Hand washing
involves both mechanical and chemical action. Careful washing of the hands
reduces the number of bacteria
Hand washing
is the single most important means of preventing the transmission of infectious
agents. Careful washing of hands using soap, water and nail brush reduces the
number of bacteria
Hand washing
is most important to reduce the numbers of bacteria. Soap and water will
emulsify fat, clean the hands and reduces the number of microorganisms
Purpose
To encourage
hand washing in following situations:
On starting and completion of duty
shifts
Before performing any invasive and
non-invasive procedure
Between handling of patient and
between procedures on same patient
After handing contaminated articles
like, urinal and bedpan, etc
After dealing with situations when
microbial contamination is likely, even if gloves are used
Equipment
Soap
Bowel with 7% Lysol
Nail brush
Towel
Running water
Precautions Taken During Hand Washing
Nails should be short to avoid the
dirt and microorganism
Remove watch and jewelry from hands
and wrists
Fold back sleeves above elbow (if
necessary)
Stand away from wash basin
Avoid splashing water against uniform
clothes
Procedure
Turn on tap using elbow and regulate
flow of water
Wet hands and lower arms under
running water keep hand forearms lower than elbows during washing
Apply soap to hands, replace soap in
dish
Scrub hands area between fingers and
wrist in rotatory movement for 15 to 30 seconds
Clean finger nails with brush or use
finger nails of other hand
Rinse hands and wrist, forearm and
elbow in running water. Ensure that hand and forearms are lower than elbows
during washing
Close tap with elbow
Dry hands from fingers to wrist and
forearms now hold arms above elbow
Hands should be washed at the following times:
When visibly contaminated with blood,
body fluids, or tissues
After every patient contact
After removal of gloves and other
protective wear or equipment
Before eating, drinking, smoking,
applying makeup, or changing contact lenses outside of the lab, and after using
the lavatory facilities
Before all other activities that
entail hand contact with mucous membranes or a break in the skin
Periodically during the day when routinely handling and testing bloody fluid
Do’s of Handwashing:
Wet Your Hands Thoroughly:
Start by wetting your hands with clean, running water before applying soap.
Use Enough Soap:
Dispense an adequate amount of soap to create a good lather.
Scrub for at Least 20 Seconds:
Scrub your hands for at least 20 seconds, ensuring that you cover all surfaces, including the backs of your hands, between your fingers, and under your nails.
Pay Attention to Fingernails and Jewelry:
Clean under your fingernails and around any jewelry, where germs can hide.
Rinse Thoroughly:
Hold your hands under clean, running water to rinse off the soap and loosened dirt and germs.
Dry Your Hands:
Dry your hands thoroughly using a clean towel or an air dryer. Ensure your hands are completely dry.
Use a Paper Towel to Turn Off the Faucet:
If possible, use a paper towel to turn off the faucet to avoid recontaminating your hands.
Use Hand Sanitizer When Needed:
If soap and water are not available, use an alcohol-based hand sanitizer with at least 60% alcohol content.
Don’ts of Handwashing:
Don’t Rush:
Take the time to wash your hands thoroughly. Rushing may result in incomplete cleaning.
Don’t Neglect Key Areas:
Ensure you clean all parts of your hands, including the wrists, between fingers, and under the nails.
Don’t Skip Hand Drying:
Drying your hands is an essential step, as wet hands can spread germs more easily than dry hands.
Don’t Ignore Proper Technique:
Follow the recommended technique for handwashing, including the proper sequence and duration of scrubbing.
Don’t Use Hot Water:
While warm water can be more comfortable, excessively hot water may lead to skin irritation. Use warm water that is comfortable for you.
Don’t Touch Surfaces After Washing:
Avoid touching surfaces with your clean hands after washing. If you must touch surfaces, use a clean paper towel.
Don’t Use Expired Soap:
Check the expiration date of the soap to ensure its effectiveness.
Don’t Forget to Perform Hand Hygiene at Critical Moments:
Remember to wash your hands after using the restroom, before eating, after touching potentially contaminated surfaces, and before and after caring for someone who is sick.
