encourage patient to express
feelings, including hostility or anger, denial, depression sense of
disconnectedness
Note whether patient refers to
affected side as ‘it’ or denies affected side and says it is ‘dead’
Identify previous methods of dealing
with life problems. Determine presence and quality of support systems
Emphasize small gains either in
recovery of function or independence
Support behaviors and efforts such as
increased interest, participation in rehabilitation activities
Monitor for sleep disturbance, increased
difficulty concentrating and statements of inability to cope, lethargy, and
withdrawal
Refer for neuropsychological
evaluation and/or counseling if indicated
Self-care deficit related to
neuromuscular impairment and decreases strength and endurance
Interventions
Assess abilities and level of deficit
(0-4 scale) for performing ADLs
Avoid doing things for patient that
patient can do for self, but provide assistance as necessary
Be aware of impulsive behavior and
actions suggestive of impaired judgment
Maintain a supportive, firm attitude.
Allow patient sufficient time to accomplish task.
Provide positive feedback for efforts
and accomplishments
Create plan for visual deficits that
are present, e.g. place food and utensils on the tray related to patient’s
unaffected side, situate the bed so that patient’s unaffected side is facing
the room with the affected side to the wall, position furniture against wall
and out of travel path
Provide self-help devices, e.g.
button/zipper hook, knife-fork combinations, long-handled brushes, extensions
for picking things up from floor, toilet riser, leg bag for catheter, shower
chair
Assist and encourage good grooming
and makeup habits
Encourage family member to allow
patient to do as much as possible for self
Assess patient’s ability to
communicate the need to void and ability to use urinal, bedpan. Take patient to
the bathroom at frequent and periodic intervals for voiding if appropriate
Identify previous bowel habits and
re-establish normal regimen. Increase bulk in diet, encourage fluid intake,
increased activity
Risk for impaired swallowing related
to neuromuscular dysfunction
Intervention
Review individual pathology and
ability to swallow, noting extend of paralysis, clarity of speech, facial,
tongue involvement, ability to protect airway and episodes of coughing or
choking, presence of adventitious breath sounds, amount and character of oral
secretions
Have suction equipment available at
bedside, especially during early feeding efforts
Promote effective swallowing, e.g.
schedule activities, medications to provide a minimum of 30 min rest before
eating, provide pleasant environment free of distractions, assist patient with
head control and support, and position based on specific dysfunction
Place patient in upright position
during and after feeding as appropriate
Provide oral care based on individual
need prior to meal
Season food with herbs, spices, lemon
juice, etc. according to patient’s preference, within dietary restrictions
Place food of appropriate consistency
in unaffected side of mouth
Touch parts of the cheek with tongue
blade and apply ice to weak tongue
Feed slowly, allowing 30-45 min for
meals
Offer solid foods and liquids at
different times
Maintain upright position for 45-60
min after eating
Maintain accurate intake output,
record calorie count
Encourage participation in exercise
Administer IV fluids and or tube
feedings
Coordinate multidisciplinary approach
to develop treatment plan that meets individual needs
Knowledge deficit related to lack of
exposure and cognitive limitation
Interventions
Evaluate type and degree of
sensory-perceptual involvement
Include family in discussions and
teaching
Discuss specific pathology and
individual potentials
Identify signs and symptoms requiring
further follow-up, e.g. changes or decline in visual, motor, sensory function,
alternation in mentation or behavioral responses, severe headache
Review current restrictions or
limitations and discuss planned resumption of activities (including sexual
relations)
Provide written instructions and
schedules for activity, medication, important facts
Encourage patient to refer to lists
communication or notes instead of depending on memory
Discuss plans for meeting self-care
needs
Refer to discharge planner, home care
supervisor, visiting nurse
Suggest patient reduce or limit
environmental stimuli, especially during cognitive activities
Recommend patient seek assistance in
problem-solving process and validate decisions, as indicated
Review importance of balanced diet,
low in cholesterol and sodium if indicated. Discuss role of vitamins and other
supplements
Refer to reinforce importance of
follow-up care by rehabilitation team, e.g. physical, occupational, speech,
vocational therapists.
CEREBROVASCULAR ACCIDENT (STROKE) – Etiology, Risk Factors, Signs and Symptoms, Diagnostic Evaluation and Management