ENDOCARDITIS – Etiology, Risk
Factors, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and
Management
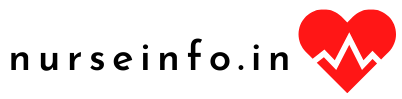
Endocarditis
is an infection of the heart’s valves or its inner lining (endocardium). It is
most common in people who have a damaged, diseased, or artificial heart valve,
caused by bacterial infection.
ETIOLOGY
Endocarditis
is caused by bacteria that enter the bloodstream and settle on the inside of
the heart, usually on the heart valves. Bacteria can invade in the bloodstream
in the many ways, including during some dental and surgical procedures. If one
does not take care of teeth, then chances of endocarditis increase.
Streptococcus viridians is responsible for about 50% of all bacterial
endocarditis cases. This is why dental procedures increase chances for
developing this condition. Other common agents include staphylococcus aureus
and Enterococcus. Staphylococcus aureus can infect normal heart valves and is
the most common cause of infectious endocarditis in intravenous drug users.
RISK FACTORS
Had endocarditis in the past
Hemodialysis for kidney failure
Abnormal or damaged heart valves
An artificial heart valve
A congenital heart defect
Hypertrophic cardiomyopathy
Injected illegal drugs using dirty
needles or without cleaning the skin
HIV
Coronary artery bypass graft surgery
(bypass surgery)
Previous rheumatic fever without
heart valve damage
A pacemaker or an implantable
cardioverter-defibrillator (ICD)
A heart attack without other
complications
Mitral valve prolapse without mitral
valve regurgitation or unusually thickened valve leaflets
A coronary artery stent
PATHOPHYSIOLOGY
Entry of
microorganism in the bloodstream —- colonization occurs on endothelium —-
replication of microbes occur —- platelets and fibrins surround the microbes
—- bacteria stimulate the humoral immune system —- nonspecific antibodies
are produced —- microbes become less vulnerable to antibodies due to
platelets and fibrin coverings
SIGNS AND SYMPTOMS
Chills and fever
Fatigue
Weight loss
Night sweats
Painful joints
Persistent cough and shortness of
breath
Bleeding under the fingernails
Tiny purple and red spots under the
skin
Nail abnormalities (splinter
hemorrhages under the nails)
Night sweats (may be severe)
Paleness
Red, painless skin spots on the palms
and soles (Janeway lesions)
Red, painful nodes (Osler’s nodes) in
the pads of the fingers and toes
DIAGNOSTIC EVALUATION
A physical
examination may reveal:
Enlarged spleen
Splinter hemorrhages in the
fingernails
A history of congenital heart disease
raises the level of suspicion. An eye examination may show bleeding in the
retina a central area of clearing. This is known as Roth’s spots
The
following tests may be performed:
Blood culture and sensitivity (to
detect bacteria)
Chest X-ray
Complete blood count (may show mild
anemia)
CT scan of the chest
Echocardiogram (ultrasound of the
heart)
Erythrocyte sedimentation rate (ESR)
Transesophageal echocardiogram
MANAGEMENT
The American
Heart Association recommends preventive antibiotics for people at risk for
infectious endocarditis before:
Certain dental procedures
Surgeries on respiratory tract or
infected skin, skin structures, or musculoskeletal tissue
Antibiotics
are more likely to be recommended to those with the following risk factors:
Artificial heart valves
Certain congenital heart defects,
both before or possibly after repair
History of infective endocarditis
Valve problems after a heart
transplant
NURSING MANAGEMENT
Nursing
Diagnosis
Hyperthermia related to infection of
cardiac tissue as evidenced by temperature elevation, diaphoresis, chills, malaise,
tachycardia and tachypnea
Intervention
Monitor temperature as appropriate to
determine effectiveness of therapy and to prevent treatment-induced hypothermia
Administer antipyretic medication as
appropriate or as ordered to reduce fever
Administer medications as appropriate
to treat the cause of the fever
Monitor white blood cell count to
evaluate a patient’s response to treatment
Monitor vital signs to assess
cardiorespiratory response to fever
Encourage intake of oral fluids to
replace fluids lost as a result of fever
Activity intolerance related to
generalized weakness, arthralgia, and alternation in oxygen transport secondary
to valvular dysfunction
Intervention
Monitor cardiorespiratory response to
activity (e.g. vital signs) to plan or alter activities
Monitor patient for evidence of
excess physical (e.g. tachycardia, hypertension, diaphoresis, dyspnea) or
emotional fatigue to plan for changes in activity level
Instruct patient/caregiver to
recognize signs and symptoms of fatigue that require reduction in activity
(e.g. pulse increases> 20 beats/min; no increase in activity if resting
pulse > 100 beats/min) since these signs indicate excessive cardiac effort
Encourage alternate rest and activity
periods to reduce cardiac workload
Deficient knowledge related to lack
of experience and exposure to information about disease and treatment process
Review patient’s and caregiver’s knowledge about condition to
identify teaching needs
Discuss common signs and symptoms of
the disease (e.g. fatigue, malaise, chills, elevated temperature, anorexia) so
health care provider can be notified and treatment initiated promptly
Discuss lifestyle changes that may be
required to prevent future complications and/or control the disease process
(e.g. avoiding persons with infection, taking prophylactic antibiotics before
dental procedures) to reduce the risk of recurrent infective endocarditis
Teaching: prescribed medication
Provide the patient and caregiver
with information about the action, purpose and side effects of the medications
to promote safe medication therapy
ENDOCARDITIS – Etiology, Risk Factors, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
NURSING PROCESS – Definition, Steps,
Assessment, Diagnosis, Planning, Implementation and Evaluation
DEFINITION
Nursing
process is an orderly, systematic manner of determining the patient’s problems,
making plans to solve them, initiating the plan or assigning others to
implement it and evaluating the extent to which the plan was effective in
resolving the problems identified.
The five
steps in nursing process are as follows:
Assessment or gathering data
Diagnosis or identifying a problem
Planning or creating a plan to
achieve desired outcomes
Implementation or enacting the plan
Evaluation or determining the effectiveness
of the plan
NURSING ASSESSMENT
Assessment
involves the collection, organization and analysis of information about the
patient’s health. In psychiatric mental health nursing, this process is often
referred to as a psychosocial assessment. The nurse obtains assessment data
from several sources.
Components
of Psychosocial Assessment
Interview with the patient and his
family
History and physical examination
Mental status examination
Records from other healthcare
facilities or prior treatment
Laboratory and psychological tests
Assessments by other professional and
para-professionals
Clinical
Interview
The
interview allows the nurse to hear the patient’s perspective on the problem
Conduct the interview in a quiet
place, ensure privacy
Be relaxed and maintain an unhurried
posture
Maintain eye contact with the patient
Be interested and attentive to what
he says
Pick up verbal and non verbal cues of
distress
Allow the patient to talk freely
without any interruption
When the patient deviates from the
theme or loses his tract, guide him to the main theme politely
Use open-ended questions
Use active listening
Do not offer premature conclusions
and assurance on the outcome of the treatment
History
Taking
History
taking proceeds through different headings as follows:
Identification and demographical
details
Presenting complaints and duration
History of present illness
Past psychiatric history
Family history
Personal history
Premorbid personality
Identification and Demographical Details
This includes the patient’s name, age, sex, religion,
address, socioeconomic status, hospital number, marital status, occupation
details of informant, and information relevant or not, adequate or not.
Presenting Complaints/Chief Complaints
Here symptoms are listed in a chronological order with their
duration. Sometimes the patient may deny the existence of any symptoms and say
that he was forcibly brought to the hospital by his relatives. In such cases,
information is collected from his relatives. It is preferable to use the
patient’s own words verbatim, without translating or interpreting their
meaning. For example, sleeplessness – 3 weeks, loss of appetite and hearing
voices – 2 weeks.
The mode of onset of the illness may be acute or insidious.
The progress may be steady and progressive or diminishing and reappearing
periodically or staying the same way throughout. These should also be enquired
into. Sometimes the patient will be able to point out some antecedent stressful
event alluded as precipitants. The temporal relation of the event with the
illness, severity of the stress, the patient’s preoccupation with the events
and the value attached to the event by him, may all give a clue to the presence
and nature of the precipitant.
History of Present Illness
Under this are recorded the evolution of the patient’s
symptoms from the time they were first noted till the time of consultation.
Details of each symptom should be collected. The patient’s history may have to
be supplemented with data available from other sources.
It is ideal to use the patient’s own words. Look for and also
ask for any precipitating factors. An attempt should also be made to identify
any possible secondary gain to the patient because of his symptoms.
Past Psychiatric History
Enquire whether the patient has any psychiatric illness in
the past. If so its nature, duration, treatment and outcome should be noted
down. If treatment was discontinued in the middle enquire the reason for this
as well as the reason for switching over to other models of therapy.