Surgical handwashing, also known as a surgical scrub, is a specialized and thorough hand hygiene procedure performed by healthcare professionals before entering the operating room or engaging in surgical procedures. The purpose of surgical handwashing is to eliminate or reduce the number of microorganisms on the hands and forearms to prevent the introduction of infections into the sterile surgical environment. Here is a step-by-step guide for surgical handwashing:
Surgical Handwashing Procedure:
1. Remove Jewelry and Accessories:
Begin by removing all jewelry, including rings, watches, and bracelets, from your hands and wrists. Jewelry can harbor microorganisms and interfere with proper handwashing.
2. Pre-rinse:
Pre-rinse your hands and forearms under running water. This helps to remove loose dirt and debris.
3. Apply Antiseptic Solution:
Dispense the appropriate antiseptic solution or surgical scrub solution onto your hands and forearms. Common antiseptic solutions include chlorhexidine gluconate or povidone-iodine.
4. Scrub the Fingernails:
Use a nail brush or the bristles of your scrub brush to clean under and around the fingernails. Pay attention to each finger and the area around the nails.
5. Scrub the Hands and Forearms:
Rub your hands and forearms with the antiseptic solution for the recommended duration, often ranging from 2 to 5 minutes. Follow a systematic scrubbing pattern, including the backs of hands, between fingers, and up to the elbows.
6. Pay Attention to Specific Areas:
Focus on high-risk areas such as the fingertips, the webbing between fingers, and the wrists, as these areas are more prone to contamination.
7. Keep Hands Elevated:
Keep your hands elevated during the scrub to prevent the runoff of water from contaminating your scrubbed hands.
8. Rinse:
Rinse your hands and forearms thoroughly under running water to remove the antiseptic solution. Ensure that water flows from your fingertips towards your elbows.
9. Repeat If Necessary:
Some surgical scrubs may require a second application of the antiseptic solution and a repeat of the scrubbing process. Follow the specific guidelines of the facility or procedure.
10. Dry Hands with Sterile Towel: – Dry your hands and forearms using a sterile, lint-free towel. Pat them dry rather than rubbing.
11. Don Sterile Gown and Gloves: – After completing the surgical scrub, don a sterile gown and gloves without contaminating the scrubbed hands.
12. Maintain Sterility: – Throughout the surgical procedure, healthcare professionals must maintain sterility by avoiding contact with non-sterile surfaces and minimizing unnecessary movements.
Surgical asepsis: the hands should be thoroughly cleansed for about 3 to 5 minutes (in operation room, hands are scrubbed up to 10 minutes)
Surgical Scrub
Wet hands and forearms
Apply soap (containing 3%
hexachlorophene) to make a good lather
Clean under nails, which should be
kept very short (30 seconds)
Rinse thoroughly
Apply soap to hand and arms again
Scrub with brush so that every area
receives 15 to 30 strokes
Add small amount of water frequently
and use just enough detergent to maintain lather
Rinse the arms and hands
In rinsing keep palms higher than the
elbow so that water does not run over palms from the arms
Dry on a sterile towel moving from
the palms to the arms
General Instructions
When washing hands, they are held
above the level of the elbow (in surgical asepsis the elbow are considered more
contaminated than the hands)
The water should run from least
contaminated are hands to the area of great contamination (elbows)
It is important to put soap well and
scrub with a brush and rinse thoroughly with water several times
A sterile towel is used to wipe the
hands and arms. Starting from the palms to the elbows
The gown is to worn by the infected
person when he is transported outside his room. The gown prevents the patients
contaminated clothing from touching clean areas
The gowns are worn by the nurses who
caring for the persons whose resistance to infection is diminished, e.g.
