Nurseinfo.in provides free Nursing Notes, Nursing Procedures, Medical MCQs, Nursing Calculators, Care Plans and exam preparation resources for BSc Nursing, GNM, P.B. BSc and MSc Nursing students. Browse subject-wise notes, previous year questions and study materials based on the latest nursing syllabus.
Nurseinfo.in provides free Nursing Notes, Nursing Procedures, Medical MCQs, Nursing Calculators, Care Plans and exam preparation resources for BSc Nursing, GNM, P.B. BSc and MSc Nursing students. Browse subject-wise notes, previous year questions and study materials based on the latest nursing syllabus.
Complete Nursing Notes for BSc, GNM & MSc Nursing Students (2026)
Welcome to NurseInfo Nursing Notes, a complete educational resource for BSc Nursing, GNM, P.B BSc Nursing, and MSc Nursing students. This website provides organized nursing notes, study materials, MCQs, nursing care plans, exam preparation resources, and subject-wise study guides prepared according to the latest nursing syllabus.
Our goal is to help nursing students improve their academic performance, clinical knowledge, and exam preparation through easy-to-understand nursing notes and educational resources.
Whether you are preparing for university exams, competitive nursing exams, NCLEX, OET, HAAD, DHA, MOH, IQN, or other nursing assessments, NurseInfo offers structured study materials to support your learning journey.
Nursing Notes for All Subjects
We provide nursing notes and study materials for major nursing subjects including:
Medical Surgical Nursing Notes
Medical Surgical Nursing notes cover important diseases, patient care, nursing interventions, diagnosis, treatment, and nursing management. Students can learn cardiovascular disorders, respiratory diseases, renal disorders, gastrointestinal conditions, neurological problems, endocrine disorders, and more.
Pharmacology Nursing Notes
Pharmacology notes include drug classifications, mechanisms of action, side effects, nursing responsibilities, dosage calculations, and patient education. These notes help students understand safe medication administration and pharmacological concepts.
Anatomy and Physiology Nursing Notes
Anatomy and Physiology notes explain the structure and functions of the human body. Students can study body systems, organs, physiological processes, and important concepts required for nursing practice.
Mental Health Nursing Notes
Mental Health Nursing notes include psychiatric disorders, therapeutic communication, crisis intervention, counseling concepts, mental health assessment, and nursing management of psychiatric conditions.
Community Health Nursing Notes
Community Health Nursing notes focus on public health, disease prevention, health promotion, family health nursing, epidemiology, immunization programs, and community-based healthcare services.
Child Health Nursing Notes
Child Health Nursing notes help students understand pediatric nursing care, growth and development, common childhood disorders, neonatal care, vaccination schedules, and pediatric nursing interventions.
Obstetrics and Gynecological Nursing Notes
Obstetrics and Gynecological Nursing notes include antenatal care, labor management, postpartum care, gynecological disorders, maternal health, newborn care, and reproductive health nursing.
Nursing Research and Statistics Notes
Research and statistics notes explain research methodologies, data analysis, sampling techniques, evidence-based practice, and nursing research principles.
Nursing MCQs and Exam Preparation
In addition to nursing notes, we provide:
Nursing MCQs with answers
Exam preparation questions
Prioritization questions
Case study discussions
Nursing care plans
Objective type questions
Viva questions and answers
These resources help nursing students improve critical thinking, clinical judgment, and exam confidence.
Nursing Notes for Competitive Exams
Our nursing study materials are useful for:
NCLEX preparation
OET nursing exam
HAAD exam
DHA nursing exam
MOH nursing exam
IQN nursing exam
Prometric nursing exam
Staff nurse recruitment exams
Nursing entrance examinations
Students can use these nursing notes to strengthen theoretical knowledge and prepare effectively for professional nursing exams.
Why Choose NurseInfo Nursing Notes?
Organized Subject-wise Notes
All nursing subjects are categorized systematically for easy learning and quick access.
Exam-focused Study Materials
Our nursing notes are prepared according to the latest nursing syllabus and exam patterns.
Simple and Easy Explanations
Complex nursing concepts are explained in a clear and student-friendly manner.
Useful for All Nursing Students
The study materials are helpful for BSc Nursing, GNM, P.B BSc Nursing, MSc Nursing, and nursing exam aspirants.
Regularly Updated Content
We continuously update nursing notes and educational resources to maintain quality and relevance.
Popular Nursing Subjects
Fundamentals of Nursing
Medical Surgical Nursing
Pharmacology
Anatomy and Physiology
Mental Health Nursing
Pediatric Nursing
Community Health Nursing
Nursing Education
Nursing Management
Nursing Research and Statistics
Frequently Asked Questions (FAQ)
What are nursing notes?
Nursing notes are educational study materials prepared to help nursing students understand nursing concepts, diseases, patient care, and clinical procedures.
Are these nursing notes useful for exams?
Yes. These notes are designed according to nursing syllabus and are useful for university exams and competitive nursing exams.
Which nursing students can use these notes?
BSc Nursing, GNM, P.B BSc Nursing, MSc Nursing, and other healthcare students can use these nursing notes.
Are MCQs available for nursing subjects?
Yes. We provide nursing MCQs, objective questions, prioritization questions, and exam preparation materials.
How should nursing students use these notes?
Students should study topic-wise notes regularly, practice MCQs, revise important concepts, and use nursing care plans for clinical learning.
Final Thoughts
Nursing education requires dedication, clinical knowledge, and consistent practice. NurseInfo Nursing Notes is designed to support nursing students by providing organized study materials, nursing notes, MCQs, and exam preparation resources in one place.
Our mission is to simplify nursing education and help students achieve academic and professional success through high-quality nursing learning resources.
Continue learning, practicing, and improving your nursing knowledge to build a successful nursing career.
Concurrent and Terminal Disinfection in Nursing: Definition, Purpose, Procedure, and Responsibilities
UPDATED 2026
Introduction
Infection prevention and control are essential components of nursing care. Disinfection helps reduce the spread of microorganisms and protects patients, healthcare workers, and visitors from infectious diseases. Two important methods used in healthcare settings are concurrent disinfection and terminal disinfection. Understanding these procedures is crucial for nursing students and healthcare professionals.
What is Disinfection?
Disinfection is the process of destroying or reducing harmful microorganisms on surfaces, equipment, and objects to prevent the spread of infection. Unlike sterilization, disinfection may not eliminate all bacterial spores but significantly reduces the risk of disease transmission.
Definition of Concurrent Disinfection
Concurrent disinfection refers to the immediate cleaning and disinfection of infectious materials, contaminated articles, and patient surroundings while the patient is still in the healthcare facility. It is carried out continuously throughout the patient’s stay to prevent the spread of infection.
Examples of Concurrent Disinfection
Cleaning blood or body fluid spills immediately.
Disinfecting patient-care equipment after use.
Proper disposal of contaminated dressings and waste.
Cleaning frequently touched surfaces such as bed rails and bedside tables.
Definition of Terminal Disinfection
Terminal disinfection is the thorough cleaning and disinfection of a patient’s room, furniture, equipment, and environment after the patient has been discharged, transferred, or has died. It ensures that the area is safe for the next patient.
Examples of Terminal Disinfection
Cleaning walls, floors, and furniture after patient discharge.
Disinfecting reusable medical equipment.
Replacing bed linens and curtains.
Disinfecting high-touch surfaces throughout the room.
Objectives of Concurrent and Terminal Disinfection
The primary objectives include:
Preventing the spread of infectious diseases.
Breaking the chain of infection.
Protecting healthcare workers, patients, and visitors.
Maintaining a safe healthcare environment.
Reducing healthcare-associated infections (HAIs).
Supporting quality patient care.
Importance of Concurrent Disinfection
Concurrent disinfection plays a vital role in infection control because it:
Reduces the immediate risk of cross-contamination.
Prevents the spread of pathogens within healthcare facilities.
Maintains cleanliness around infected patients.
Protects healthcare workers from occupational exposure.
Supports standard infection prevention measures.
Importance of Terminal Disinfection
Terminal disinfection is important because it:
Eliminates pathogens remaining in the patient’s environment.
Reduces the risk of infection for future occupants.
Ensures hospital rooms meet infection control standards.
Prevents outbreaks caused by environmental contamination.
Promotes patient safety and quality healthcare.
Principles of Concurrent Disinfection
The following principles should be followed:
Perform cleaning immediately after contamination occurs.