Family History
Enquire about the type and size of family and the general
family environment. The presence of psychiatric illness on the paternal or
maternal side should be routinely asked. It would be useful to construct a
family tree depicting the living members, their age, deceased members and their
age at death. Mark whether any of them has or had a similar illness and if
known the type of treatment they received and the outcome. Note specifically
any history of suicide, mental retardation, epilepsy or any genetically transmittable
disorders.
Personal History
The personal history includes the developmental, educational,
occupational as well as the sexual history of the patient. Developmental
history includes details of pregnancy and delivery, developmental milestones, health
during childhood and adolescence, neurotic symptoms and occurrence of any
significant event (for example, separation from parents, bereavements, etc are
recorded).
The educational history relates to details regarding the
level of performance in school, relationship with peers and teachers, academic
achievements and extracurricular activities.
In occupational history, enquiry should be made about the
types of work, job satisfaction, whether jobs were changed frequently and if
so, the reasons for this, work skills and relationship with colleagues.
Sexual history includes details about sexual development,
practices and attitudes towards sex. In marital history, enquire about married
life and details about spouse and children.
Premorbid Personality
Personality of a patient consists of those habitual attitudes
and patterns of behavior which characterize an individual. Personality
sometimes changes after the onset of an illness. The nurse has to get a
description of the personality before the onset of the illness and aim to build
up a picture of the individual not a type. Enquiry with respect to the
following areas has to be made.
Attitude to others in social, family
and sexual relationship: Ability to trust others, make and sustain
relationship, anxious or secure, leader or follower, participation,
responsibility, capacity to make decision, dominant or submissive, friendly or
emotionally cold, etc. Difficulty in role taking- gender, sexual and familial.
Attitude to self: Egocentric,
selfish, indulgent, dramatizing, critical, depreciatory, over concerned,
self-conscious, satisfaction or dissatisfaction with work. Attitude towards
health and bodily functions. Attitude to past achievements and failure, and to
the future.
Moral and religious attitudes and
standards: Evidence of rigidity or compliance, permissiveness or over
conscientiousness, conformity, or rebellion. Enquire specifically about
religious beliefs. Excessive religiosity
Mood: Enquire about stability of
mood, mood swings, whether anxious, irritable, worrying or tense. Whether
lively or gloomy. Ability to express and control feelings of anger, anxiety or
depression.
Leisure activities and hobbies:
Interest in reading, playing, music, movies, etc., Enquire about creative
ability. Whether leisure time is spent alone or with friends. Is the circle of
friends large or small?
Fantasy life: Enquire about content
of day dreams and dreams, amount of time spent in day dreaming
Reaction pattern to stress: ability
to tolerate frustrations, losses, disappointments, and circumstances arousing
anger, anxiety or depression. Evidence for the excessive use of particular
defense mechanisms, such as denial, rationalization, projection, etc.,
Mental
Status Examination
The mental
status examination (MSE) is used to determine whether a patient is experiencing
abnormalities in thinking and reasoning ability, feelings or behavior. The MSE
includes observations and questions in the following categories:
General appearance and behavior
Speech
Thought
Mood and affect
Perception
Cognitive functions
General
Appearance and Behavior
Describe
patient’s appearance and behavior. Is he dressed properly? Assess the patient’s
sensorium. Is he alert? Drowsy? Stuporous? Comatose? Is he cooperative for the
examination? Does he make eye contact with the examiner? What is his level of
activity? Is he excited? Retarded? Hyperactive? Restless? Does he have any mannerisms? Gestures? Tics?
Involuntary movements?
Speech
The manner of
speaking and its defects are recorded under speech, whereas the content and
form of speech are recorded under thought disorders. Does he speak
spontaneously or only responding to questions posed to him? Assess the rate,
quantity and flow of speech. It is worthwhile to record a sample of speech for
later analysis.
Thought
Inference
about the thought process and its disorders are made from the speech sample or
the writing sample of the patient. Disorders of form, progression, content and
possession may be present. Does the patient have delusions, obsessive
ruminations and thought alienation? How does the delusion affect his behavior?
Mood and
Affect
The patient
should be asked about his affective state. Compare the subjective report with
what is objectively observed. Is his mood appropriate or not? Congruent or
incongruent? Labile? Is the emotional expression blunt? Is the emotional
expression blunt? Is the affective expression adequate and appropriate?
Perception
Has the
patient any perceptual abnormalities like illusions and hallucinations? If
hallucinating, what is the type of hallucination and what is his reaction?
Cognitive
Function
Is the
patient attentive? Can his attention be easily aroused and sustained? How is
his concentration? To assess cognitive function some simple tests can be
administered. The patient is asked to name the days of the week or names of the
months forwards and backwards. He may be asked to serially subtract 7 or 3 from
100 and tell the numbers.
Is the
patient oriented to time, place and other persons? Orientation to time involves
ability to tell correctly the time of the day, date, week, month, year and
other related data. Orientation to a place includes correct information of his
whereabouts, how he came to be there and other details. Correct identification
of people around him ensures orientation to other persons.
Patient’s
intelligence can be inferred from his conversation and behavior, educational
level vocabulary, ability for abstract thinking and reasoning, general
information, etc., Specific tests are used when a more accurate measurement of intelligence
is needed. The patient’s awareness of his disabilities and readiness for
treatment are reflected in insight. Judgment may be inferred from his plans for
the future.
Physical
Examination
A thorough
physical examination should be carried out in all cases. The physical
examination should include body system review, neurological status and
laboratory tests.
Particular
attention is paid to recent head trauma, episodes of hypertension, and changes
in personality, speech, or ability to handle activities of daily living. Also
note for any movement disorders. Available laboratory data are reviewed for any
abnormalities and documented. Particular attention is paid to any abnormalities
of hepatic or renal function because these systems metabolize or excrete many
psychiatric medications. In addition, abnormal white blood cell and electrolyte
levels should be noted.
Psychological
Tests
Psychological tests are another source of data for the nurse to use in planning care for the patient. Commonly used psychological tests are instruments for assessing symptoms.
NURSING PROCESS – Definition, Steps, Assessment, Diagnosis, Planning, Implementation and Evaluation
Nursing
diagnosis is defined as clinical judgments about individual, family or
community responses to actual and potential health problems. Nursing diagnoses
are used to describe nursing interventions, and to delineate the parameters for
developing outcome criteria.
A nursing
diagnosis statement consists of the problem of patient response and one or more
related factors that influence or contributes to the patient’s problem or
response; signs and symptoms or deficiency characteristics or subjective and
objective assessment data that support the nursing diagnosis.
The basic
level psychiatric nurse identifies nursing problems by using the nomenclature
specified by the North American Nursing Diagnoses Association (NANDA).
A nursing
diagnosis describes an existing or high-risk problem and requires a three-part
statement.
The health problem (Problem, ‘P’)
The etiological or contributing
factors (Etiology, ‘E’)
The defining characteristics (Signs
and symptoms, ‘S’)
For example:
High-risk for self-directed violence
related to depressed mood, feeling of worthlessness, anger turned inward on the
self
Powerlessness related to
dysfunctional grieving process,
lifestyle of helplessness, evidenced by feelings of lack of control over life
situations, over dependence on others to fulfill needs.
Planning
Planning
involves setting and prioritizing goals, formulating nursing interventions and
developing a care plan in conjunction with the patient based on the nursing
diagnoses chosen.
Specific patient needs
Consideration of the patient’s
strengths and weaknesses
Encouragement of the patient to help
set achievable goals and participate in his own care
Feasible interventions
Nursing interventions with rationale are selected in the
planning phase based on the patient’s identified risk-factors and defining
characteristics. The process of planning includes:
Collaboration by the nurse with
patients, significant others, and treatment team members
Identification of priorities of care
Critical decisions regarding the use
of psycho therapeutic principles and practices (identify the most appropriate
nursing intervention)
Coordination and delegation of
responsibilities
In this, the
nurse will choose nursing interventions appropriate to an individual’s
identified problem with specific expected outcomes.
Once the
nursing diagnoses are identified, the next step is the prioritization of the
problems in order of importance. Highest priority is given to those problems
that is life threatening. Next in the priority are those issues that are
related to normative or developmental experiences. Psychiatric nurses often use
Maslow’s hierarchy of needs to prioritize nursing diagnosis.
Outcome
Identification
Outcomes can
be defined as a patient’s response to the care received. Outcomes are the end
result of the process. Measuring outcomes not only demonstrates clinical
effectiveness, but also helps to promote rational clinical decision making on
the part of the nurse. Each outcome must follow certain criteria.
Relate directly to the nursing diagnosis
Be measurable, time limited, and
realistic
Be stated as a desired patient
outcome of nursing care
Reflect the desires of the patient
and his family
Be stated in a way that the patient
and his family can understand
Diagnosis:
Impaired social interaction (isolates self from others)
Outcome:
Patient will attend group sessions everyday
Intervention:
Using a contract format explain the role and responsibility of patients
Correct and
Incorrect Outcome Statements
Nursing
Diagnosis – Anxiety
Correct
Outcome- Verbalizes feeling, calm, relaxed, with absence of muscle tension and
diaphoresis; practices deep breathing
Incorrect
Outcome- Exhibits decreased anxiety, engages in stress reduction
Nursing
Diagnosis- Ineffective Coping
Correct
Outcome- Makes own decisions to attend groups; seeks staff for interaction
In the
implementation phase nurse sets interventions prescribed in the planning phase.