premature babies
The outside of the gown is considered
to be highly contaminated and the inside of the gown is considered to be clean
If the gown is to be re-used, hang
the gown inside the patients unit with the contaminated side folded out
Hang the gown outside the patients
unit with the contaminated side folded in
Sterile gowns
are worn in the operating room and the delivery room and whenever open wounds
are present which necessitate a sterile technique, e.g. to attend to patient
with burns
Procedure
Put on the head cap and mask first
Scrub hand thoroughly
Dry the hands with sterile towel
Pick up the gown by grasping the
folded gown at the neck. Stand well back about one foot from the sterile bundle
and the table
Unfold it by keeping the gown away
from the body do not shake the gown
Hold the gown at the shoulder
(inside) and put each hand alternately into the arm holes
Extend the arms and hold hands upward
at the shoulder height
The circulating nurse than assist her
in pulling the sleeves by working from behind and holding the gown from the
inside
The gown is then fastened at the neck
by the circulating nurse and the open edges are the folded or held together
The waist ties are then fastened by the circulating nurse from behind
Surgical gowning is a process that healthcare professionals follow to put on a sterile surgical gown as part of the preparation for entering an operating room or engaging in a sterile procedure. The purpose of surgical gowning is to maintain aseptic conditions and prevent the introduction of contaminants into the sterile field. Here is a general guide for surgical gowning:
Surgical Gowning Steps:
1. Perform Hand Hygiene:
Wash hands thoroughly with soap and water or use an alcohol-based hand sanitizer before starting the gowning process.
2. Select a Sterile Gown:
Choose a sterile surgical gown appropriate for the specific procedure. Gowns are typically packaged in a way that allows for aseptic opening.
3. Inspect the Gown:
Examine the gown for any visible damage or defects. If the gown is compromised in any way, do not use it, and obtain a replacement.
4. Open the Gown Package:
Open the gown package aseptically. Be cautious not to touch the inside of the gown with bare hands.
5. Allow the Gown to Unfold:
Allow the gown to unfold without touching its inside surfaces. The outside of the gown is considered sterile.
6. Insert Arms into Sleeves:
Slip your arms through the sleeves of the gown without touching the outer surface. Keep your hands and wrists within the gown sleeves.
7. Secure Gown at Neck:
If the gown has a hook-and-loop or tie closure system, secure the gown at the neck, making sure it covers the front of the neck area.
8. Ask for Assistance If Needed:
If assistance is available, ask a colleague to secure the gown at the back, ensuring a snug fit without any exposed skin.
9. Secure Gown at the Back:
Secure the gown at the back using the ties or closures provided. The back of the gown should be covered entirely.
10. Allow Colleagues to Assist: – If additional assistance is needed to secure the gown, colleagues may help without compromising the sterility of the gown.
11. Maintain Sterile Field: – Be mindful of maintaining the sterile field throughout the gowning process. Avoid touching non-sterile surfaces or reaching behind you.
12. Don Sterile Gloves: – After gowning, proceed to don sterile gloves. The gloves should be put on over the cuffs of the gown sleeves.
13. Perform a Sterile Gowning Check: – Perform a final check to ensure that the gown is secure, covers all necessary areas, and is free of visible defects.
14. Enter Sterile Area: – Once properly gowned and gloved, enter the sterile field or operating room without touching non-sterile surfaces.
Gloving technique is a crucial aspect of maintaining aseptic conditions in healthcare settings, particularly in sterile environments such as operating rooms or during certain medical procedures. Proper gloving technique helps prevent contamination and ensures the safety of both healthcare professionals and patients.