Use approved disinfectants according to guidelines.
Wear appropriate personal protective equipment (PPE).
Practice proper hand hygiene before and after procedures.
Dispose of infectious waste safely.
Follow standard precautions at all times.
Ensure contaminated items are handled carefully.
Principles of Terminal Disinfection
Important principles include:
Thoroughly clean all surfaces before disinfection.
Remove visible dirt and organic matter.
Disinfect all reusable equipment.
Follow the recommended disinfectant contact time.
Use appropriate PPE during cleaning.
Properly dispose of waste materials.
Ensure adequate ventilation when using disinfectants.
Procedure of Concurrent Disinfection
Preparation
Gather necessary cleaning supplies and disinfectants.
Perform hand hygiene.
Wear gloves and other PPE as required.
During the Procedure
Clean contaminated surfaces immediately.
Disinfect reusable equipment after each use.
Handle soiled linens carefully.
Dispose of contaminated waste according to policy.
Clean spills of blood and body fluids promptly.
After the Procedure
Remove PPE safely.
Dispose of waste appropriately.
Perform hand hygiene.
Document actions if required.
Procedure of Terminal Disinfection
Step 1: Preparation
Wear appropriate PPE.
Remove waste and used linens from the room.
Step 2: Cleaning
Clean furniture, equipment, walls, and floors.
Remove dust and visible dirt.
Clean high-touch surfaces thoroughly.
Step 3: Disinfection
Apply approved disinfectants to all surfaces.
Follow the manufacturer’s recommended contact time.
Disinfect reusable medical equipment.
Step 4: Final Inspection
Check the cleanliness of the room.
Replace clean linens and supplies.
Prepare the room for the next patient.
Difference Between Concurrent and Terminal Disinfection
Feature
Concurrent Disinfection
Terminal Disinfection
Timing
During patient stay
After discharge or transfer
Purpose
Prevent ongoing spread of infection
Eliminate remaining microorganisms
Frequency
Continuous
Performed after patient leaves
Area Covered
Contaminated items and surroundings
Entire room and equipment
Goal
Immediate infection control
Prepare environment for next patient
Nursing Responsibilities
Nurses play a crucial role in maintaining infection control. Their responsibilities include:
Following infection prevention protocols.
Performing proper hand hygiene.
Using PPE correctly.
Educating patients and caregivers.
Monitoring environmental cleanliness.
Reporting infection control concerns.
Ensuring safe disposal of biomedical waste.
Documenting disinfection activities when required.
Advantages of Concurrent and Terminal Disinfection
Reduces infection transmission.
Prevents healthcare-associated infections.
Improves patient safety.
Protects healthcare workers.
Maintains a clean healthcare environment.
Supports quality healthcare services.
Conclusion
Concurrent and terminal disinfection are essential infection control measures in healthcare settings. Concurrent disinfection prevents the spread of infection during patient care, while terminal disinfection ensures that the environment is safe after the patient leaves. Proper implementation of these procedures helps protect patients, healthcare workers, and the community from infectious diseases.
Frequently Asked Questions (FAQs)
What is concurrent disinfection?
Concurrent disinfection is the immediate cleaning and disinfection of contaminated materials and surfaces while the patient is still receiving care.
What is terminal disinfection?
Terminal disinfection is the thorough cleaning and disinfection of a patient’s environment after discharge, transfer, or death.
Why is concurrent disinfection important?
It prevents the immediate spread of infectious microorganisms and reduces cross-contamination.
Why is terminal disinfection necessary?
It removes remaining pathogens from the environment and prepares the area for future use.
Who is responsible for disinfection in healthcare settings?
Nurses, infection control personnel, and environmental service staff share responsibility for maintaining effective disinfection practices.
Cardiopulmonary Resuscitation (CPR) is a life-saving emergency procedure used when a person’s heart stops beating or breathing stops. CPR combines chest compressions and rescue breaths to maintain blood circulation and oxygen supply to vital organs until advanced medical care becomes available. Early recognition of cardiac arrest and immediate CPR can significantly improve survival outcomes.
What is Cardiopulmonary Resuscitation (CPR)?
Cardiopulmonary Resuscitation (CPR) is an emergency technique performed to manually preserve brain function and blood circulation in a person experiencing cardiac arrest or respiratory arrest. It is an essential component of Basic Life Support (BLS).
Definition of CPR
CPR is a lifesaving procedure involving chest compressions and artificial ventilation performed on an individual whose breathing or heartbeat has stopped, with the aim of maintaining circulation and oxygenation until spontaneous circulation is restored.
Objectives of CPR
The main objectives of CPR include:
Maintain blood flow to the brain and heart.
Provide oxygen to body tissues.
Prevent irreversible brain damage.
Increase the chances of survival.
Support life until advanced medical treatment is available.
Restore spontaneous circulation and breathing.
Learn the essential steps of Cardiopulmonary Resuscitation (CPR), including chest compressions, rescue breaths, AED use, and emergency response guidelines. Ideal for nursing students and healthcare professionals.
Importance of CPR
CPR is important because:
Brain damage can begin within minutes after cardiac arrest.
Immediate CPR helps maintain oxygen delivery to vital organs.
Early CPR improves survival rates.
It buys time until emergency medical services arrive.
It is a critical link in the Chain of Survival.
Indications for CPR
CPR should be initiated when a person:
Is unresponsive.
Is not breathing normally.
Has no pulse or signs of circulation.
Experiences sudden cardiac arrest.
Suffers severe respiratory arrest.
Is found unconscious with absent breathing.
Contraindications of CPR
CPR may not be indicated when:
There is a valid Do Not Resuscitate (DNR) order.
Obvious signs of irreversible death are present.
The environment is unsafe for the rescuer.
Severe injuries incompatible with life are observed.
Equipment Required for CPR
The following equipment may be used during CPR:
Personal Protective Equipment (PPE)
Pocket mask
Face shield
Bag-Valve-Mask (BVM)
Automated External Defibrillator (AED)
Oxygen source
Suction apparatus
Emergency crash cart
Basic Principles of CPR
Ensure scene safety.
Check patient responsiveness.
Activate emergency response system.
Begin high-quality chest compressions.
Maintain airway patency.
Provide effective rescue breaths.
Use an AED as soon as available.
Minimize interruptions in chest compressions.
Steps of Adult CPR
Step 1: Ensure Safety
Check the surroundings and ensure the area is safe for both the rescuer and the victim.
Step 2: Check Responsiveness
Tap the person’s shoulders and ask loudly:
“Are you okay?”
If there is no response, proceed immediately.
Step 3: Call for Help
Call emergency medical services.
Ask someone to bring an AED if available.
Step 4: Check Breathing
Look for normal breathing.
If breathing is absent or abnormal, begin CPR.
Step 5: Start Chest Compressions
Hand Position
Place the heel of one hand in the center of the chest.
Place the other hand on top.
Interlock fingers.
Compression Technique
Keep arms straight.
Push hard and fast.
Allow complete chest recoil after each compression.
Recommended Compression Rate
100–120 compressions per minute
Recommended Compression Depth
5–6 cm (2–2.4 inches) in adults
Step 6: Open the Airway
Use the:
Head Tilt–Chin Lift Method
Tilt the head backward.
Lift the chin upward.
If neck injury is suspected, use the jaw-thrust maneuver.
Step 7: Give Rescue Breaths
Pinch the nose closed.
Seal your mouth over the victim’s mouth.
Deliver one breath over one second.
Observe chest rise.
Give:
2 rescue breaths after every 30 compressions
Step 8: Continue CPR
Continue cycles of:
30 Chest Compressions : 2 Rescue Breaths
Continue until:
The person regains consciousness.
Emergency personnel arrive.
An AED is available and ready.
You are physically unable to continue.
Adult CPR Parameters
Component
Recommendation
Compression Rate
100–120/min
Compression Depth
5–6 cm
Compression-to-Breath Ratio
30:2
Chest Recoil
Complete
Compression Interruptions
Minimal
Hand Position
Center of Chest
Pediatric CPR Overview
Infants
Compression depth: About 4 cm
Use two fingers for single rescuer CPR
Children
Compression depth: About 5 cm
One or two hands may be used depending on child size
Use of Automated External Defibrillator (AED)
An AED is a portable device used to treat sudden cardiac arrest.
Steps
Turn on the AED.
Attach electrode pads.
Follow voice prompts.
