LARYNX CANCER – Types, Etiology and Risk Factors, Signs and Symptoms, Diagnostic Evaluation and Management
Throat cancer refers to cancerous tumors that develop in throat (pharynx), voice box (larynx) or tonsils
TYPES OF LARYNX CANCER
Throat cancer is a general term that applies to cancer that develops in the throat (pharyngeal cancer) or in the voice box (laryngeal cancer). The throat and the voice box are closely connected, with the voice box located just below the throat.
Though most throat cancers involve the same types of cells, specific terms are used to differentiate the part of the throat where cancer originated
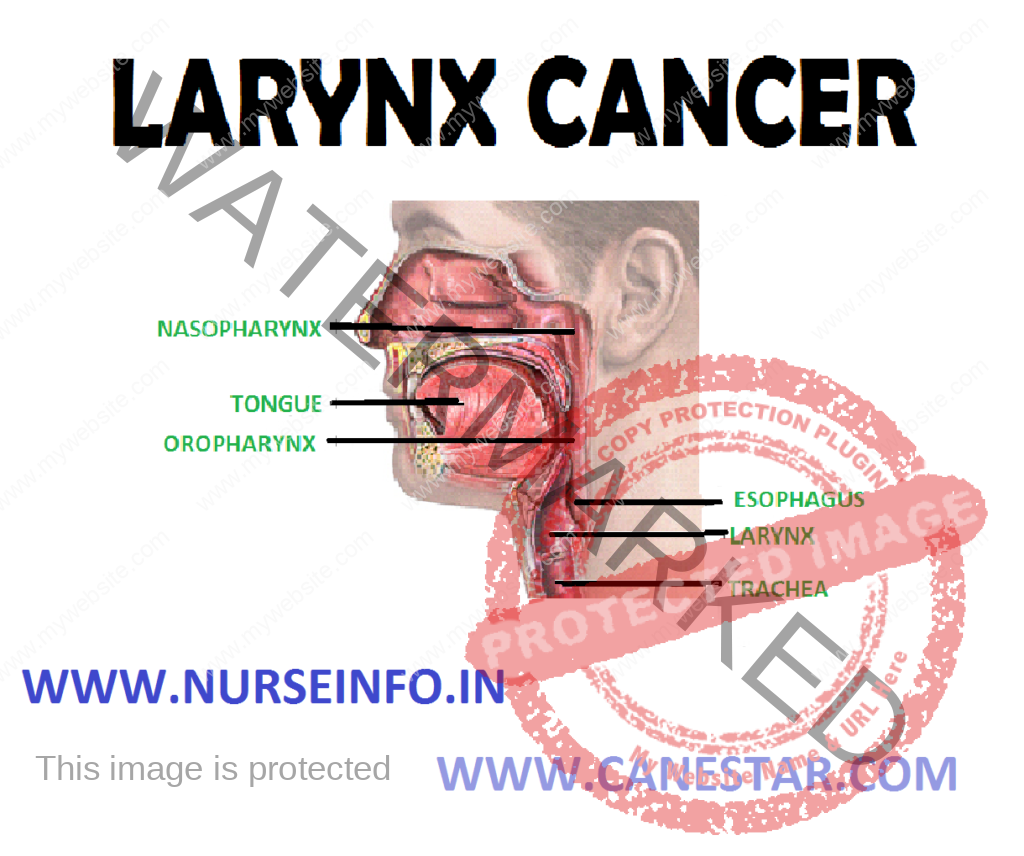
- Nasopharyngeal cancer begins in the nasopharynx
- Oropharyngeal cancer begins in the oropharynx
- Hypopharyngeal cancer (laryngopharyngeal cancer) begins in the hypopharynx
- Glottic cancer begins in the vocal cords
- Supraglottic cancer begins in the upper portion of the larynx and includes cancer that affects the epiglottis
- Subglottic cancer begins in the lower portion of voice box and below vocal cords
- Cancers that start in gland cells (adenocarcinoma): adenocarcinoma is uncommon compared to squamous cell laryngeal cancer. It starts in the adenomatous cells that are scattered around the surface of the larynx. Adenomatous cells are gland cells that produce mucus
- Connective tissue cancers (sarcoma): sarcomas are cancers that start in the body’s connective tissues. These are the supporting tissues of the body, such as bone, muscle, and nerves. Cartilage is the supporting tissue of the larynx. Cancers that develop from cartilage are called chondrosarcomas
TNM STAGES OF CANCER OF THE LARYNX
TNM stands for Tumor, Node and Metastasis. The system describes:
- The size of a primary tumor (T)
- Whether the lymph nodes have cancer cells in them (N)
- Whether the cancer has spread to a different part of the body (M)
The exact T staging of laryngeal cancer varies depending on which part of the larynx is involved. The cancer may start on the vocal cords (glottis), above the vocal cords (supraglottis), or below the vocal cords (subglottis)
Early-Stage Laryngeal Cancer (T0-T2)
- T Stage 0, Tis
In early cancer of the larynx, this means there are abnormal cells that may be precancerous. Tis (tumor in situ) means an early tumor that has not broken through the basement membrane of the tissue it is growing in
- T stage 1
T stage 1 means the tumor is in only one part of the larynx and the vocal cords are able to move normally
- T stage 2
T stage 2 means the tumor which may have started on the vocal cords (glottis), above the vocal cords (supraglottis), or below the vocal cords (subglottis) has grown into another part of the larynx. In cancer of the vocal cords (glottic cancer), stage T2a means that the vocal cords move normally
Locally Advanced Laryngeal Cancer (T2b-T4)
- Glottic cancer T stage 2b
In T stage 2b in cancer that starts in the vocal cords (glottis), the vocal cord movement is limited
- T stage 3