Medical Gloving
Gloves are
used in the medical asepsis to protect the nurse from pathogens. They serve as
a barrier when the nurse handles articles contaminated by the feces or wound
Gloves used
in the medical asepsis need not to be sterile. These are changed after
attending each of the patient discharges. Before wearing the gloves, hand wash,
dry and powder them and then put on clean gloves
Purpose
To protect the nurse from pathogens
To serve as a barrier when nurses
handles contaminated articles
To protect the patients with poor
resistance
It is used for the cleaning for the
patient
While Wearing Gloves
Wash hands
Dry the hands and apply powder for
easy insertion of gloves
Put on the clean gloves
After Use
Remove the gloves and discard them in
the container with antiseptic lotion
Wash hands thoroughly
General Instructions
Every surgical patient should be
protected from respiratory, intestinal, skin and other general infections
They are to be provided with
uncontaminated dishes, bed linen, clothing and other articles
Removing Isolation Clothing
Untie the gown at the waist
Slip a finger from one hand
underneath the cuff of the glove on the opposite hand
Pull the glove off, turning inside
out as it is removed
Deposit in the designed waste
receptacle. Repeat the procedure on the opposite hand
Remove the mask by untying the ties
or slipping the rubber bands from behind the ears. Be careful not to touch the
front of the mask. Holding the mask by the ties deposit in the designed waste
receptacle
Untie the tie at the neck of the
gown. Using the ties, pull the gown down toward the front of the body
Pull one arm of its sleeve, turning
the sleeve inside out as you proceed. Repeat, using the other arm. Be sure the
front of the gown does not contact your hands or uniform. Deposit the gown in
the designated waste receptacle
Wash hands. Put on lab coat
SURGICAL GLOVING
Procedure
Scrub hands using a brush and soap
under running water
Open the sterile package of gloves
with a sterile forceps before scrubbing if no assistant is available
After scrubbing, dry hands on a
sterile towel
Apply sterile powder on both hands
The first gloves are drawn on by
touching the inside of the gloves cuff
The second by placing the gloves hand
under the cuff
The sterile gown is worn. It should
be put on before the gloves so that the glove cuffs may be drawn up over its
sleeves
Medical Gloving, Surgical Gloving – Purpose, Procedure, Instructions, After Use
Donning Sterile Gloves:
1. Perform Hand Hygiene:
Wash your hands thoroughly with soap and water or use an alcohol-based hand sanitizer to ensure your hands are clean before starting the gloving process.
2. Choose the Correct Glove Size:
Select the appropriate size of sterile gloves. Gloves that are too tight may tear, while those that are too loose may compromise dexterity.
3. Open the Outer Glove Package:
Grasp the outer package of sterile gloves without touching the inside. Open the package carefully to expose the inner glove package.
4. Put on the First Glove:
With the glove package still intact, use the hand opposite to your dominant hand to pick up the glove for your dominant hand.
Hold the glove by the folded cuff and insert your dominant hand into the glove without touching the exterior surface.
5. Secure the First Glove:
Once the first glove is on, use the gloved hand to pick up the second glove by the inside surface of the cuff.
6. Put on the Second Glove:
With the first glove-covered hand, insert your fingers into the second glove without touching the outside of the glove. Pull the second glove over your non-dominant hand.
7. Adjust and Secure Gloves:
Adjust the gloves for a comfortable fit, ensuring that they cover the hands and wrists adequately. Secure the cuffs of both gloves to prevent them from rolling down.
8. Perform a Gloving Check:
Inspect the gloves for any visible defects, such as tears or punctures. If you notice any issues, remove the gloves, perform hand hygiene, and start the gloving process again.
Doffing Sterile Gloves:
1. Grasp the Outside of the Glove:
Pinch the outside of the glove near the wrist with your opposite hand. Avoid touching your skin or clothing.
2. Peel Off the First Glove:
Peel off the first glove by turning it inside out as you pull it away from your hand. Hold the removed glove in the gloved hand.
3. Hold the Removed Glove:
Keep the removed glove in your gloved hand.
4. Slide Fingers under the Cuff:
Slide your fingers from the bare hand under the remaining glove cuff, being careful not to touch the outside of the glove.
5. Peel Off the Second Glove:
Peel off the second glove by turning it inside out, covering the first glove. The removed gloves should be inside-out and contained within the remaining glove.
6. Dispose of Gloves:
Discard the used gloves into the appropriate waste container without touching the exterior surfaces.
7. Perform Hand Hygiene:
Wash your hands thoroughly or use an alcohol-based hand sanitizer after removing the gloves.