Deliver shock if advised.
Resume CPR immediately after shock.
Nursing Responsibilities During CPR
Nurses play a vital role during resuscitation.
Responsibilities include:
Assess patient responsiveness.
Activate emergency response system.
Initiate CPR promptly.
Maintain airway patency.
Assist with ventilation.
Monitor patient condition.
Prepare emergency medications.
Assist with defibrillation.
Record events accurately.
Communicate with healthcare team members.
Provide emotional support to family members.
Advantages of CPR
Maintains circulation.
Preserves brain function.
Increases survival rates.
Supports oxygen delivery.
Prevents organ damage.
Buys time until advanced treatment is available.
Possible Complications of CPR
Although CPR is lifesaving, complications may occur:
Rib fractures
Sternal fractures
Internal organ injury
Gastric distension
Aspiration
Chest discomfort after recovery
Chain of Survival
The Chain of Survival includes:
Early recognition of cardiac arrest.
Early activation of emergency services.
Early CPR.
Early defibrillation.
Advanced life support.
Post-cardiac arrest care.
Patient Education
Healthcare professionals should educate the public about:
Recognizing cardiac arrest.
Learning CPR techniques.
Importance of early CPR.
AED awareness.
Emergency response activation.
Conclusion
Cardiopulmonary Resuscitation (CPR) is one of the most important emergency procedures in healthcare. Prompt initiation of CPR can significantly improve survival and reduce complications associated with cardiac arrest. Every nurse and healthcare professional should possess the knowledge and skills required to perform high-quality CPR effectively and confidently.
Frequently Asked Questions (FAQs)
What does CPR stand for?
CPR stands for Cardiopulmonary Resuscitation.
What is the purpose of CPR?
The purpose of CPR is to maintain blood circulation and oxygen delivery to vital organs during cardiac arrest.
What is the compression-to-breath ratio in adult CPR?
The recommended ratio is 30 compressions to 2 rescue breaths (30:2).
What is the recommended compression rate?
The recommended compression rate is 100–120 compressions per minute.
What is the recommended compression depth for adults?
The recommended depth is 5–6 cm (2–2.4 inches).
When should CPR be stopped?
CPR should continue until the patient recovers, trained medical personnel take over, or the rescuer becomes unable to continue.
CARDIOPULMONARY RESUSCITATION (CPR) (Definition, Purpose, Equipment, General Instructions, Procedure, Method, Do’s and don’ts in CPR and Complications.
Back care is an important nursing procedure performed to maintain skin integrity, improve circulation, promote relaxation, and prevent pressure sores in bedridden patients. It includes cleaning the back, assessing the skin condition, and providing a gentle massage or back rub. Regular back care contributes to patient comfort and helps prevent complications associated with prolonged bed rest.
Definition of Back Care
Back care is a nursing procedure that involves cleaning, inspecting, and massaging the patient’s back to maintain hygiene, stimulate circulation, prevent skin breakdown, and promote comfort.
Definition of Back Massage
Back massage is the systematic manipulation of the muscles and soft tissues of the back using gentle strokes and movements to promote relaxation, relieve muscle tension, and improve blood circulation.
Definition of Back Rub
A back rub is a gentle massage of the back using lotion or oil to provide comfort, stimulate circulation, and help the patient relax.
Purposes of Back Care
The purposes of back care include:
Promoting blood circulation.
Preventing pressure ulcers and bedsores.
Relieving muscle tension and fatigue.
Providing comfort and relaxation.
Encouraging restful sleep.
Maintaining skin cleanliness and integrity.
Observing the condition of the skin.
Enhancing patient well-being.
Importance of Back Care in Nursing
Back care is an essential component of nursing care, particularly for patients who are confined to bed. Regular back care helps identify early signs of pressure injury, improves circulation, prevents skin complications, and promotes patient comfort. It also provides an opportunity for nurses to assess the patient’s physical and emotional condition.
Indications for Back Care
Back care is commonly performed for:
Bedridden patients.
Elderly patients.
Postoperative patients.
Critically ill patients.
Patients with limited mobility.
Long-term hospitalized patients.
Patients at risk of pressure ulcers.
Contraindications for Back Massage
Back massage should be avoided in patients with:
Open wounds on the back.
Skin infections.
Burns.
Recent spinal surgery.
Spinal injuries.
Fractured ribs.
Severe skin irritation.
Areas of redness or pressure injury.
Articles Required
Basin with warm water.
Soap or cleansing solution.
Washcloth.
Towel.
Gloves.
Lotion or massage cream.
Mackintosh and draw sheet.
Privacy screen.
Waste container.
Preparation of the Patient
Explain the procedure to the patient.
Obtain consent if necessary.
Ensure privacy.
Perform hand hygiene.
Assemble all required articles.
Position the patient comfortably.
Expose only the back area while maintaining dignity.
Procedure of Back Care
Step 1: Position the Patient
Place the patient in a side-lying or prone position according to comfort and medical condition.
Step 2: Inspect the Skin
Observe the back carefully for redness, pressure areas, rashes, wounds, bruises, or signs of skin breakdown.
Step 3: Clean the Back
Wash the back gently with warm water and mild soap. Use smooth strokes to remove dirt, sweat, and dead skin cells.
Step 4: Rinse Thoroughly
Remove all soap residue to prevent skin irritation.
Step 5: Dry the Back
Pat the skin dry gently with a clean towel, paying special attention to skin folds and pressure areas.
Step 6: Apply Lotion
Warm a small amount of lotion between your hands and apply it evenly over the back.
Step 7: Perform Back Massage
Use gentle massage techniques with smooth and rhythmic movements. Avoid applying excessive pressure.
Step 8: Observe Patient Response
Monitor the patient for comfort, pain, or any signs of discomfort during the procedure.
Step 9: Reposition the Patient
Place the patient in a comfortable position and ensure safety measures are maintained.
Step 10: Document Findings
Record observations regarding skin condition and patient response.
Massage Techniques Used During Back Care
Effleurage
Effleurage involves long, smooth, gliding strokes performed with the palms of the hands. It helps relax muscles and improve circulation.
Petrissage
Petrissage is a kneading movement that gently lifts and squeezes muscle tissues to stimulate deeper circulation.
Friction
Friction consists of small circular movements that help improve blood flow to specific areas.
Circular Motion
Circular movements are used over the shoulders and larger muscle groups to promote relaxation.
Nursing Responsibilities
The nurse should:
Assess the patient’s condition before the procedure.
Maintain privacy and dignity.
Follow infection control measures.
Use proper body mechanics.
Observe skin condition carefully.
Identify early signs of pressure ulcers.
Ensure patient comfort throughout the procedure.
Report abnormalities promptly.
Document nursing observations accurately.
Advantages of Back Care
Improves blood circulation.
Prevents pressure sores.
Promotes relaxation.
Reduces muscle tension.
Enhances patient comfort.
Encourages restful sleep.
Maintains healthy skin.
Improves overall well-being.
Complications of Poor Back Care
If proper back care is not provided, patients may develop:
Pressure ulcers.
Skin breakdown.
Local infections.
Reduced circulation.
Increased discomfort.
Delayed recovery.
Muscle stiffness.
Prevention of Pressure Ulcers
Back care is an important measure in preventing pressure ulcers. Additional preventive measures include:
Repositioning patients every two hours.
Using pressure-relieving mattresses.
Maintaining skin hygiene.
Ensuring adequate nutrition and hydration.
Monitoring high-risk patients regularly.
Patient Education
Patients and caregivers should be educated about:
The importance of regular skin care.
Frequent position changes.
Adequate hydration.
Proper nutrition.
Early reporting of redness or skin changes.
Maintaining personal hygiene.
Conclusion
Back care, back massage, and back rub are fundamental nursing procedures that promote comfort, maintain skin integrity, improve circulation, and prevent pressure ulcers. Proper technique and regular assessment help ensure patient safety and contribute significantly to quality nursing care. Regular back care is especially important for bedridden and immobile patients to maintain health and prevent complications.
Frequently Asked Questions (FAQs)
What is back care in nursing?
Back care is a nursing procedure involving cleaning, inspection, and massage of the patient’s back to maintain hygiene, comfort, and skin integrity.
Why is back care important?
Back care helps prevent pressure ulcers, improves circulation, promotes relaxation, and enhances patient comfort.
What is a back rub?
A back rub is a gentle massage performed using lotion or oil to stimulate circulation and provide comfort.