Nursing
interventions (also known as nursing orders or nursing prescriptions) are the
most powerful pieces of the nursing process. Interventions are selected to
achieve patient outcome and to prevent or reduce problems. Implementation
serves as a blueprint of plan.
Nursing
interventions are classified as independent, interdependent and dependent.
Nursing
Intervention in Psychiatric Nursing
Interventions
for biological dimension:
Self-care activities
Activity and exercise
Nutritional interventions
Hydration interventions
Thermoregulation intervention
Pain management
Medication management
Interventions
for Psychological Dimension:
Counseling interventions
Conflict resolutions
Bibliotherapy
Reminiscence therapy
Relaxation interventions
Behavior therapy
Cognitive therapy
Psychoeducation
Spiritual interventions
Interventions
for social dimensions:
Group interventions
Family intervention
Milieu therapy
Evaluation
Evaluation is the process of determining the value of an intervention. Nurses determine the effectiveness of interventions with particular patients. Nurses evaluate selected interventions by judging the patient’s progress towards the outcome set down in the nursing care plan.
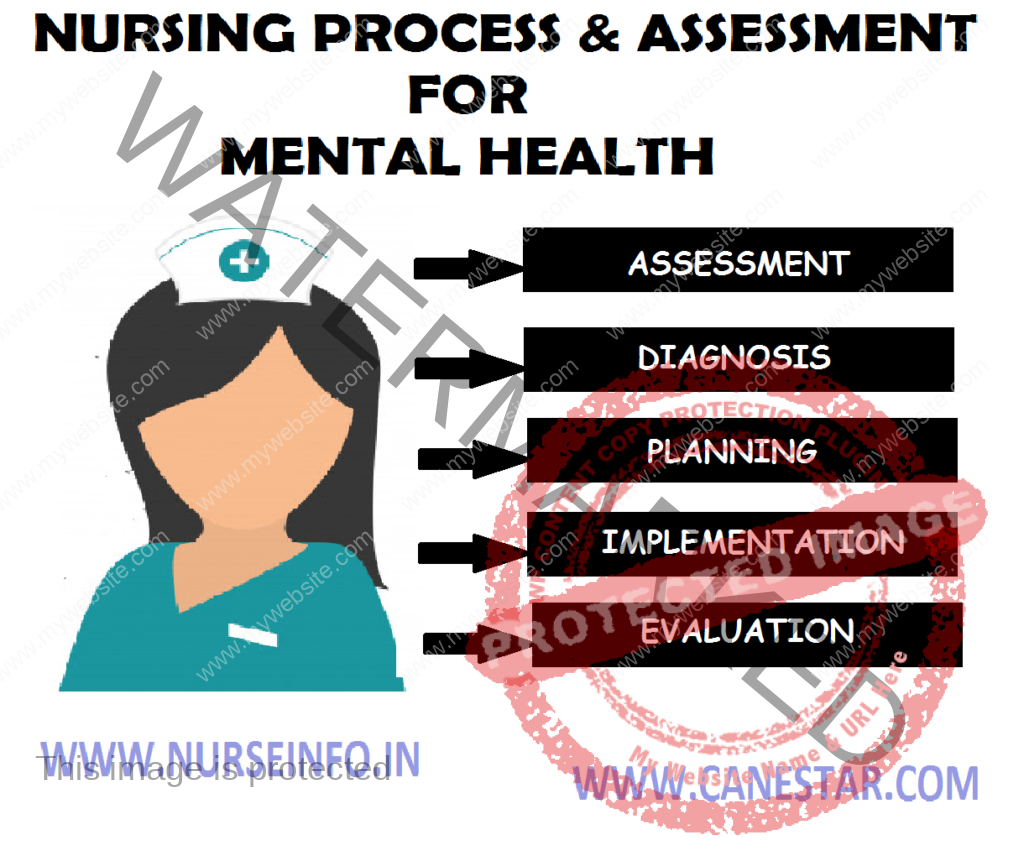
Chronic
pericarditis is a condition in which there is chronic inflammatory thickening
of the pericardium that changes the pericardium into thick fibrous band of
tissues. Thus, the tissues encircle, encase and compress the heart and prevent
it from expanding to normal size, causing restriction of ventricular filling.
TYPES
Adhesive pericarditis
Adhesive mediastinopericariditis
Constrictive pericarditis
Adhesive pericarditis: chronic
pericarditis with adhesions between visceral and parietal pericardium
CAUSES
Shortness of breath
Pain: it may be steady and constant
or it may occur in paroxysms, usually after unusual effort or after mental
excitement or a fit of anger
Pulse: rapid and feasible; pulse
tension and pressure greatly reduced; irregular pulse
Palpitations
Ventricles become dilated and
hypertrophied with its concomitant symptoms – dropsy, vertigo and venous stasis
are present
Treatment: it needs most careful and
continuous oversight. Effusion should be retarded and its absorption and removal
should be promoted by rational measures
Adhesive mediastino pericarditis:
here pericardial sac is obliterated due to adhesion between two layers of
pericardium as well as between parietal pericardium and surrounding mediastinal
structures, chest wall and diaphragm
Constrictive pericarditis:
constrictive pericarditis is a late sequela of an inflammatory condition of the
pericardium. The inflammatory condition is usually an infection that involves
the pericardium, but it may also occur after a heart attack or after heart
surgery
Almost half
the cases of constrictive pericarditis in the developing world are idiopathic
in origin. In regions where tuberculosis is common, it is the cause in a large
portion of cases. Causes of constrictive pericarditis include:
Infectious (tuberculosis, incomplete
drainage of purulent pericarditis, fungal and parasitic infections)
Inflammatory and autoimmune: (chronic
pericarditis, postviral pericarditis, postsurgical, following pericarditis
associated with acute myocardial infarction, following postmyocardial
infarction (Dressler’s) syndrome, in association with pulmonary asbestosis
Prior mediastinal radiation therapy
Chronic renal failure
Connective tissue disorders
Neoplastic pericardial infiltration
PATHOPHYSIOLOGY
Constrictive
pericarditis is due to a thickened, fibrotic pericardium that forms a
noncompliant shell around the heart —- this shell prevents the heart from
expanding when blood enters it —-
During inspiration, the negative
pressure in the thoracic cavity will cause increased blood flow into the right
ventricle —- increased volume in the right ventricle will cause the
interventricular septum to bulge towards the left ventricle, leading to
decreased filling of the left ventricle —- due to the Frank-Starling law,
this will cause decreased pressure generated by the left ventricle during
systole —- thi is known as ventricular interdependence since the amount of
blood flow into one ventricle is dependent on the amount of blood flow into the
other ventricle
During expiration, the amount of
blood entering the right ventricle will decrease —- allowing the
interventicular septum to bulge towards the right ventricle, and increased
filling of the left ventricle and subsequent increased pressure generated by
the left ventricle during systole —- this is known as ventricular
interdependence since the amount of blood flow into one ventricle is dependent
on the amount of blood flow into the other ventricle
DIAGNOSTIC EVALUATION
Imaging will demonstrate a thickened
pericardium. In contrast with restrictive cardiomyopathy, there is an increased
resistance to ventricular filling due to increased myocardial stiffness. Imaging
features of restrictive cardiomyopathy demonstrate an increased left
ventricular thickness with infiltration of the myocardium
Chest X-ray: pericardial
calcification, and pleural effusions are common findings
Echocardiography: the echographic
finding is an exaggerated anterior motion of the septum with the atrial
filling. Since the posterior ventricular wall is unable to expand, an increase
in left ventricular volume with the atrial systole produces a marked
displacement of the septum
CT and MRI: useful in select cases
BNP blood test: tests for the
existence of the cardiac hormone, brain natriuretic peptide which is only
present in RCMP but not in CP, and is particularly helpful in determining the
specific CHF type
Pulmonary catheterization showed all
four heart chambers having equal diastolic pressures
Hepatomegaly and other signs of right
heart failure; ascites; fatigue; peripheral edema
TREATMENT
Pericardial
stripping: the definitive treatment for constrictive pericarditis is
pericardial stripping, which is a surgical procedure where the entire
pericardium is peeled away from the heart. This procedure has significant risk
involved, with mortality rates of 6%. The high risk of the procedure is
attributed to adherence of the thickened pericardium to the myocardium and
coronary arteries. In patients who have undergone coronary artery bypass
surgery with pericardial stripping, there is danger of tearing a bypass graft
while removing the pericardium. Due to the significant risks involved with
pericardial stripping, many patients are treated medically, with judicious use
of diuretics
Common
Causes of Chronic Pericarditis
Long-standing pyogenic infections
Postviral infections
Tuberculosis
Hemopericardium
Common Signs
and Symptoms of Chronic Pericarditis
Congestive heart failure
Dyspnea
Chronic atrial fibrillation
Fatigue on exertion
Leg edema
Ascites
Low pulse pressure
Distended neck pain
Delay in capillary refill time
Common
Treatment of Chronic Pericarditis
Medical Treatment: digitalis and
diuretics
Surgical Treatment: surgical removal
of the tough encasing pericardium (pericardiectomy) is the only treatment of
benefit. The objective of the operation is to release both ventricles from the
constrictive and restrictive inflammation. Surgery may be considered if the
pericardium is scarred and inflexible, or if pericarditis keeps recurring.