T stage 3 means the tumor is throughout the larynx but has not spread further than the covering of the larynx
- T stage 4
T stage 4 means the tumor has grown into body tissues outside the larynx. It may have spread to the thyroid gland, windpipe (trachea) or food pipe (oesophagus)
N-Stages of Laryngeal Cancer
There are 4 main lymph node stages in cancer of the larynx. N2 is divided into N2a, N2b and N2c. the important points here are whether there is cancer in any of the nodes and, if so, the size of the node and which side of the neck it is on.
- N0 means there are no lymph nodes containing cancer cells
- N1 means there are cancer cells in one lymph node on the same side of the neck as the cancer, but the node is less than 3 cm across
- N2a means there is cancer in one lymph node on the same side of the neck and it is between 3 cm and 6 cm across
- N2b means there is cancer in more than one lymph node, but none are more than 6 cm across. All the nodes must be on the same side of the neck as the cancer
- N2c means there is cancer in lymph nodes on the other side of the neck from the tumor, or in nodes on both sides of the neck, but none is more than 6 cm across
- N3 means that at least one lymph node containing cancer is larger than 6 cm across
M-stages of Laryngeal Cancer
There are two stages to describe whether cancer of the larynx has spread:
- M0 means there is no cancer spread
- M1 means the cancer has spread to other parts of the body, such as the lungs
Grade of Cancer
The grade of a cancer tells how much the cancer cells look like normal cells under a microscope. There are 3 grades of laryngeal cancer:
- Grade 1 (low grade): the cancer cells look very much like normal larynx cells (they are well-differentiated)
- Grade 2 (intermediate grade): the cancer cells look slightly like normal larynx cells (they are moderately differentiated)
- Grade 3 (high grade): the cancer cells look very abnormal and very little like normal larynx cells (they are poorly differentiated)
ETIOLOGY AND RISK FACTORS
- Age, as with most cancers, cancer of the larynx is more common in older people than in younger. There are few cases in people under 40 years of age
- Drinking alcohol and smoking: smoking tobacco and drinking a lot of alcohol are the main risk factors for cancer of the larynx in the western world
- Alcohol and cigarettes contain chemicals that increase the risk of cancer
- Heavy drinking and smoking are particularly linked to cancer above the vocal cords (the supraglottis) and the area around the vocal cords (the glottis). Compared to non-drinkers, heavy drinkers have about 3 times the risk of developing cancer of the larynx. Even drinking less than two drinks a day (for example, two pints of beer or two small glasses of wine) gives a slightly increased risk of laryngeal cancer. But nonsmokers are unlikely to have an increased risk of laryngeal cancer at this level of drinking
- HPV infection: HPV stands for human papilloma virus (HPV). There are many types of HPV. Some types can affect the lining of the larynx and cause small, wart-like growths.