Which patients require back care?
Bedridden patients, elderly patients, postoperative patients, and those with limited mobility commonly require back care.
What are the benefits of back massage?
Back massage improves circulation, reduces muscle tension, promotes relaxation, and helps prevent skin complications.
Keywords: back care in nursing, back massage procedure, back rub nursing notes, back care nursing procedure, nursing practical procedure, pressure ulcer prevention, bedridden patient care, fundamentals of nursing, nursing notes, patient comfort measures.
BACK CARE / BACK MASSAGE / BACK RUB – Definition, Purpose, Equipment, Procedure, After Care
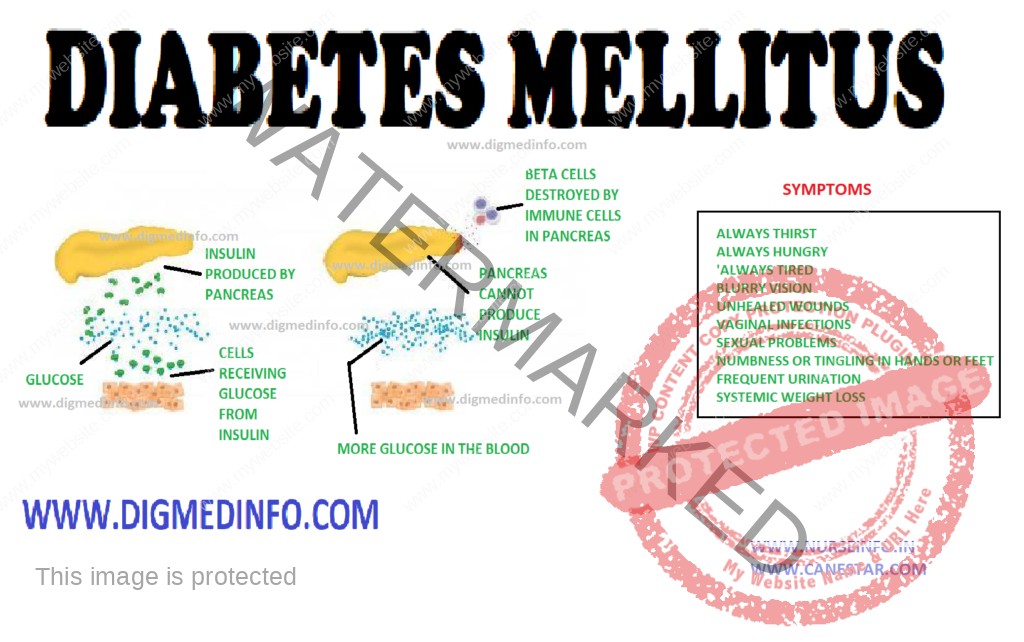
DIABETES MELLITUS – General Characteristics, Pancreas, Classification, Etiopathogenesis, Pathological Changes, Clinical Features, Diagnosis and Treatment
UPDATED 2024
General Characteristics
Diabetes
mellitus is a chronic metabolic disorder characterized by hyperglycemia with or
without glycosuria, resulting from an absolute or relative deficiency of
insulin. This is brought about by an impairment of insulin production or its
release by the beta cells of the islets of Langerhans. More often it is due to
a resistance to the action of insulin either due to a receptor/post receptor defect
or an imbalance between insulin and its counter regulatory hormones. Clinically
diabetes is characterized by a wide spectrum of disorders ranging from asymptomatic
hyperglycemia to abnormalities in the various organs.
PANCREAS
The
endocrine component of the pancreas consists of different types of cells:
α-cells, β-cells, δ-cells and PP cells contained in the islets of Langerhans
which constitute 1% of its weight. There are 100,000 islets in the pancreas, and
each islet contains 1000-3000 cells. Thus altogether there are 100-300 million
β-cells in the pancreas.
Pancreatic
beta cells can store 200 units of insulin and can release 30-50 units of
insulin per day. 95% of cells of the pancreas have exocrine function and 5%
have endocrine function. The beta cells produce insulin, alpha cells produce
glucagon, delta cells produce somatostatin and the PP cells produce pancreatic polypeptide.
CLASSIFICATION
The
Classification suggested by American Diabetes Association (ADA) is called as
the etiological classification of diabetes and has the two main types of
diabetes labeled as type 1 and type 2, along with gestational diabetes mellitus
and the other specific types where a precise etiological factor is identified.
The revised
diagnostic criteria give equal importance to the fasting and 2 hours post
glucose load plasma glucose (2h PG) for the diagnosis of diabetes, thereby eliminating
the need for a routine oral glucose tolerance test (OGTT) for the diagnosis of
diabetes. The cut-off level of fasting plasma glucose (FPG) for diagnosis of
diabetes has been fixed as 126 mg/dl, since this reflects the same degree of
hyperglycemia as a 2hr-PG of 200 mg/dl in terms of susceptibility for the development
of microvascular and macrovascular complications. These criteria are expected
to rationalize and simplify the diagnosis of diabetes and a larger number of
people could be screened due to the simplification of the procedure of doing
only fasting plasma glucose rather than an OGTT.
ETIOPATHOGENESIS
Type 1Diabetes:
Type-1
diabetes mellitus has been classified into type-1A in which cell-mediated autoimmune
attack on the beta cells is more prominent and type-1B in which the mechanism
is less clear. Type1B is less frequent of the two.
Classification of type-1 diabetes
mellitus
1.
Preclinical
a.
Autoantibodies + / OGTT normal.
b.
Autoantibodies + / OGTT abnormal.
c.
Autoantibodies + / fasting hyperglycemia
2. Clinical – with diabetes
1a.
Autoantibodies present (autoimmune)
1b.
Autoantibodies absent (idiopathic)
3. Explosive onset / fulminent onset
4. Rapid onset
5. Late onset (LADA).
ETIOLOGICAL CLASSIFICATION OF
DIABETES MELLITUS
1. Type 1 diabetes (cell destruction, usually leading
to absolute insulin deficiency)
• Immune
mediated
• Idiopathic
2. Type 2 diabetes (may range from predominantly
insulin resistance with relative insulin deficiency to a predominantly secretory
defect with insulin resistance)
Type 2 DM
(previously known as NIDDM) is considered as a ‘multifactorial’ or ‘complex’
disease due to the complex interaction between various genetic and environmental
factors in its pathogenesis. Multiple evidence suggests that genetic factors
play a major role in this condition. A genetic predisposition running through families
is evident. Identical twins invariably develop type 2 diabetes when exposed to
the same environmental factors. In genetically predisposed individuals several environmental
factors precipitate the onset of diabetes.
Important
among these are obesity, physical inactivity, repeated pregnancies, infections,
physical or psychological stress and diabetogenic drugs. Birth of large babies weighing
above 4 kg is a strong pointer to the subsequent development of diabetes in the
mother.
Obesity
The current
obesity epidemic due to the modern sedentary life and caloric abundance is a
major factor that predisposes to type 2diabetes. Hence it is invariably seen that
type 2 diabetes is closely related to obesity. Obese subjects show a relative
resistance to the action of insulin due to a reduction in the number of insulin
receptors on the target cells. The full complement of receptors is restored on
shedding the excess weight.
There is an
association between low birth weight in infancy and occurrence of IGT or DM in
young adulthood. Increase in the body mass index (BMI) after the age of 2 years
is also associated with the chance to develop DM.
Physical Inactivity
It seems to
act as a factor favoring the onset of type 2 diabetes. Many of the diabetics
are physically inactive. Physical exercise improves their exercise tolerance.
Role of
Insulin antagonists: Glucose metabolism is delicately balanced by the coordinated
effects of insulin antagonist hormones like glucagon, cortisol, catecholamines and
growth hormone. Several other hormones also take part in the metabolism of
carbohydrates. Imbalance of this hormonal profile results in carbohydrate intolerance.
Other
antagonists to insulin: Antibodies to insulin may develop in individuals who
are on treatment with insulins especially the animal insulins. The antibodies
inactivate endogenous as well as administered insulin. Such patients show
progressive insulin resistance. Fatty acids which compete with carbohydrate for
metabolism in muscle lead to insulin resistance. In hyperlipidemia insulin
dependent carbohydrate metabolism suffers and a relative insulin resistance
develops.
Thus it
would seem that persons are predisposed to develop type 2 diabetes by
genetically. However lifestyle factors will determine the onset, age of onset,
severity of the metabolic defect and further course.