The procedure begins when the surgeon
makes and incision in the skin over the breastbone and divides it to expose the
pericardium. During the surgery, the surgeon will grasp the pericardium, cut
the drop of this fibrous covering of the heart, drop it into the specimen bag,
and re-cover the heart. The breastbone is then wired back together and the
incision is closed, completing the procedure. When the portion of pericardium
lying between the two phrenic nerves is excised, it is called total
pericardiectomy. In cases where total pericardiectomy is not possible, subtotal
pericardiectomy is performed or, in extreme cases, a cruciate incision on the
pericardium is performed.
Nursing Management
Assessment
Assess signs of pain
Assess association of pain with
respiratory movements, cough, swallowing
Assess for pericardial friction rub
(helps to distinguish between pericarditis and MI).
Frequently check client for
temperature (pericarditis can cause abrupt onset of fever in a previously
afebrile patient).
Nursing
Diagnosis
Acute pain related to inflammation of layers
of heart
Goal: to
relieve pain
Interventions
Check the intensity of pain
Assist the patient to sit upright or
to lean forward to relieve pain
Restrict the activities of patient
Provide prescribed analgesics
(morphine).
Hyperthermia related to inflammatory
process
Goal: to
maintain normal temperature
Interventions
Monitor temperature 2-4 hourly
Observe for basic principles of
asepsis like handwashing
Provide cold compression if chills
are not present along with fever
Administer prescribed antibiotics and
antipyretics (decreased cardiac output
related to structural abnormality of valves
Goal: to
reduce risk of complications
Interventions
Monitor BP and pulse (pulsus
alternans indicates left-sided heart failure)
Evaluate jugular vein distension
Check laboratory findings (ECG,
cardiac enzymes)
Maintain intake
Output chart
Obtain daily weight
Administer prescribed drugs like
digitalis (risk for complications related to disease process)
Goal: to
reduce risk of complications
Interventions
Assess vital signs of patient
Assess peripheral edema
Check the laboratory findings (ECG,
cardiac enzymes)
Administer digitalis and digoxin if
signs of heart failure appear
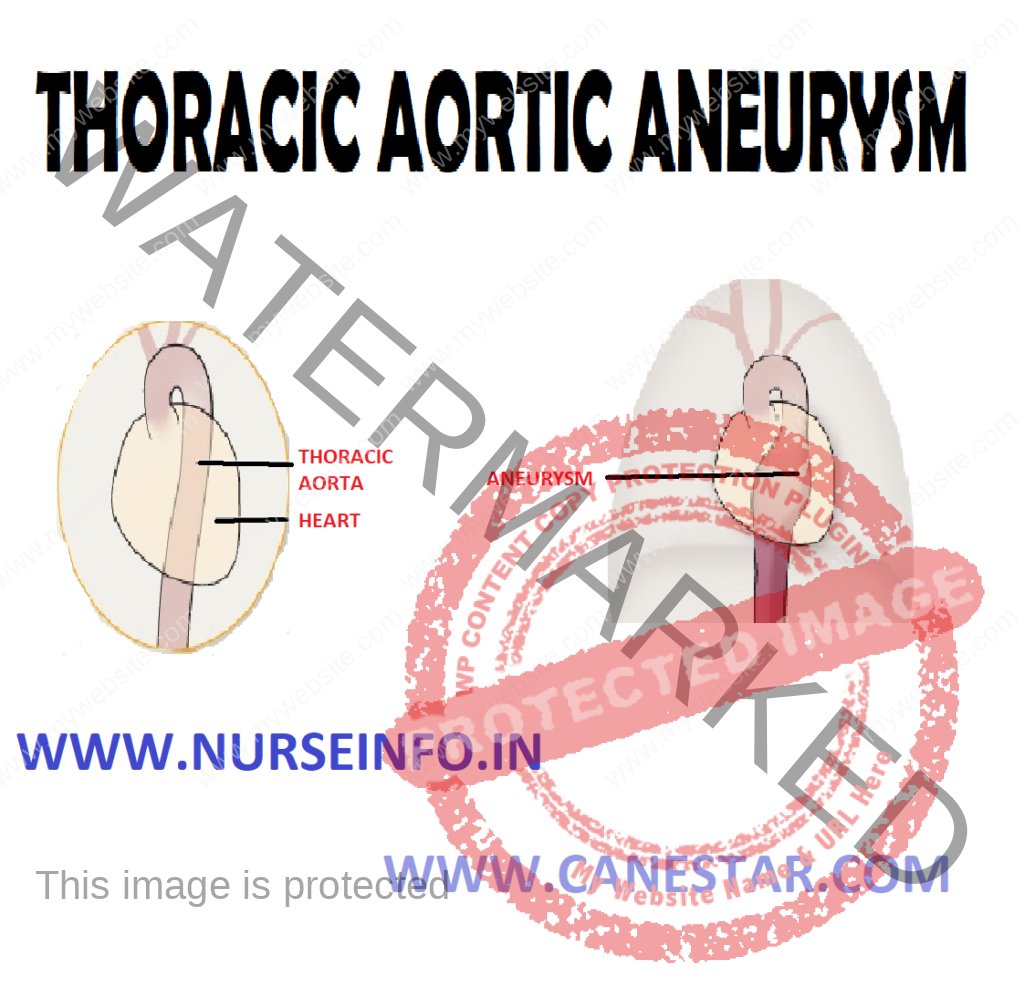
THORACIC AORTIC ANEURYSM –
Introduction, Clinical Manifestations, Signs and Symptoms, Diagnostic
Evaluation and Management
INTRODUCTION
Approximately
85% of all cases of thoracic aortic aneurysm are called by atherosclerosis.
They occur most frequently in men between ages 40 and 70 years. The thoracic
area is the most common site for a dissecting aneurysm. About one-third of
patients with thoracic aortic aneurysm die of rupture of aneurysm
CLINICAL MANIFESTATIONS
Symptoms are
variable and depend on how rapidly the aneurysm dilates and how the pulsating
mass affects the surrounding intrathoracic structures. Some of the patients are
asymptomatic. But some are having:
Pain occurring in supine position
Dyspnea
Hoarseness
Stridor
Weakness
Aphonia
Dysphasia
ASSESSMENT AND DIAGNOSTIC TESTS
Physical Examination: superficial
veins of neck, chest or arm dilated
Chest X-ray
Transesophageal echocardiography
TREATMENT (Medical Management)
Antihypertensive: hydralazine
hydrochloride
Beta blocker: atenolol, timolol
maleate
Surgical
Management
Repair of an
ascending aortic wall aneurysm and aortic wall replacement —- incision into
aortic aneurysm —- aortic wall replacement with aortic graft implant to
repair ascending aortic aneurysm —- aortic aneurysm trimmed —- then closed
over graft
Abdominal Aortic Aneurysm
Introduction
The most
common cause of abdominal aortic aneurysm is arteriosclerosis. The condition
which is more common among Caucasians population affects men 4 times more often
than women and it is most prevalent in elderly patients. Most of this aneurysm
occurs below renal arteries. Untreated, the eventual outcome may be rupture and
death.
CAUSES
Congenital weakness
Smoking
Hypertension (50% cases)
CLINICAL MANIFESTATIONS
Patient feels his heart beating in
abdomen
Abdominal mass
Abdominal throbbing
ASSESSMENT AND DIAGNOSTIC TESTS
Physical Examination: superficial
veins of neck, chest or arm dilated
Duplex ultrasonography
CT scan: determine size, length and
location of aneurysm
TREATMENT (Medical Management)
Medical therapy of aortic aneurysms
involves strict blood pressure control. This does not treat the aortic aneurysm
per se, but control of hypertension within tight blood pressure parameters may
decrease the rate of expansion of the aneurysm
The tetracycline and doxycycline is
currently being investigated for use as a potential drug in the prevention of
aortic aneurysm due to its metalloproteinase inhibitor and collagen-stabilizing
properties
PREVENTION
Attention to
patient’s general blood pressure, smoking and cholesterol risks helps reduce
the risk on an individual basis. There have been proposals to introduce
ultrasound scans as a screening tool for those most at risk: men over the age
of 65
Surgical Management
For
abdominal aortic aneurysms, suggest elective surgical repair when the diameter
of the aneurysm is greater than 5 cm (2 in). However, suggest medical
management for abdominal aneurysms with a diameter of less than 5.5. (2 in).