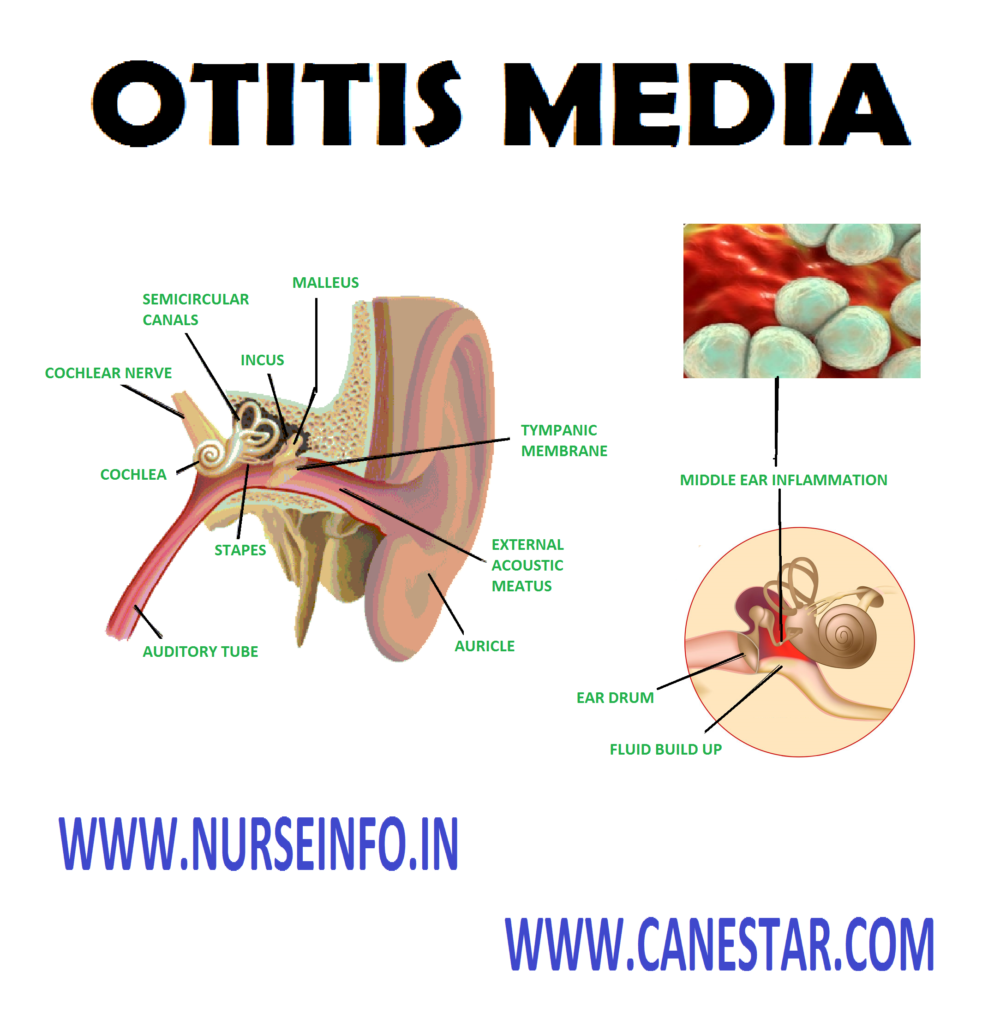
OTITIS MEDIA – Types, Etiology, Signs
and Symptoms, Diagnostic Evaluation, Complications, Management and Nursing
Management
Otitis media
refers to inflammation of the middle ear. Acute otitis media occurs when a
cold, allergy, or upper respiratory infection, and the presence of bacteria or
viruses lead to the accumulation of pus and mucus behind the eardrum, blocking
the Eustachian tube and characterized by earache and swelling.
When fluid
accumulates in the middle ear, the condition is known as otitis media with
effusion. This occurs in a recovering ear infection.
TYPES
Acute otitis media: It is usually of
rapid onset and short duration. Acute otitis media is typically associated with
fluid accumulation in the middle ear together with signs or symptoms of ear
infection and may associate with drainage of purulent material (pus, also
termed as suppurative otitis media)
Chronic otitis media: It is a persistent
inflammation of the middle ear, typically for a minimum of a month. Following
an acute infection, fluid may remain behind the eardrum for up to three months
before resolving. Chronic otitis media may develop after a prolonged period of
time with fluid or negative pressure behind the eardrum.