PATHOLOGICAL CHANGES
Pancreas: In
type 1 diabetes the beta cells of the islets of Langerhans show reduction in
number, degranulation and hyalinization. In recent onset type 1 DM lymphocytic infiltration
of the islets occurs and this may be caused by viral infection. Inflammation is
seen particularly around the beta cells only and not around the other types of
cells.
In type 2 DM
during the early phase the beta cells are normal in number or only slightly
reduced. The beta cells lose their sensitivity to the hyperglycemic stimulus
for releasing insulin. As a result insulin secretion loses its smooth and fine
relationship with glucose level. It tends to be erratic. In the early stages of
evolution of type 2 DM—the reduction in the sensitivity of the receptors is compensated
by overproduction of insulin and accompanying hyperinsulinemia. Frank diabetes
results when beta cells starts failing and insulin production comes down.
Insulin
resistance in muscle develops early in persons who would develop type 2
diabetes later. Beta cell function starts deteriorating about 10 years before
the onset of DM, by which time the beta cell function has fallen to 30% or
less. Acanthosis nigricans is a cutaneous marker of hyperinsulinemia. Both
impaired fasting glucose (1FG) and
impaired
glucose tolerance (IGT) lead to type 2 diabetes in a variable proportion of patients.
Several
factors account for the frequency and time of onset of complications in
diabetes. These include theabnormalities of glucose levels, genetic factors,
smoking, obesity, hypertension, hyperlipidemia and others.
Vascular Changes
Diabetics show
a predisposition to develop vascular lesions affecting both small and large
blood vessels. In microangiopathy, there is specific involvement of the small
blood vessels. Venules, capillaries and arterioles are affected in this
process. There is deposition of PAS (periodic acid Schiff) positive material in
the capillary basement membrane. Glycosylation of several proteins in the
vessel wall results in increased permeability. The basement membrane is
thickened. Ultimately there is vascular occlusion.
Microangiopathy
is most marked in type 1, developing early in life but also occurs in type 2.
Various factors like endothelial damage, increased plasma viscosity,
erythrocyte aggregation, reduced red cell deformability and increased platelet
adhesion lead to microangiopathy. The problem is more complex and the entire
process is still not fully understood. Microangiopathy affects several organ
systems. The main lesions are seen in the retina; kidneys, peripheral nerves and
heart giving rise to diabetic retinopathy, nephropathy, many forms of diabetic
neuropathy and cardiomyopathy.
Macroangiopathy
The diabetic
is prone to develop occlusive vascular disease in medium sized arteries such as
the coronary, cerebral and peripheral limb vessels. The process is one of atheroma
which sets in at younger ages and is more extensive than that occurring in non
diabetics. These lesions lead to increased risk of ischemic heart disease, cerebrovascular
accidents and ischemia to the limbs with intermittent claudication and peripheral
gangrene. Macroangiopathy largely accounts for the steep rise in mortality in
middle-aged diabetics.
Retinopathy
Diabetes
mellitus produces a classical retinopathy. A specific change occurs in the
vessels leading to loss of mural cells (pericytes) and the formation of micro aneurysms.
The occurence of retinopathy is related more to the duration of the disease
than to the severity. Once initiated the fundus changes are usually
progressive. The early changes are venous dilation and the appearance of small dot
like micro aneurysms in the perimacular area.
Arterial
blood is shunted and this leads to ischemia of the retina. Increased vascular
permeability accounts for the formation of exudates. In the next stage dot and
blot hemorrhages predominate. Large subhyaloid hemorrhages and vitreous
hemorrhages may develop and vision is seriously impaired. Such hemorrhages are
due to rupture of newly formed blood vessels. As these hemorrhages are absorbed,
organization by fibrous tissue results and multiple bands of retinitis
proliferans develop. These lead to permanent visual impairment. The fibrous
bands may contract giving rise to retinal detachment. Leaking vessels in the
retina can be demonstrated by fluorescein angiography.
Retinopathy
is usually associated with advanced nephropathy. Sometimes in diabetic
ketoacidosis with severe hyperlipidemia the fat gives a milky white appearance
to the retinal arteries called “lipemia retinalis”
Renal Lesions
These are
commonly seen in subjects who have had diabetes for over 15-20 years. Vascular
changes include (i) arteriosclerosis of the renal artery, (ii) sclerosis of the
arterioles and (iii) glomerulosclerosis. Glomerulosclerosis may be nodular
(Kimmelstiel-wilson lesion) or diffuse. There is accumulation of PAS positive eosinophilic
material within the mesangium. There is thickening of the glomerular capillary
basement membrane. The establishment of glomerulosclerosis is indicated by the
presence of proteinuria. Further damage to the glomeruli results in the
development of chronic renal failure.
Distant
stages can be defined in the evolution of diabetic nephropathy. In the initial
stages, asymptomatic microalbuminuria in which up to 200 mcg/minute of albumin
may be lost in the urine. Normal subjects do not lose more than 20 mcg/min or
300 mg of protein in 24 hours. Microalbuminuria is not detectable by the
ordinary laboratory tests. In type 1 DM there is elevation of systotic BP
during sleep preceding micro albuminuria. This rise in BP is an important
contributory factor in the development of structural changes in the kidneys. It
is absolutely necessary to control blood pressure also along with blood sugar
to prevent deterioration.
In the early
stage the kidneys are enlarged, more vascular and the glomerular filtration
rate (GFR) is increased. In the second stage, there is microalbuminuria and in
third stage the proteinuria is more pronounced and easily detectable by routine
tests. Loss of 3.5g or more of protein in 24 hours may lead to the development
of nephrotic syndrome. Hypertension develops during this stage. In the fourth
stage further structural changes develop and the glomerular filtration rate
comes down with gradual increase in the blood levels of metabolic waste
products such as creatinine and urea. The fifth stage is one of gross reduction
of glomerular filtration and overt renal failure with azotemia, severe
hypertension and complications such as cardiac failure and end stage renal failure.
Autonomic neuropathy may lead to functional obstruction of the bladder,
retention with over flow, urinary infection and further deterioration of renal functions.
Another system of classification is based on creatinine clearance.
The diabetic
patient is predisposed to develop urinary infection and therefore acute and chronic
pyelonephritis are very common. Fulminant urinary infection leads to ischemic
necrosis of the renal papillae. This presents as acute anuric renal failure.
Fleshy masses may be passed in the urine. These are the necrosed papillae and
the condition is called papillitis necroticans ulcerans.
Emphysematouspyelonephritis is another serious complication.
Peripheral Nerves
In the
myelinated nerve fibers, axonal atrophy was considered to be the primary
lesion, secondary to ineffective axonal transport. Axoglial dysfunction, and abnormalities
of paranodal connections between the terminal myelin loops and the axonal
membrane have also been described. This could explain the reduction in nerve conduction
velocity. This improves with therapeutic inhibition of aldose reductase. More
recent studies, however provide evidence for the presence of demyelination and
hence Schwann’s cell involvement is the primary lesion. As the myelinated
fibers degenerate, there is an attempt to regenerate, which manifests in the form
of regeneration clusters. With progress of the neuropathy the density of the
regeneration clusters also comes down. Structural abnormalities have also been
found in the vessels supplying the nerve fibers. The epineural vessels show
arteriolar attenuation, venous distension, arteriovenous shunting and new
vessel formation along with intimal hyperplasia and hypertrophy, denervation
and reduction in neuropeptide expression. The perineural vessels also
demonstrate basement membrane thickening and endothelial cell hypertrophy and
hyperplasia. There is also a reduction in capillary density and occurrence of pericyte
loss with reduction of endoneural oxygen tension and blood flow to the nerves.
CLINICAL FEATURES
The clinical
manifestations of diabetes are protean. Though the symptoms are similar in both
types of diabetes, in type 1 they develop acutely whereas in the majority of
the type 2 the onset is insidious. Type 1 patients are usually below the age of
30, thin and emaciated and unless promptly treated with insulin, they would
develop ketoacidosis.
Due to the
high prevalence of obesity, type 2 diabetes is occurring at earlier ages as a
global phenomenon, especially in developed countries.
Type 2
patients are generally above the age of 30, obese, usually asymptomatic and may
present directly with the vascular complications of diabetes. Around 50% of the
cases present with the classical symptoms of polyuria, polyphagia and weight
loss. These symptoms can be directly correlated with hyperglycemia and glycosuria.