Open Surgery
Open surgery
typically involves dissection of the dilated portion of the aorta and insertion
of a synthetic (Dacron or Gore-Tex) patch tube. Once the tube is sewn into the
proximal and distal portions of the aorta, the aneurysmal sac is closed around
the artificial tube. Instead of sewing, the tube ends, made rigid and
expandable by nitinol wireframe, can be much more simply, quickly and
effectively inserted into the vascular stumps and there permanently fixed by
external ligature
Endovascular
Surgery
The endovascular treatment of aortic aneurysms involves the placement of an endovascular stent via a percutaneous technique (usually through the femoral arteries) into the diseases portion of the aorta. This technique has been reported to have a lower mortality rate compared to open surgical repair, and is now being widely used in individuals with comorbid conditions that make them high-risk patients for open surgery
THORACIC AORTIC ANEURYSM – Introduction, Clinical Manifestations, Signs and Symptoms, Diagnostic Evaluation and Management
Occasionally,
in aorta diseases by atherosclerosis, a tear develops in the intima or the
media degenerate, resulting in a dissection.
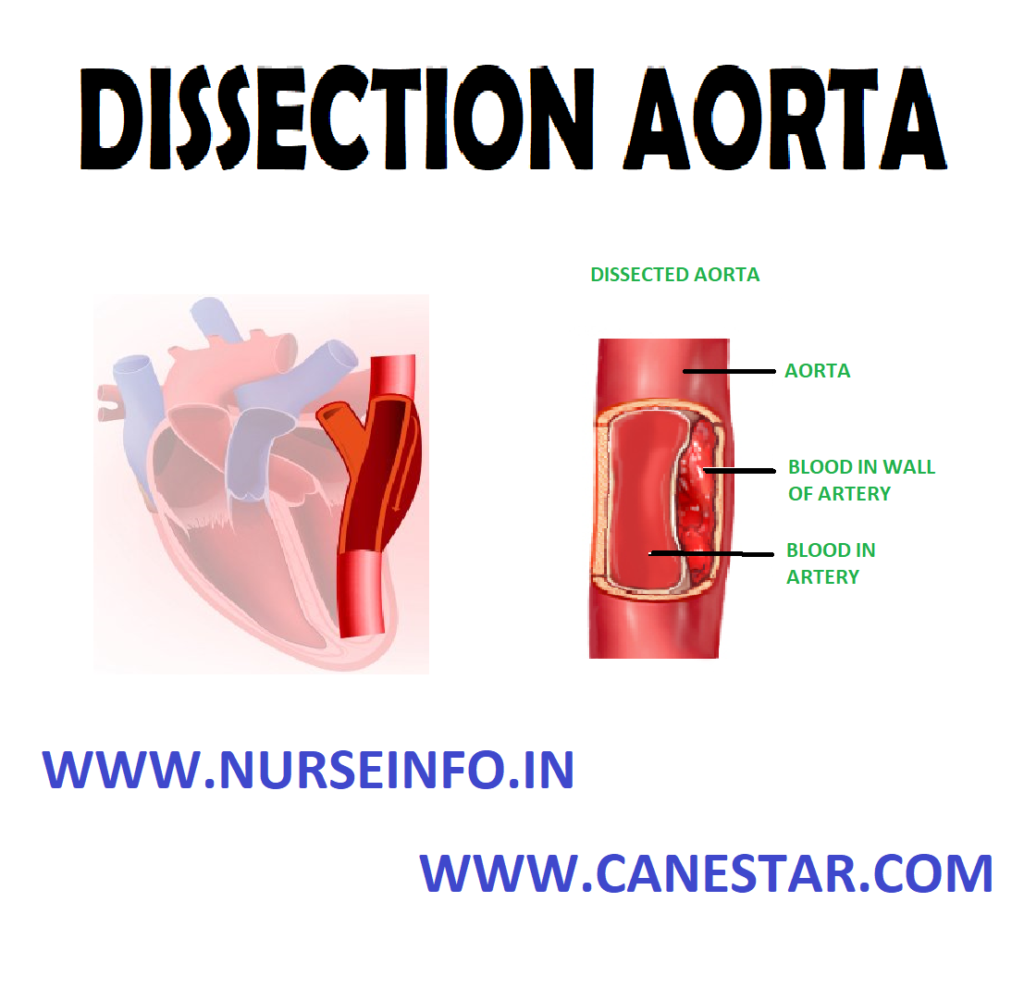
DEFINITION
An aortic
dissection is a serious condition in which a tear develops in the inner layer
of the aorta, the large blood vessel branching off the heart. Blood surges
through this tear into the middle layer of the aorta, causing the inner and
middle layers to separate (dissect). If the blood-filled channel ruptures
through the outside aortic wall, aortic dissection is often fatal.
INCIDENCE
Arterial
dissection is commonly associated with poorly controlled hypertension. It is 3
times more common in men than in women and occurs most commonly in 50 to 70
year old age group. Dissection is caused by rupture in the intima layer. A
rupture may occur through adventitia or into the lumen through intima, allowing
blood to re-enter the main channel and resulting in chronic dissection or
occlusion of branches of the aorta.
CLASSIFICATION
Stanford
Classification
The Stanford
classification divides dissections into 2 types, type A and type B. Type A
involves the ascending aorta (DeBakey types I and II); type B does not involve
(DeBakey type III)
Type A dissections involve the
ascending aorta and arch
Type B involves the descending aorta
A patient can have a type A
dissection, type B dissection, or a combination of both
DeBakey
Classification
The DeBakey
system, named after surgeon and aortic dissection sufferer Michael E. DeBakey,
is an anatomical description of the aortic dissection. It categorizes the
dissection based on where the original intimal tear is located and the extent
of the dissection (localized to either the ascending aorta or descending aorta,
or involves both the ascending and descending aorta. The DeBakey classification
divides dissections into 3 types as follows:
Type I: originates in ascending
aorta, propagates at least to the aortic arch and often beyond it distally. It
is most often seen in patients less than 65 years of age and is the most lethal
form of the disease.
Type II: originates in and is
confined to the ascending aorta
Type III: originates in descending
aorta, rarely extends proximally but will extend distally. It most often occurs
in elderly patients with atherosclerosis and hypertension
ETIOLOGY
High blood pressure: most cases (over
70%) are associated with high blood pressure (hypertension)
Bicuspid aortic valve (a congenital
abnormality of the aortic valve)
Marfan’s syndrome
Ehlers-Danlos syndrome
Turner syndrome
Syphilis
Cocaine use
Pregnancy: pregnancy is a rare
associated risk factor, especially in the third trimester and early in the
postpartum period
Trauma: blunt trauma is known to
cause dissection, which is often seen after car wrecks in which the patient’s
chest hits the steering wheel
Surgical complications: operations
including coronary artery bypass grafting and aortic and mitral valve repairs.
It can also be a complication of heart catheterization
RISK FACTORS
The exact
cause is unknown, but more common risks include:
Aging
Atherosclerosis
Blunt trauma to the chest, such as
hitting the steering wheel of a car during an accident
High blood pressure
PATHOPHYSIOLOGY
As the
separation progresses —- the arteries branching from the involved area of the
aorta shear and occlude —- the tear most commonly occurs in the region of
aortic arch —- the dissection of the aorta may progress in backward direction
of the heart —- obstructing the opening of coronary arteries —- producing
hemopericardium, aortic insufficiency —- it may extend in opposite direction
—- occlusion of arteries supplying GI tract, kidneys, spinal cord or legs
CLINICAL MANIFESTATIONS
Onset of symptoms is sudden
Severe and persistent pain – anterior
chest or back extend to shoulder, epigastric region and abdomen
Sweating
Tachycardia
Appear pale
Increased blood pressure
The symptoms
usually begin suddenly, and include severe chest pain. The pain may feel like a
heart attack, and can:
Be described as sharp, stabbing,
tearing, or ripping
Be felt below the chest bone, then
move under the shoulder blades or to the back
Move to the shoulder, neck, arm, jaw,
abdomen, or hips
Change position – pain typically
moves to the arms and legs as the aortic dissection gets worse
The symptoms
are caused by a decrease of blood flowing to the rest of the body, and can
include:
Anxiety and a feeling of doom
Fainting or dizziness
Heavy sweating (clammy skin)
Nausea and vomiting
Shortness of breath – trouble
breathing when lying flat (orthopnea)
Other
symptoms may include:
Pain in the abdomen
Stroke symptoms
Swallowing difficulties from pressure
on the esophagus
ASSESSMENT AND DIAGNOSTIC TESTS
Physical examination: superficial
veins of neck, chest or arm dilated
D-dimer: a blood D-dimer level less
than 500 ng/ml may be able to rule out the diagnosis of aortic dissection
alleviating the need for further imaging
Chest X-ray: widening of the
mediastinum on an X-ray of the chest has moderate sensitivity in the setting of
an ascending aortic dissection. Pleural effusions may be seen on chest X-ray.