ETIOLOGY
Winter is
high season for ear infections. They often follow a cold. Some factors that
increase a risk for middle ear infections include:
Crowded living conditions
Attending daycare
Exposure to secondhand smoke
Respiratory illnesses such as common
cold
Close contact with siblings who have
cold
Having a cleft palate
Allergies that cause congestion on a
chronic basis
Premature birth
Not being breastfed
Bottle-feeding while lying down
SIGNS AND SYMPTOMS
Symptoms of
an ear infection may include:
Acute otitis media (AOM)
Pulling at ears
Excessive crying
Fluid draining from ears
Sleep disturbances
Fever
Headaches
Problems with hearing
Irritability
Difficulty balancing
Symptoms of
fluid build-up may include:
The symptoms
of swimmer’s ear include: Itching inside the ear, watery discharge from the
ear, severe pain and tenderness in the ear, especially when moving your head or
when gently pulling on the earlobe a foul smelling, yellowish discharge from
the ear and temporarily muffled hearing (caused by blockage of the ear canal).
Popping, ringing or a feeling of
fullness or pressure in the ear
Trouble hearing
Balance problems and dizziness
DIAGNOSTIC EVALUATION
History, a physical examination and
an ear examination
Pneumatic otoscope to look at the
eardrum for signs of an ear infection or fluid buildup
Ear
Infection Syndrome
The symptoms
of an ear infection in adults are: earache (either a sharp, sudden pain or a
dull, continuous pain); A sharp stabbing pain with immediate warm discharge
from the ear canal; a feeling of fullness in the ear; nausea muffled hearing;
ear drainage.
In children,
the symptoms are: Tugging at the ear; poor sleep fever irritability,
restlessness; ear drainage; diminished appetite; crying at night when lying
down.
Tympanometry: it measures how the
eardrum responds to a change of air pressure inside the ear
Hearing tests
Tympanocentesis: This test can remove
fluid if it has stayed behind the eardrum (chronic otitis media with effustion)
Blood tests, which are done if there
are signs of immune problems
COMPLICATIONS
Infratemporal
infections can include:
Tympanic membrane perforation
Mastoiditis
Facial nerve palsy
Acute labyrinthitis
Petrositis
Acute necrotic otitis
Chronic otitis media
Intracranial
infections can include:
Meningitis
Encephalitis
Brain abscess
Otitic hydrocephalus
Subarachnoid abscess
Subdural abscess
Sigmoid sinus thrombosis
MANAGEMENT
Antibiotic
is the only treatment for otitis media
Antimicrobials
AMOXICILLIN
Dosage: 80
to 90 mg per kg per day, given orally in two divided doses
Comments:
first-line drug. Safe, effective and inexpensive
AMOXICILLIN
(augmentin)
Dosage: 90
mg of amoxicillin per kg per day given orally in two divided doses
Comments:
second-line drug. For patients with recurrent or persistent acute otitis media,
those taking prophylactic amoxillicin, those who have used antibiotics within
the previous month, and those with concurrent purulent conjunctivitis
AZITHROMYCIN
Dosage: 30
mg per kg, given orally
Comments:
for patients with penicillin allergy. One dose is as effective as longer
courses
AZITHROMYCIN
(Three-day course)
Dosage: 20
mg per kg once daily, given orally
Comments:
for patients with recurrent acute otitis media
AZITHROMYCIN
(five-day course)
Dosage: 5 to
10 mg per kg once daily, given orally
Comments:
for patients with penicillin allergy (type 1 hypersensitivity)
CEFDINIR
Dosage: 14
mg per kg per day, given orally in one or two doses
Comments:
for patients with penicillin allergy, excluding those with urticaria or
anaphylaxis to penicillin (i.e. type 1 hypersensitivity)
CEFPODOXIME
Dosage: 30
mg per kg once daily, given orally
Comments:
for patients with penicillin allergy, excluding those with urticaria or
anaphylaxis to penicillin (i.e. type 1 hypersensitivity)
CEFTRIAXONE
(Rocephin)
Dosage: 50
mg per kg once daily, given intramuscularly or intravenously. One dose for
initial episode of otitis media, three doses for recurrent infections
Comments:
for patients with penicillin allergy, persistent or recurrent acute otitis
media or vomiting
CEFUROXIME
(Ceftin)
Dosage: 30
mg per kg per day, given orally in two divided doses
Comments:
for patients with penicillin allergy, excluding those with urticaria or
anaphylaxis to penicillin (i.e. type 1 hypersensitivity)
CLARITHROMYCIN
Dosage: 15
mg per kg day, given orally in three divided doses
Comments:
for patients with penicillin allergy (type 1 hypersensitivity) may cause
gastrointestinal irritation
CLINDAMYCIN
Dosage: 30
to 40 mg per kg per day, given orally in four divided doses
Comments:
for patients with penicillin allergy (type 1 hypersensitivity)
TOPICAL AGENTS
CIPROFLOXACIN/HYDROCORTISONE
Dosage: 3
drops twice daily
HYDROCORTISONE/NEOMYCIN
Dosage: 4
drops three or four times daily
OFLOXACIN
Dosage: 5
drops twice daily (10 drops in patients older than 12 years)
ANALGESICS
ACETAMINOPHEN
Dosage: 15
mg per kg every six hours
ANTIPYRINE/BENZOCAINE
Dosage: 2 to
4 drops three to four times daily
IBUPROFEN
Dosage: 10
mg per kg every six hours
NURSING MANAGEMENT
Nursing
Diagnosis
Acute pain related to inflammation of
the middle ear tissue
Disturbed sensory perception:
auditory conductive disorder related to the sound of the organ
Acute pain related to inflammation of
the middle ear tissue
Intervention
Assess the level of intensity of the
client and client’s coping mechanisms
Give analgesics as indicated
Distract the patient by using
relaxation techniques: distraction, guided imagination, touching, etc
Disturbed sensory perception:
Auditory conductive disorder related to the sound of the organ
Intervention
Reduce noise in the client
environment
Looking at the client when speaking
Speaking clearly and firmly on the
client without the need to shout
Providing good lighting when the
client relies on the lips
Using the signs of nonverbal (e.g.
facial expressions, pointing, or body movement) and other communications
Instruct family or the people closest
to the client about the techniques of effective communication so that they can
interact with clients
If the client wants, the client can
use hearing aids
OTITIS MEDIA – Types, Etiology, Signs and Symptoms, Diagnostic Evaluation, Complications, Management and Nursing Management
Staff Nurse Jobs (Paramedical) in
Railways (RRB) – How to Join and Procedure in Railways Hospital
Indian
Railways is one of the biggest departments in India that hires employees for
different sectors that includes engineers, nurses etc. Indian Railways is
managed by Central Government of India and Railways Management Board.
Railways
have many facilities that are offered specifically for railways employees and
their family members. In those perks one huge benefit is Railways Hospitals,
these railways hospitals are established in such a way to benefit only railway
employees and their family members. These hospitals are categorized as
Divisional Hospitals and Production Unit hospital. Divisional hospitals are
functioning in cities where major railway lines are connected to different
cities and which acts as a hub for trains to check out their mechanical faults
and other services. Production Unit hospitals are located only in the location
and factory where locomotives are manufactured. It is established to help
employees on time to treat an accident or other medical ailments.
Staff Nurse
is included in Paramedical staff in Railway Hospital. There is separate board
to govern the administration and job vacancies for paramedical categories.
Staff nurse earns 44900 INR per month as initial pay. There is a medical
standard for paramedical staff classified as B1, C1 and C2.
Salary Details for Paramedical Staff
in Railways Hospital
There are
about 1.7 millions of employees working in Indian Railways in different
sectors. Railways recruitments are taken care by Railway Recruitment board. Railways nurses’ jobs come under Paramedical
department in Indian Railways. They will publish advertisements for Staff nurse
openings in Railways.