Other clinical presentations which warrant full investigation to exclude
diabetes are (i) non-healing ulcers (ii) recurrent respiratory or urinary tract
infections (iii) Rapid changes in refraction of the eyes (iv) steady and unexplained
rapid weight loss (v) increased tendency for fungal infections like moniliasis,
balanoposthitis and vulvitis; (vi) unexplained peripheral neuropathy (vii)
premature onset of ischemic heart disease, stroke or vascular occlusions (viii)
history of overweight babies and recurrent fetal loss in women (ix) premature
cataract often below the age of 50 years and retinopathy (x) impotence in
males, and (xi) any vague ill-health. In some cases, diabetics may present to
the doctor for the first time with any of the major emergencies, without any apparent
illness previously.
DIAGNOSIS
Diabetics
with classic symptoms can be diagnosed clinically, but since many cases may be
asymptomatic, diabetes should be suspected even in the absence of symptoms. The
clinical symptoms and the biochemical alterations do not go hand in hand in
many cases. Diabetes being mainly a biochemical disease with several different but
inter-related biochemical and molecular abnormalities, should always be
diagnosed and managed with biochemical monitoring along with clinical
examination.
Fasting
plasma glucose levels above 126 mg/dL (6.7 mmol/L) or postprandial plasma
glucose levels above 200 mg/dL are diagnostic. It is always better to do
bothestimations to confirm the diagnosis.
Estimation
of FBS and PPBS has become mandatory investigations in all health check up
examinations.
Urine tests: These tests can be used for initial
screening and follow-up of cases under treatment. Urinary glucose does not
always directly reflect the blood glucose level. The value of urine examination
cannot be underestimated since protenuria, ketonuria and the microscopic
abnormalities can be detected only by examining the urine.
Glucose in
urine is tested by the Benedict’s test and Clinitest (Chemtab), which detect
reducing substances non-specifically. While glucose is by far the most common reducing
substance in urine, the possibility of other reducing substance should be kept
in mind and the enzyme methods (employing glucose oxidase) which are specific for
glucose (Clinistix, Diastix) should be employed. If the Benedict’s test is
positive and the glucose oxidase is negative, the presence of other reducing substances
such as ascorbic acid, aspirin and lactose should be suspected.
Blood glucose estimation: Various methods are employed to
estimate the blood glucose. The methods using copper reduction (Folin-Wu or
Nelson Somogyi) also detect the reducing substances like uric acid, creatinine
and hence their values are 20-30 mg/dL higher than those obtained by the
glucose oxidsae method which gives the true glucose values. Highly accurate and
rapid (1-2 min) devices are now available based on immobilized glucose oxidase
electrodes. Hexokinase and glucose dehydrogenase methods are used for
reference. Blood sugar estimations are mandatory for confirming the diagnosis of
diabetes. Both fasting and postprandial values should be estimated. In mild
diabetes the fasting blood sugar values may be below 126 mg /dL and therefore
the diagnosis is likely to be missed if only the fasting blood sugar is
estimated.
Glucose tolerance test (GTT): The oral glucose tolerance test
(OGTT) is mainly used for diagnosis of diabetes when blood glucose levels are
equivocal, during pregnancy, or in an epidemiological setting to screen for
diabetes and impaired glucose tolerance.
The OGTT
should be administered in the morning after at least 3 days of unrestricted
diet (greater than 150 g of carbohydrate daily) and usual physical activity.
The test should be preceded by an overnight fast of 8-14 h. during which period
only water may be drunk. Smoking is not permitted during the test. The presence
of factors such as medications, inactivity and infection that influence interpretation
of the results of the test must be recorded.
After
collection of the fasting blood sample, the subject should drink 75 g of
anhydrous glucose dissolved in 250-300 mLof water over the course of 5 minutes.
For children, the test load should be 1.75g of glucose per kg of body weight,
up to a maximum of 75g of glucose. Blood samples should be once again collected
2 hr after the test load.
If there is
delay in estimation of glucose the blood samples should be collected in a tube
containing sodium fluoride (6 mg/mL of whole blood) and immediately centrifuged
to separate the plasma. In subjects having symptoms of diabetes, a single
fasting value above 126 mg/dL or a 2-hour blood glucose value above 200 mg/dL
after 75 g of glucose oral may be taken to be diagnostic. In asymptomatic
subjects at least two abnormal blood glucose values should be insisted upon to
confirm the clinical diagnosis.
TREATMENT
The aim of treatment is to achieve normal blood glucose levels throughout day and night, to alleviate symptoms and to prevent complications. The four pillars of diabetic management are diet, exercise, drugs and patient education, backed up by regular monitoring of glycemic control and early detection and treatment of complications.
DIABETES MELLITUS – General Characteristics, Pancreas, Classification, Etiopathogenesis, Pathological Changes, Clinical Features, Diagnosis and Treatment
A
Psychiatric nurse faces various challenges because of changes in the inpatient
care approach. Some of these changes that affect her role are as follows:
Trends in Health Care
Increased mental health problems
Provision for quality and
comprehensive services
Multidisciplinary team approach
Providing continuity of care
Care provided in alternative settings
Economic
Issues
Industrialization
Urbanization
Raised standard of living
Changes in Illness Orientation
Shift from illness to prevention
(modification of style), specific to holistic, quantity of care to quality of
care
Changes in Care Delivery
Care delivery is shifted from
institutional services to community services, genetic services to counseling
services, nurse patient relationship to nurse-patient partnership.
Information Technology
Telenursing
Telemedicine
Mass media
Electronic systems
Nursing informatics
Consumer Empowerment
Increased consumer awareness
Awareness of the community in early detection
and treatment of mental illness as well as proper utilization of available
psychiatric hospitals
Patients are health care consumers
demanding quality health care services at affordable cost with less restrictive
and more humane rates.
Deinstitutionalization
Bringing mental health patients out
of the hospital and shifting care to community.
Physician Shortage and Gaps in Service
Physician shortage can provide the
opportunity for new roles, for example, nurse practitioner. In respect to gaps
in services, nurses always meet the needs of people for whom services are not
available, for example, home visiting nurse.
Demographic Changes
Increasing number of the elderly
group
Type of family (Increased number of
nuclear families).
Change in Patient Needs
Wanting a more holistic orientation
in health care.
Challenges in Psychiatric Nursing
Knowledge development, dissemination
and application
Overcoming stigma
Health care delivery system issues
Impact of technology
Educational Programs for the Psychiatric Nurse
Diploma in Psychiatric Nursing (The
first program was offered in 1956 at NIMHANS, Bengaluru)
MSc in Psychiatric Nursing (The first
program was offered in 1976 at Rajkumari Amrit Kaur College of Nursing, New
Delhi)
Mphil in Psychiatric Nursing (1990,
MG University, Kottayam)
Doctorate in Psychiatric Nursing
(offered at MAHE, Manipal; RAK College of Nursing, Delhi; NIMHANS, Bengaluru,
National Consortium for PhD in Nursing under RGUHS, Karnataka, etc)
Short term training programs for both
the degree and diploma holders in nursing
Standards of Mental Health Nursing
The
development of standards for nursing practice is a beginning step towards the
attainment of quality nursing care. The adoption of standards helps to clarify
nurses areas of accountability, since the standards provide the nurse, the
health agency, other professionals, patients, and the public, with a basis for
evaluating practice. Standards also define the nursing profession’s
accountability to the public. These standards are therefore a means for
improving the quality of care for mentally ill people.
Development of Code of Ethics
This is very
important for a psychiatric nurse as she takes up independent roles in
Psychotherapy, behavior therapy, cognitive therapy, individual therapy, group therapy,
maintains patient’s confidentiality, protects his rights and acts as patient’s
advocate.
Legal Aspects in Psychiatric Nursing
Knowledge of
the legal boundaries governing psychiatric nursing practice is necessary to
protect the public, the patient, and the nurse. The practice of psychiatric
nursing is influenced by law, particularly in its concern for the rights of
patients and the quality of care they receive.
The
patient’s right to refuse a particular treatment, protection from confinement,
intentional torts, informed consent, confidentiality, and record keeping are a
few legal issues in which the nurse has to participate and gain quality
knowledge.
Promotion of Research in Mental Health Nursing
The nurse
contributes to nursing and the mental health field through innovations in
theory and practice and participation in research.