They are more commonly seen in descending aortic dissections. Depression of the
left main stem bronchus and tracheal deviation
Computed
Tomography
Computed
tomography angiography is a fast noninvasive test that will give an accurate
three-dimensional view of the aorta. These images are produced by taking rapid
thin-cut slices of the chest and abdomen, and combining them in the computer to
create cross-sectional slices. In order to delineate the aorta to the accuracy
necessary to make the proper diagnosis, an iodinated contrast material is
injected into a peripheral vein. Contrast is injected and the scan performed
using a bolus tracking method. This is a type of scan timed to an injection to
capture the contrast as it enters the aorta. The scan will then follow the
contrast as it flows through the vessel
It has a
sensitivity of 96 to 100% and a specificity of 96 to 100%. Disadvantages
include the need for iodinated contrast material and the inability to diagnose
the site of the intimal tear.
Magnetic
Resonance Imaging
Magnetic
Resonance Imaging (MRI) is currently the gold standard test for the detection
and assessment of aortic dissection, with a sensitivity of 98% and a
specificity of 98%. An MRI examination of the aorta will produce a
three-dimensional reconstruction of the aorta, allowing the physician to
determine the location of the intimal tear, the involvement of branch vessels,
and locate any secondary tears. It is a noninvasive test, does not require the
use of iodinated contrast material, and can detect and quantitate the degree of
aortic insufficiency.
The
disadvantage of the MRI scan in the face of aortic dissection is that it has
limited availability and is often located only in the larger hospitals, and the
scan is relatively time-consuming. Due to the high-intensity magnetic fields
used during MRI, an MRI scan is contraindicated in individuals with metallic
implants. In addition, many individuals experience claustrophobia while in the
MRI scanning tube
Transesophageal
Echocardiography
It is an
echocardiogram displaying the true lumen and false lumen of an aortic
dissection. In the image to the left, the intimal flap can be seen separating
the two lumens. In the image to the right, color flow during ventricular
systole suggests that the upper lumen is the true lumen.
The
transesophageal echocardiogram (TEE) is a relatively good test in the diagnosis
of aortic dissection, with a sensitivity of up to 98% and a specificity of up
to 97%. It has become the preferred imaging modality for suspected aortic
dissection. It is a relatively noninvasive test, requiring the individual to
swallow the echocardiography probe. It is especially good in the evaluation of
AI in the setting of ascending aortic dissection, and to determine whether the
ostia (origins) of the coronary arteries are involved. While many institutions
give sedation during transesophageal echocardiography for added patient
comfort, it can be performed in cooperative individuals without the use of
sedation. Disadvantages of the TEE include the inability to visualize the
distal ascending aorta (the beginning of the aorta arch), and the descending
abdominal aorta that lies below the stomach. A TEE may be technically difficult
to perform in individuals with esophageal strictures or varices
Aortogram
An aortogram
involves placement of a catheter in the aorta and injection of contrast
material while taking X-rays of the aorta. The procedure is known as
aortography. Previously thought to be the diagnostic ‘gold standard’, it has
been supplanted by other less-invasive imaging modalities
MEDICAL MANAGEMENT
Antibiotic: the antibiotic doxycycline
is currently being investigated for use as a potential drug in the prevention
of aortic aneurysm due to its metalloproteinase inhibitor and collagen
stabilizing properties
Antihypertensive: hydralazine
hydrochloride
Beta blocker: atenolol, timolol
maleate
Vasodilators: sodium nitroprusside
Calcium channel blockers: verapamil
and diltiazem
SURGICAL MANAGEMENT
Replacement
of the damaged section with a tube graft (often made of Dacron) when there is
no damage to the aortic valve
Bentall procedure: replacement of the
damaged section of aorta and replacement of the aortic valve
David procedure: replacement of the
damaged section of aorta and reimplantation of the aortic valve
Tevar: insertion of a stent graft
(covered stent): e.g. in TEVAR (thoracic endovascular aortic repair). It is
usually combined with ongoing medical management
Vascular ring connector (VRC):
replacement of the damaged section of aorta with a sutureless vascular ring
connector-reinforced Dacron graft. Vascular ring connector (VRC) is a titanic
ring used as a stent in the vascular graft to achieve a quick, blood-sealed and
sutureless anastomosis. There are two furrows on the surface of the ring for
fixation of the vascular graft and the aorta. The tapes used to tie against the
ring provide a larger contact surface area than the traditional stitches, thus
providing stronger anastomosis and better surgical results.
Aneurysm is a localized sac or
dilation formed at a weak point in the wall of the aorta.
An aneurysm is an abnormal bulge in
the wall of a blood vessel. A larger bulge, more than 1.5 times the size of
normal aorta, is called an aneurysm
INCIDENCE
30-60/100
Increasing incidence over past 3
decades
Carotid Artery Stenosis – 10%
Smoker: Nonsmoker – 8:1
Male: Female – 4:1
HTN: 40% of pts
Shapes:
Aneurysm may be classified by its shape and form:
True aneurysms: one, two and all
three layers of artery may be involved. It is classified into different types:
Fusiform aneurysms: symmetric, spindle-shaped
expansion of entire circumference of involved vessel. It appears as symmetrical
bulges around the circumference of the aorta. They are the most common shape of
aneurysm
Saccular
aneurysms: a bulbous protrusion, asymmetrical and appear on one side of the
aorta. They are usually caused by trauma or a severe aortic ulcer
Dissecting
aneurysms: a bilateral out pouching in which layers of the vessels wall
separate creating a cavity. This is usually is a haematoma that split the layer
of arterial wall
False aneurysms: the wall rupture and
a blood clot is retained in an out pouching of tissue or there connection
between and artery that does not close.
TYPES
The two
types of aortic aneurysms are:
Thoracic aortic aneurysms: develop in
the part of the aorta that runs through the chest. This includes the ascending
aorta (the short stem of the cane); the aortic arch (the cane handle); and the
descending thoracic aorta (the longer stem of the cane).
Abdominal aortic aneurysms: develop
in the part of the aorta that runs through the abdomen. Most abdominal aortic
aneurysms develop below the renal arteries (the area where the aorta branches
out to the kidneys). Sometimes aortic aneurysms extend beyond the aorta into
the iliac arteries (the blood vessels that go to the pelvis and legs).
Causes: the
exact cause is unknown. But recent evidence includes:
The physical
change in the aortic diameter (can occur) —- secondary to trauma, infection
—- an intrinsic defect in the protein construction of the aortic wall (due
to) —- progressive destruction of aortic proteins by enzymes —- enlargement
of atrial walls
CLINICAL
MANIFESTATIONS
Asymptomatic: 70-75%
Symptoms
Early satiety, N, V
Abdominal, flank, or back pain
1/3 of patients experience abdominal and flank pain
Abrupt onset of pain – rupture or
expansion of aneurysm
DIAGNOSTIC EVALUATION
Physical
Examination
If
>5 cm in diameter, then cannot be detected by routine physical
examination
Radiographs
Calcified wall. Can determine size in
2/3
Cannot rule out and AAA
Arteriography
Cannot determine aneurysm size
because of mural thrombus
Indications for obtaining
arteriography
Suspicion of visceral ischemia
Occlusive disease of iliac and femoral arteries
Severe HTN, or impair renal function
Horseshoe kidney
Suprarenal of TAAA component
Femoropopliteal aneurysms
Ultrasound
Establishes diagnosis easily
Accurately measures infrarenal
diameter
Difficult to visualize thoracic or
suprarenal aneurysms
Difficult to establish relationship
to renal arteries
RESTRICTIVE LUNG DISEASES – Etiology,
Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
Introduction
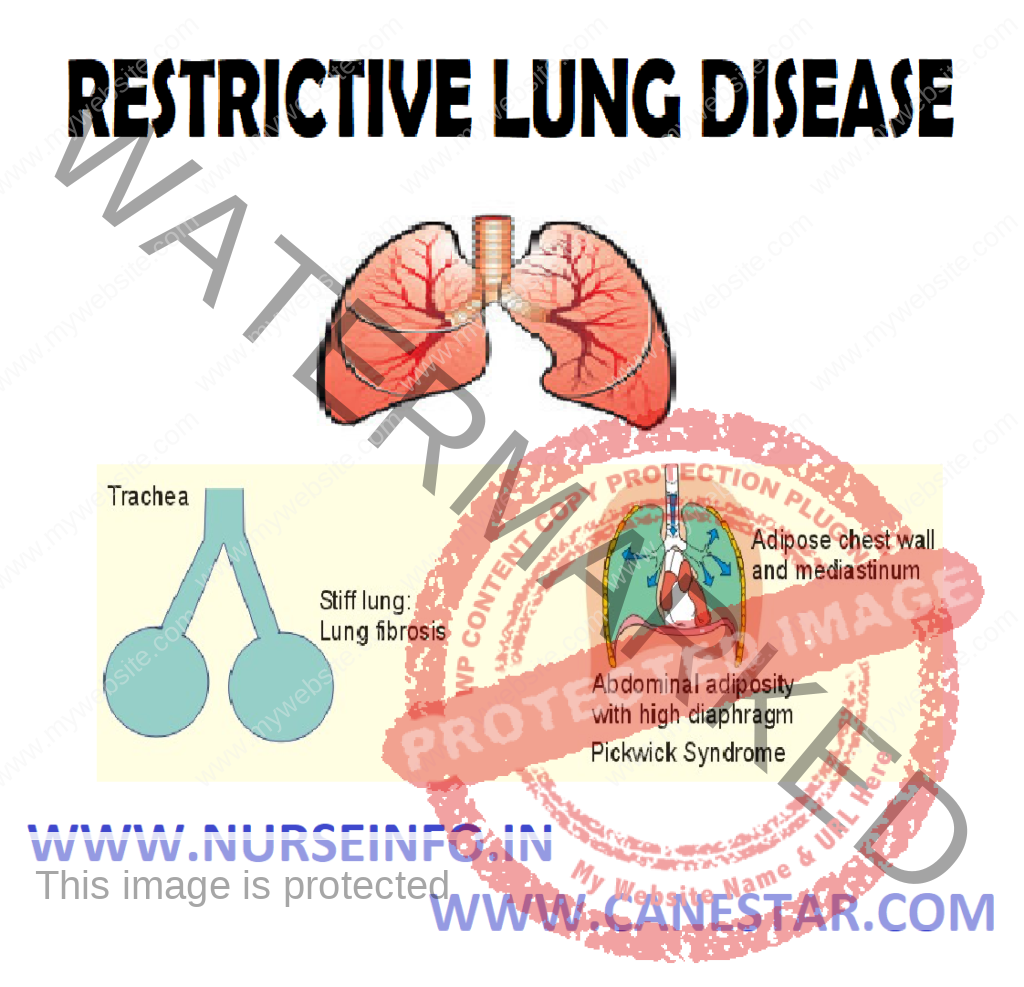
Restrictive
lung diseases are characterized by reduced lung volume, either because of an
alternation in lung parenchyma or because of a disease of the pleura, chest
wall, or neuromuscular apparatus. In physiological terms, restrictive lung
diseases are characterized by reduced total lung capacity (TLC), vital
capacity, or resting lung volume. Accompanying characteristics are preserved
airflow and normal airway resistance, which are measured as the functional
residual capacity (FRC). If caused by parenchymal lung disease, restrictive
lung disorders are accompanied by reduced gas transfer, which may be marked
clinically by desaturation after exercise.