- Diet: poor eating patterns are common in people who are heavy drinkers. This may be one reason why alcohol increases the risk of cancer. A poor diet may increase risk of cancer of the larynx. This may be due to a lack of vitamins and minerals. A diet high in fresh fruit and vegetables seems to reduce the risk of cancer of the larynx. This may be because these foods contain high levels of the antioxidant vitamins, A, C and E. vitamins and other substances in fresh foods may help to stop damage to the lining of the larynx that can lead to cancer
- Family history: people who have a first degree relative diagnosed with a head and neck cancer have double the risk of laryngeal cancer of someone without the family history
- Low immunity: HIV and AIDS lower immunity and so do drugs that people take after organ transplants
- Exposure to substances: some chemicals may increase risk of cancer of the larynx, like wood dust, soot or coal dust, or paint fumes, exposure to coal as a fuel source at home
- Acid reflux: reflux happens when stomach acid comes back up the esophagus and irritates the lining. In the long term this can cause damage to the cells in the esophagus. This irritation and damage can extend to the larynx and may increase cancer risk
SIGNS AND SYMPTOMS
- A cough
- Changes in voice, such as hoarseness
- Difficulty swallowing
- Ear pain
- A lump or sore that does not heal
- A sore throat
- Weight loss
DIAGNOSTIC EVALUATION
- Flexible endoscopy of the larynx: this test means the back of mouth and throat (including the larynx) examined with a narrow, flexible telescope (a nasoendoscope). This is passed up the nose to look at all upper air passages, including the larynx from above. This may be a bit uncomfortable, but can have an anesthetic spray to numb throat first. This test is sometimes called a nasoendoscopy.
- Endoscopy: an endoscope is a series of connected telescopes that an ENT specialist uses to look at the back of throat. There are camera and light at one end, and an eyepiece at the other. Through the endoscope, doctor can see the inside the nose and throat very clearly and will take biopsies of any abnormally looking areas.
- Transnasal esophagoscopy: the doctor inserts a flexible tube (endoscope) through nose and down the throat. This test is sometimes used instead of having an endoscope under general anesthetic. The tip of the tube has a digital video system and self-contained light. This test is done under a local anesthetic. It gives clear pictures of the inside of the throat and larynx.
- Fine needle aspiration: this is sometimes written as FNA. A fine needle aspiration is done to aspirate the fluid to evaluate any cancerous property
- Physical examination
- CT scan: this is a computerized scan using X-rays to evaluate the size of the cancer and any enlarged lymph nodes in the neck
- MRI scan
- PET-CT scan
MANAGEMENT
The Main Treatments
The main treatments for cancer of the voice box are radiotherapy or surgery
Radiotherapy
Radiotherapy can shrink a large tumor in the larynx and make it easier to remove. Or it can kill off any cancer cells that might have been left behind after surgery. This lowers the risk of the cancer coming back.
Radiotherapy may be used to treat the lymph nodes after surgery; if there is a risk, these may contain cancer cells. This may be instead of lymph node dissection.
Surgery
- Partial laryngectomy (also called cordotomy): tumors that are limited to one vocal cord are removed, and a temporary tracheotomy is performed to maintain the airway. After recovery from surgery, the patient will have a voice but it will be hoarse
- Hemilaryngectomy: when there is a possibility the cancer includes one true and one false vocal cord, they are removed along with an arythenoid cartilage and half of the thyroid cartilage. Temporary tracheotomy is performed, and the patient’s voice will be hoarse after surgery
- Supraglottic laryngectomy: when the tumor is located in the epiglottis or false vocal cords, radical neck dissection is done and tracheotomy performed. The patient’s voice remains intact; however, swallowing is more difficult because the epiglottis has been removed.
- Total laryngectomy: advanced cancers that involve a large portion of the larynx require removal of the entire larynx, the hyoid bone, the cricoid cartilage, two or three tracheal rings, and the strap muscles connected to the larynx. A permanent opening is created in the neck into the trachea, and a laryngectomy tube is inserted to keep the stoma open. The lower portion of the posterior pharynx is removed when the tumor extends beyond the epiglottis, with the remaining portion sutured to the esophagus after a nasogastric tube is inserted. The patient must breathe through a permanent tracheostomy, with normal speech no longer possible.