Cost-effective Nursing Care
Studies need
to be conducted to find out the viability in terms of cost involved in training
a nurse and the quality of output in terms of nursing care rendered by her.
Focus of Care
A psychiatric nurse has to focus care on certain target groups like the elderly, children, women, youth, mentally retarded and chronic mentally ill.
Urine Testing Uses – Purpose, Characteristics, Examination, Preliminary Assessment, Equipment, Procedure, Urine pH, Gravity, After Care
UPDATED 2024
Urine testing, also known as urinalysis, is a diagnostic test that involves analyzing a person’s urine for various markers, compounds, and characteristics. This type of testing can provide valuable information about a person’s overall health, help diagnose medical conditions, and monitor the effectiveness of treatments.
USES OF URINE TESTING
Here are some common uses of urine testing:
Drug Testing: Urine tests are frequently used to screen for the presence of drugs and their metabolites. This is common in workplaces, athletic organizations, and legal situations.
Medical Conditions: Urinalysis can help diagnose various medical conditions, such as diabetes, kidney diseases, urinary tract infections (UTIs), and liver problems. Abnormal levels of glucose, protein, blood cells, or other substances in the urine may indicate an underlying health issue.
Pregnancy Testing: Urine tests are often used to detect the presence of human chorionic gonadotropin (hCG), a hormone produced during pregnancy. Home pregnancy tests typically use urine samples for this purpose.
Kidney Function: Urine tests can provide information about kidney function by measuring levels of creatinine, urea, and other substances. Changes in these levels can indicate kidney problems.
Metabolic Disorders: Certain metabolic disorders, such as phenylketonuria (PKU) or maple syrup urine disease (MSUD), can be diagnosed through urine testing.
Monitoring Medications: Some medications can be monitored through urine testing to ensure that they are at therapeutic levels and not causing adverse effects.
URINE TESTING
Urine
analysis methods comprise testing reaction, specific gravity, albumen, sugar,
bile, acetone, pus, blood and yeasts microscopically
Purpose
To detect reaction, in cystitis the
reaction is alkaline
To detect sugar, it is present in
diabetes mellitus
To detect – protein it is present in
kidney damage, pre-eclampsia and is called proteinuria
To detect acetone, it is present due
to incomplete metabolism of fat
To detect bile – it is seen in cases
of obstructive jaundice or hemolytic diseases
To detect pus cells – it is present
due to urinary tract infection
To detect blood – it is seen in snake
bite, fracture pelvis, etc
Characteristics of Normal Urine
Volume: 1,000 to 2,000 ml in 24 hours
Appearance: clear
Odor: aromatic color
Color: amber or pale straw in color
Reaction: normal urine is slightly
acidic
Specific gravity: 1.010 to 1.025
Constituents of the normal urine:
water 96 percent, urea 2% and uric acid, urates, creatinine, chlorides,
phosphates, sulfates, oxalates – 2%
Characteristics of Abnormal Urine
Volume
Polyuria – increased in volume
Oliguria – decreased in volume
Anuria – total absence or marked
decrease of urine
Suppression – failure of the kidney
to secrete urine
Color
Green or brownish yellow – bile salts
and bile pigments
Reddish brown – urobilinogen
Bright red – a large amount of fresh
blood
Smokey brown – blood pigment
Milk white – chyluria due to filariasis
Appearance
Mucus – appears as a flocculent cloud
Pus – settles at the bottom as a
heavy cloud
Stones – as fine sand
Uric acid – as grains of pepper
Odor
Sweetish or fruity odor – seen in
diabetes
Reaction
Alkaline – cystitis
Specific gravity
Diabetes mellitus – increased
specific gravity
Renal disease – low specific gravity
Constituents of urine
Kidney damage – albumin
Types of Examination of the Urine
Physical examination: color
appearance, volume, reaction, specific gravity and color
Chemical examination: routine tests
such as for albumin and sugar. Special tests such as tests for acetone, bile
pigments and bile salts. Microscopic examination – crystals, casts, RBC, pus
cells, epithelial and bacteria
Preliminary Assessment
The doctor order for any instructions
Articles available in the unit
General condition and diagnosis of
the patient
Self-care ability of the patient
Preparation of the Patient and Environment
Explain the procedure to the patient
Keep the urine sample ready
Arrange the articles ready in the
treatment
Provide labeled container for
collecting urine
Equipment
Test tubes 4 to 6 on a test tube
Test tube holder – 1
Spirit lamp – 1
Match box – 1
Kidney tray with lining to discard
the wastes
Duster or rag piece – to wipe the
outside of the test tube before heating
Acetic acid – to test urine for
albumin
Nitric acid or sulfosalicyclic acid –
to test urine for albumin
Red and blue litmus paper – to test
the reaction of the urine
Urinometer – to measure the specific
gravity of the urine
Benedict’s solution – to test urine
for sugar
Ammonium sulfate crystals, sodium
nitroprusside crystals and liquor ammonia to test urine for acetone
Weak solution of Tr. Iodine to test
for bile pigments
Sulfur powder: to test for bile salts
Glass jar: to measure the amount of
the urine
Pipette – 2 – to measure drops of
urine and reagents
A small bottle brush – to clean the
test tubes
Procedure
Sugar Test
Take test tube and fix in holder
Pour 5 ml of Benedict’s solution into
test tube
Light spirit lamp and heat Benedict
solution till it boils
Holding test tube mouth facing away
from nurse
Add 8 drops of urine using dropper
and allow boiling for few seconds
Put off flame and cool test tube
under running water
Observations
Blue: Nil
Green: +
Yellow: ++
Orange: +++
Brick red: ++++
Albumin Test
A hot test
Fill 2/3 of test tube with urine,
secure test tube holder at very top
Heat the upper third of test tube
over flame
If there is precipitation, it denotes
the presence of wither protein or phosphate
Add 2-4 drops of 2 percent acetic
acid
If precipitate dissolves it is due to
phosphates present in normal urine
If precipitate does not dissolve it
denotes presence of albumin
Observation
Trace: +
Cloudy:++ (100mg/dL)
Thick cloudiness: +++ (500 g/dL)
Cold Test
Pour a small quantity of nitric acid
or sulfosalicylic acid 3 percent in to a clean test tube
Allow equal quantity of urine to
trickle down the sides of the test tube
If albumin present, a white
precipitate will be seen where two fluids meet
Urine pH
Collect and keep ready with urine
sample
Dip litmus strip in urine and keep
for one minute
Note color change
Discard strip into container for
infected waste
Urine Specific Gravity
Fill 3/4 of jar with urine
Gently place urinometer into jar
When urinometer stops bobbing
Read specific gravity directly from
scale marked on calibrated stem of urinometer
Make sure that instrument floats
freely and does not touch sides of jar
Read scale at lowest point of
meniscus to ensure an accurate reading at eye level
Rothera’s Test (Acetone)
Take 2 cm depth of ammonium sulfate
crystals in a small test tube
Add equal volume of urine and one
crystal of sodium nitroprusside
Close the test tube with a cork and
shake the test tube
Take liquor ammonia and add it to the
urine, trickling through the sides
Read the results immediately
Observations
If acetone
is present permanganate purple colored ring is formed at the junction of urine
and ammonia
Hays Test (Bile Salts)
Take a test tube, half full of urine
Sprinkle sulfur powder on the surface
of the urine
If the powder sinks down to the test
tube, it indicates the presence of bile salts
Smith’s Test (Bile Pigments)
Fill 3/4 of test tube with urine
Add iodine drops along the sides of
the tube, so as to form a layer on the surface of the urine
A green color at the junction of the
two liquids indicates the presence of bile pigments
After Care
Discard the urine in the sluice room
Wash the test tube with soap and
water
Dry the tube, holder and urinometer
with jar
Replace the article after cleaning
Wash hands thoroughly
Record the procedure in the nurse’s record sheet and dietetic chart
Urine Testing – Purpose, Characteristics, Examination, Preliminary Assessment, Equipment, Procedure, Urine pH, Gravity, After Care
TEMPERATURE TECHNIQUES – Principles, Equipment and Procedure (COMMUNITY HEALTH NURSING)
UPDATED 2024
A clinical
thermometer is a special instrument designed to measure the temperature of the
body. Two thermometers – one oral and one rectal – are essential equipment
which the nurse always carries in her bag. Elevation in temperature is an
indication that the body is reacting to an infection
PRINCIPLES
Meticulous cleaning of thermometer
before and after use is essential to prevent the spread of infection
Temperature is usually taken by
mouth. Rectal temperatures are most accurate while auxillary temperatures are
least accurate
Shake the mercury to 95 degree F
before taking the temperature
Keep all thermometers in the shade
and in the coolest part of the building
Accuracy in temperature helps in
effective treatment and medical decision
EQUIPMENT
Ten small cotton swabs
Kidney basin to hold moist cotton
swabs
Thermometer
Lubricant for rectal temperature
Paper bag
PROCEDURE
Use bag technique as per standard
precautions
Remove the thermometer swab up to
bulb and read
Place the thermometer at proper site
Rinse the thermometer thoroughly
under cool running water after reading
Replace it in the community bag and
wash hands
Record it in the TPR sheet
TEMPERATURE TECHNIQUES – Principles, Equipment and Procedure (COMMUNITY HEALTH NURSING)
CHOLECYSTOGRAPHY – Purpose, Preparation of the Patient, Procedure, After Care and Complications
UPDATED 2024
Cholecystography
is a test for gallbladder disease, done by visualizing the gallbladder.