DEFINITION
Restrictive lung disease is a chronic
disorder that causes a decrease in the ability to expand the lung and sometimes
makes it harder to get enough oxygen to meet the body’s needs. The most common
restrictive lung diseases are:
Interstitial pulmonary fibrosis or interstitial lung disease (including
sarcoidosis-granulomatous disorder)
Restrictive lung diseases are
characterized by reduced lung volume, either because of an alteration in lung
parenchyma or because of a disease of the pleura, chest wall, or neuromuscular
apparatus. In physiological terms, restrictive lung diseases are characterized
by reduced total lung capacity (TLC), vital capacity, or resting lung volume
ETIOLOGY
Restrictive
lung diseases may be due to specific causes which can be intrinsic to the
parenchyma of the lung, or extrinsic to it
Intrinsic
Radiation fibrosis, usually from the
radiation given for cancer treatment
Certain drugs such as bleomycin and
methotrexate
As a consequence of another disease
such as rheumatoid arthritis
Hypersensitivity pneumonitis due to
an allergic reaction to inhaled particles
Acute respiratory distress syndrome
(ARDS), a severe lung condition occurring in response to a critical illness or
injury
Infant respiratory distress syndrome
due to a deficiency of surfactant in the lungs of a baby born prematurely
Extrinsic
Neuromuscular diseases, including
Myasthenia gravis, and Guillain-Barre syndrome
Nonmuscular diseases of the upper
thorax, such as kyphosis and chest wall deformities
Diseases restricting lower
thoracic/abdominal volume (e.g. obesity, diaphragmatic hernia, or the presence
of ascites)
Pleural thickening
PATHOPHYSIOLOGY
In cases of
Intrinsic Lung Disease
The
physiological effects of diffuse parenchyma disorders —- reduce all lung
volumes by the excessive elastic recoil of the lungs, in comparison to the
outward recoil forces of the chest wall —- expiratory airflow is reduced in
proportion to lung volume —- arterial hypoxemia in these disorders is
primarily caused by ventilation-perfusion mismatch —- the diffusion of oxygen
is impaired —- hypoxemia
In cases of
Extrinsic Disorders
Disorders of
the pleura and thoracic cage —- the total compliance by the respiratory
system is reduced —- lung volumes are reduced as a result of atelectasis —-
ventilation-perfusion mismatch and hypoxemia —- hypoxemia
SIGNS AND SYMPTOMS
Symptoms of
restrictive lung disease include:
Cough
Shortness of breath
Wheezing and chest pain
Difficulty in inhaling and exhaling
Wheezing and noisy breathing
Coughing up blood
DIAGNOSTIC EVALUATION
Diagnostic
testing for lung disease may include any of the following:
Physical examination
In patients
with intrinsic lung disorders may yield distinguishing physical findings. Those
with chest wall disorders show obvious massive obesity and an abnormal
configuration of the thoracic cage (e.g. kyphoscoliosis, spondylitis)
Cyanosis at
rest is uncommon in persons with interstitial lung diseases, and this is
usually a late manifestation of advanced disease
Digital
clubbing is common in those with idiopathic pulmonary fibrosis
Pulmonary function tests: spirometry
provides an objective assessment of airflow obstruction and is important in
staging asthma severity. It should be done on initial diagnosis of asthma,
after treatment is started and symptoms have stabilized, and every 1 to 2 years
afterward. Spirometry is used to measure the rate of airflow during maximal
expiratory effort after maximal inhalation. It can be useful in differentiating
between obstructive and restrictive lung disorders
Chest X-ray: patient is made to stand
in front of X-ray machine. Patient will be told to hold breath when the X-ray
is taken. Two images are usually taken. You will need to stand against the
machine, and then sideways. Air-space opacities suggest pulmonary hemorrhage
CT scans: high-resolution CT scanning
of the chest can be helpful, but the expense and high dose of radiation makes
it inappropriate for every patient. Generally, complete scans only a few
minutes. The newest multidetector scanners can image the entire body in less
than 30 seconds
Bronchoscopy: a bronchoscope is a
device used to see the inside of the airways and lungs. The scope can be
flexible or rigid. A flexible scope is almost always used. It is a tube less
than one-half inch wide and about two feet long. In rare cases, a rigid
bronchoscope is used. The scope is passed through mouth or nose through
windpipe and into lungs. Going through the nose is a good way to look at the
upper airways
Pulse oximetry: pulse oximeters are
noninvasive devices used to measure a patient’s blood-oxygen saturation level
and pulse rate
Lung biopsy: a lung biopsy is not
always required to make a diagnosis in patients suggested to have interstitial
lung diseases. A lung biopsy can provide information that may help lead to a
specific diagnosis, help assess for disease activity, exclude neoplastic and
infectious processes, establish a definitive diagnosis, and predict the
prognosis
MANAGEMENT
Few
medicines are available to treat most causes of restrictive lung disease. In
cases of restrictive lung disease caused by ongoing inflammation, medicines
that suppress the immune system may be used, including:
Corticosteroids
(such as prednisone)
Corticosteroids
are a first-line therapy but are associated with myriad adverse effects.