Visualization of the gallbladder depends upon absorption of the dye from the
intestinal tract, isolation and excretion by the liver cells and a free passage
way from the liver to the gallbladder.
PURPOSE
To detect gallstones
To test the contractibility of the
gallbladder
To find out filling ability of the
gallbladder
To find out its ability to
concentrate, its contents, and its condition when it is empty in normal states
PREPARATION OF THE PATIENT
Explain the procedure to the patient
to relieve tension and worries
Stop medications which contain iodine
compounds and bismuth three days prior to the test
Check whether the patient is allergic
to iodine or sea food before giving the dye
Record the patient’s weight to
calculate the dose of the dye
The patient is given a low-fat
evening meal to avoid gallbladder contraction. Thereafter, no food and water
should be given to the patient until the X-ray examinations are complete
The bowel is cleansed with saline
enema
The emergency drugs and resuscitation
equipment should be kept ready to resuscitate the patient
PROCEDURE
The patient is given a light diet at
7 pm without fat
A laxative like dulcolax is given to
clear the bowels
At 10 pm the patient is given 6
telepaque tablets to swallow
This dye is opaque to X-rays and is
absorbed from the intestines, and is excreted by the liver
When the gallbladder is normal, this
dye gets concentrated in the gallbladder, which becomes visible by X-ray
X-ray pictures are taken on the
following day approximately 14, 18 and 19 hours after the drug has been
administered, i.e. at 12 noon. 4 pm and 5 pm
No food is given during this period
Then, to test the contractibility of
the gallbladder, the patient is fed with a fatty meal, one hour before the last
X-rays taken at 12 noon and 4 pm, but it empties itself after the fatty meal
taken at 4 pm and is, therefore, not visible in the X-ray taken at 5 pm
An abnormal gallbladder may not get
filled properly or may fail to empty itself
AFTER CARE
Observe the patient for allergic
reactions. Check the vital signs of the patient
Accompany the patient throughout the
procedure
Make the patient comfortable
COMPLICATIONS
Severe
reactions to dye may lead to:
Respiratory difficulty
Urticaria
Shock
Collapse
CHOLECYSTOGRAPHY – Purpose, Preparation of the Patient, Procedure, After Care and Complications
THERAPEUTIC COMMUNICATION – Principles or Characteristics, Techniques and Non-therapeutic Communication
UPDATED 2024
Therapeutic
communication is an interpersonal interaction between the nurse and the patient
during which the nurse focuses on the patient’s specific needs to promote an
effective exchange of information. All nurses need skills in therapeutic
communication to effectively apply the nursing process and to meet standards of
care for their patients.
Therapeutic
communication can help nurses to accomplish many goals:
Establish a therapeutic nurse-patient
relationship
Identify the most important patient’s
needs
Assess the patient’s perception of
the problem
Facilitate the patient’s expression
of emotions
Implement interventions designed to
address the patient’s needs
To have an effective therapeutic communication, the nurse
must consider privacy and respect of boundaries, use of touch and active
listening and observation.
Principles or Characteristics of Therapeutic Communication
The patient should be the primary
focus of interaction
A professional attitude sets the tone
of the therapeutic relationship
Use self-disclosure cautiously and
only when it has a therapeutic purpose
Avoid social relationship with
patients
Maintain patient confidentiality
Assess the patient’s intellectual
competence to determine the level of understanding
Implement interventions from a
theoretic base
Maintain a nonjudgmental attitude.
Avoid making judgments about patient’s behavior
Avoid giving advice
Guide the patient to reinterpret his
or her experiences rationally.
Therapeutic Communication Techniques
Listening: It is an active process of
receiving information. Responses on the part of the nurse, such as maintaining
eye-to-eye contact, nodding, gesturing and other forms of receptive nonverbal
communication convey to the patient that he is being listened to and understood.
Therapeutic Value: Nonverbally communicates to the patient the nurse’s
interest and acceptance.
Broad Openings: Encouraging the
patient to select topics for discussion. For example, “What are you thinking
about?”
Therapeutic Value: Indicates acceptance by the nurse and the value of
patient’s initiative.
Restating: Repeating the main thought
expressed by the patient. For example, “You say that your mother left you when
you were 5-year-old”
Therapeutic Value: Indicated that the nurse is listening and validates,
reinforces or calls attention to something important that has been said.
Clarification: Attempting to put
vague ideas or unclear thoughts of the patient into words to enhance the
nurse’s understanding or asking the patient to explain what he means. For
example, “I am not sure what you mean. Could you tell me about the again?”
Therapeutic Value: It helps to clarify feelings, ideas and perceptions of
the patient and provides an explicit correlation between them and the patient’s
actions.
Reflection: Directing back the
patient’s ideas, feelings, questions and content. For example, “You are feeling
tense and anxious and it is related to a conversation you had with your husband
last night”.
Therapeutic Value: Validates the nurse’s understanding of what the
patient is saying and signifies empathy, interest and respect for the patient.
Humor: The discharge of energy
through comic enjoyment of the imperfect. For example, “That gives a whole new
meaning to the word ‘nervous’”, said with shared kidding between the nurse and
the patient.
Therapeutic Value: Can promote insight by making repressed material
conscious, resolving paradoxes, tempering aggression and revealing new options,
and is a socially acceptable for of sublimation.
Informing: The skill of information
giving. For example,” I think you need to know more about your medications.”
Therapeutic Value: Helpful in health teaching or patient education about
relevant aspects of patient’s well-being and self-care.
Focusing: Questions or statements that
help the patient expand on a topic of importance. For example, “I think that we
should talk more about your relationship with your father”.
Therapeutic Value: Allows the patient to discuss central issues and keeps
the communication process goal-directed.
Sharing Perceptions: Asking the
patient to verify the nurses understanding of what the patient is thinking or
feeling. For example, ”You are smiling, but I sense that you are really very
angry with me”.
Therapeutic Value: Conveys the nurse understands to the patient and has
the potential for clearing up confusing communication.
Theme
Identification: This involves identification of underlying issues or problems
experienced by the patient that emerge repeatedly during the course of the
nurse-patient relationship. For example, “I noticed that you said, you have
been hurt or rejected by the man. Do you think this is an underlying issue?”
Therapeutic
Value: It allows the nurse to promote the patient’s exploration and
understanding of important problems.
Silence:
Lack of verbal communication for a therapeutic reason. For example, sitting
with a patient and nonverbally communicating interest and involvement.
Therapeutic
Value: Allows the patient time to think and gain insight, slows the pace of the
interaction and encourages the patient to initiate conversation while enjoying
the nurse’s support, understanding and acceptance.
Suggesting:
Presentation of alternative ideas for the patient’s consideration relative to
problem solving. For example, “Have you thought about responding to your boss
in a different way when he raises that issue with you? You could ask him if a
specific problem has occurred.”
Therapeutic
Value: Increases the patient’s perceived notions or choices.
Ineffective/Non-therapeutic Communication
These include failure to listen, conflicting verbal or non-verbal messages, a judgmental attitude, false reassurance, giving of advice, the inability to receive information because of a preoccupation of impaired thought process and changing of the subject if one becomes uncomfortable with the topic being discussed.
THERAPEUTIC COMMUNICATION – Principles or Characteristics, Techniques and Non-therapeutic Communication