Corticosteroids, the most commonly used drugs, halt or slow the progression of
pulmonary parenchymal fibrosis with variable success. The optimal duration of
therapy is not known, but treatment for 1-2 years is suggested
Cytotoxic
Therapy
Immunosuppressive
cytotoxic agents may be considered for patients who do not respond to steroids,
experience adverse effects, or have contraindications to high-dose
corticosteroid therapy. The failure of steroid therapy is defined as a fall in
FVC or TLC by 10% a worsened radiographic appearance and a decreased gas
exchange at rest or with exercise
Azathioprine is less toxic than
methotrexate or cyclophosphamide and may be preferred as a
corticosteroid-sparing agent for disorders that are not life-threatening. A
response to therapy may not occur for 3-6 months
Because of potentially serious
toxicities, cyclophosphamide is reserved for fulminant or severe inflammatory
disorders refractory to alternate therapy
Supplemental oxygen therapy may be
necessary
Mechanical breathing assistance may
be helpful to some people with breathing difficulty from restrictive lung
disease
Inhalers
Expectorants
Antibiotics
Chemotherapy
In cases of obesity-related lung
disease, weight loss and exercise can help reduce the resistance to breathing
caused by excess fat
Severe, end-stage restrictive lung
disease (such as idiopathic pulmonary fibrosis) may be treated with lung
transplantation
RESTRICTIVE LUNG DISEASES – Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
COAL WORKER’S PNEUMOCONIOSIS –
Causes, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and
Management
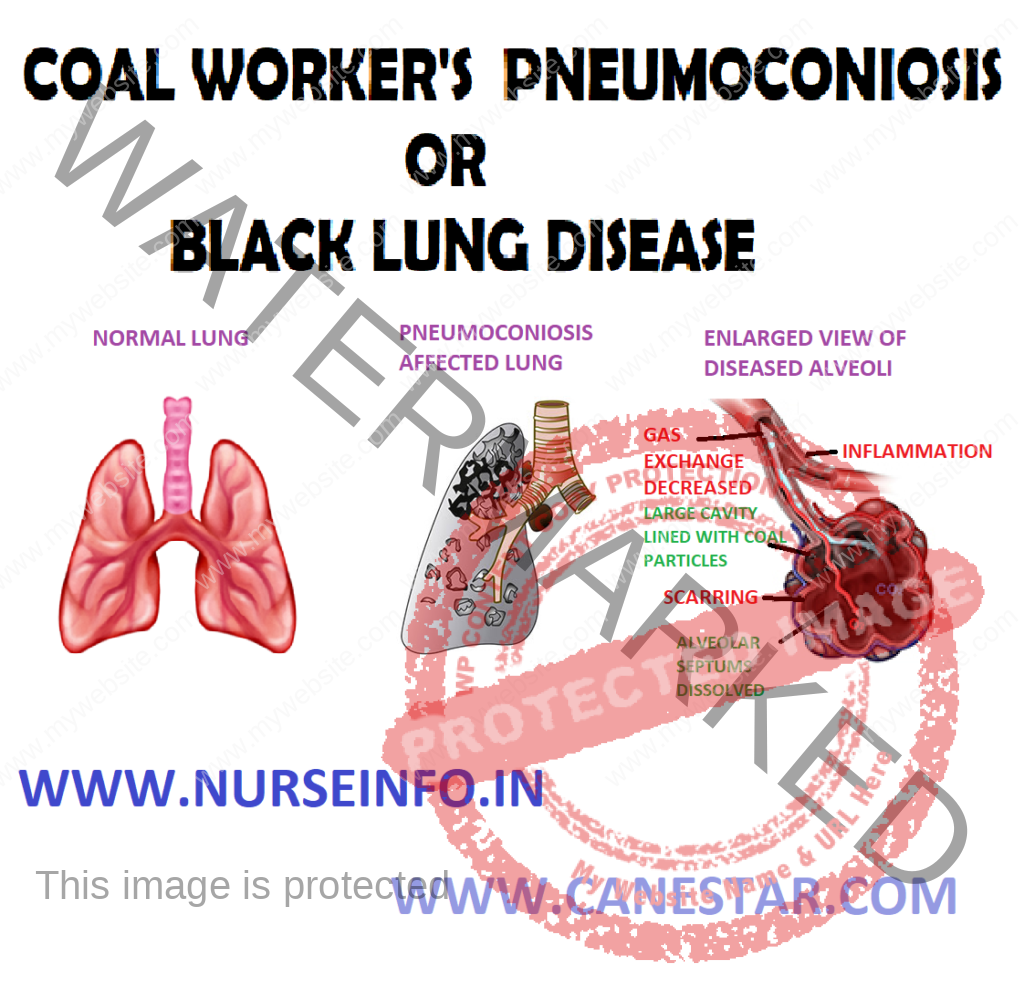
Coal worker’s pneumoconiosis (CWP)
can be defined as the accumulation of coal dust in the lungs and the tissue’s
reaction to its presence
Pneumoconiosis, also known as Black
Lung Disease, is an occupational lung disease caused by inhaling coal dust.
There are two types of pneumoconiosis – simple, known as coal worker’s
pneumoconiosis (CWP) and complicated, known as progressive massive fibrosis
(PMF)
CAUSES
Type of dust: more silica increases
the risk of fibrosis. Coal rankings are as follows:
High: this coal is older and has the least amount of volatile matter
(e.g. anthracite coal)
Medium: this coal is of moderate age and has a greater amount of volatile
matter (e.g. bituminous coal)
Low: this coal is younger and has the greatest amount of volatile matter
(e.g. lignite coal)
Age at first exposure
Length of time spent underground
Smoking
Size of dust particles
Type of job: certain job requires
more exposure to dust. Most dust is found at the coal face; therefore,
individuals who work directly on the cutting of the coal have the highest
exposure. The following list details dust exposure related to job title,
beginning with the highest exposure:
Cutting-machine operator: this worker cut coal directly at
the face. Respirable dust levels are highest here
Roof bolters: these individuals drill through rock and thus
also exposed to silica. The continuous mine operator, loading machine operator,
and shot firer are also exposed to higher amounts of respirable dust
Train operators: they drop sand onto the tracks for traction
and may, therefore, develop silicosis
Motormen, brakemen, drivers and shuttle care operators: these
individuals have less dust exposure because the coal has already been cut by
the time they work with it, thus decreasing their exposure to respirable dust.
Mechanics, electricians and maintenance personnel: they have
the least amount of dust exposure
PATHOPHYSIOLOGY
Coal dust
that enters the lungs can neither be destroyed nor removed by the body —- the
particles are engulfed by resident alveolar or interstitial macrophages —-
remain in the lungs, residing in the connective tissue or pulmonary lymph nodes
—- coal dust provides a sufficient stimulus for the macrophages to release
various products, including enzymes, cytokines, oxygen radicals, and fibroblast
growth factors —- aggregations of carbon-laden macrophages can be visualized
under a microscope as granular, black areas. In serious cases, the lung may
grossly appear black —- these aggregations can cause inflammation and
fibrosis, as well as the formation of nodular lesions within the lungs —- the
centers of dense lesions may become necrotic due to ischemia, leading to large
cavities within the lung
SIGNS AND SYMPTOMS
First stage is called simple
pneumoconiosis, which is characterized by chronic cough, fever, expectoration
and dyspnea on exertion. This is associated with little ventilator impairment.
This stage will develop after 10-12 years of exposure
Second stage is called progressive
massive fibrosis: it is irreversible and continues even after cessation of the
exposure. Prognosis is not good.
DIAGNOSTIC EVALUATION
History of exposure
Lung function test: varies from
normal to obstructive or restrictive or combination of both. Diffusion
decreased. Dyspnea on exertion. X-ray chest: small nodules, 1-10 mm in upper
lung zones, and ground glass appearance of the lung
Radiograph of CWP
Pulmonary function tests: used to
test the ability of the lungs to take in air (inspiration). Often used in
conjunction with the X-ray chest. Forced vital capacity (FVC) and FEV1 (forced
expiratory volume in one second) are used to diagnose lung disease
ASBESTOSIS – Etiology, Symptoms, Pathophysiology,
Diagnosis and Treatment
Asbestosis
is a chronic inflammatory and fibrotic medical condition affecting the
parenchymal tissue of the lungs caused by the inhalation and retention of
asbestos fibers.
ETIOLOGY
Tiny
asbestos fibers can get stuck deep inside the lungs. Inhaling asbestos fibers
can cause scar tissue to form inside the lungs. This scar tissue does not
expand and contract normally, which interferes with breathing. Asbestos fibers
may remain in the lungs for a lifetime. In some cases, the fibers might damage
the lungs or the membrane covering the lungs, leading to illness and even death
SYMPTOMS OF ASBESTOSIS
Dry inspiratory crackles: which are
clicking or rattling noises made by the lungs during inhalation
‘Clubbing of the fingers’: which may
include softening of the fingernail beds, and bulging and of the end of the
finger
Misshapen nails: caused by a decrease
of oxygenated blood flow to the extremities
Shortness of breath
A persistent dry cough
Loss of appetite with weight loss
Chest tightness or pain
OTHER SYMPTOMS OF ASBESTOSIS
Coughing
Chest pain
Blood in the sputum
Swelling in the neck or face
Difficulty swallowing
Loss of appetite
Weight loss
PATHOPHYSIOLOGY
Asbestos is
the scarring of lung tissue around terminal bronchioles and alveolar ducts —-
resulting from the inhalation of asbestos fibers —- when such fibers reach
the alveoli in the lung, where oxygen is transferred into the blood —-
activation of the lung’s local immune system —- provoke an inflammatory
reaction —- a slow ongoing progression of the immune system —- attempt to
eliminate the foreign fibers —- macrophages phagocytose the fibers, releasing
cytokines —- which eventually form a fibrous mass —- the result is
interstitial fibrosis —- the fibrotic scar tissue causes alveolar walls to
thicken —- which reduces elasticity and gas diffusion, reducing oxygen
transfer to the blood as well as the removal of carbon dioxide
DIAGNOSIS
Complete physical examination
Chest X-ray
Lung function tests
A lung biopsy, in which tissue is
removed by surgery, is the most reliable way to confirm the presence of
microscopic asbestos fibers because X-rays cannot detect asbestos fibers in the
lungs
TREATMENT
Oxygen therapy to relieve shortness
of breath
Respiratory physiotherapy to remove
secretions from the lungs
Medications to thin secretions and
relieve pain
ASBESTOSIS – Etiology, Symptoms, Pathophysiology, Diagnosis and Treatment