For applying
to the Staff Nurse Jobs once should have passed General Nursing and Midwifery
or B.sc (Nursing) from Colleges or institutions recognized by Indian Nursing
Council. A valid registration certificate authorized by Indian Nursing Council
to practice as Staff Nurse is mandatory to apply.
Candidates
between 20 years to 40 years of age can apply for this staff nurse opening with
railways. Age relaxation for SC/ST is 5 years and OBC is 3 years.
Railways
selection procedure has written examination, interview process and document
verification process like any other job. Once the candidate applies for the
Nurse opening through online in railways recruitment website the process
begins. The eligible candidate will be called for written examination along
with e- admits card or hall ticket. After the written examination, the railway
recruitment board will call the candidates who have passed the written
examination with the appropriate cut off for personal interview. Original Documents
will be verified on the process. Then the offer will be rolled out to the
eligible candidates.
Written
examination for nurses in railways contains Objective Multiple choice questions
(100 numbers) and duration will be 90 minutes. Questions will be from subjects
pertaining to nursing, Arithmetic, General – Science, Awareness, Reasoning,
Intelligence.
Exams are
conducted with local languages along with common languages like English, Hindi
and Urdu. Candidates can attend the exams in the language they prefer.
For every
wrong answer 1/3rd of the marks will be deducted.
There are many benefits while working in railways Pay scale will be high and yearly increment will be provided. Additional benefits from Central government will be provided for railway employees.
Staff Nurse Jobs (Paramedical) in Railways (RRB) – How to Join and Procedure in Railways Hospital
In India railways offer good salary for nurses
all over India. In India like many other countries government offers several
opportunities for nurses. Opportunities varies between Central and State
government opportunities. One of the best careers for nurses is with Railways
that comes under Central government. Railways have different openings for
nurses all over the India. Nurses can attend Railways Entrance exam and can get
placed in their Divisional hospitals and Production Unit hospitals all over
India. In railways, staff nurse earns average 32,400 INR per month. Nurses’
salary will get increased according to their education and band they are
working in railways.
STAFF NURSE SALARY BASED ON CONTRACT
On contract
basis, the staff nurse will earn average 21,190 INR per month. In COVID
emergency period, the staff will be appointed as contract employee and earns
approximately 44,900 INR per month. Along with basic pay, COVID emergency staff
nurse get DA + HRA per month. Nurse will be under Medical Classification C 1. Staff
nurse need to get certified on their normal eye vision and physical fit, to be
eligible to work in Railway Department.
Staff Nurse
(Medical Classification C 1) – contract basis in Railway Hospital – Monthly
Remuneration 21,190 INR per Month
COVID
Emergency Staff Nurse Opening (Medical Classification – Contract Basis in
Railway Hospital – Monthly Remuneration 44,900 INR + DA + HRA per Month
Permanent Position Salary for Staff
Nurse
Nurse who
works in railway department earns about approx 32,400 INR per month. According
to 7th pay commission, the staff nurse under medical standard (C1)
get 44,900 INR per month. Increment in nurse salary will depend on position,
band pay and grade. Highest position of nurse is from Chief Matron, Matron,
Nursing Sister and Staff Nurse.
Staff Nurse – Level as per 7th CPC (7) – Medical Standard (C1) – 44,900 INR per Month
In railways,
the salary structure is based on post, pay band and grade pay.
Chief Matron
Chief Matron
is the highest rank for nurses in railway department, their basic pay scale is
about 7450 to 11500 INR per month, it comes under pay band PB – 3, Pay bands
will be around 15,600 – 39,100 INR per month and grade pay will be 5400 INR per
month.
Matron
Matron is
the second most top position for nurses in railway department. Matron get basic
pay scale is about 6500 to 10500 INR per month, it comes under pay band PB – 3,
Pay Bands 15600 to 39100 INR per month and grade pay 5400 INR per month.
Nursing
Sister
Nursing
Sister Position comes after Matron, get basic scale 5500 to 9000 per month, and
it comes under pay band PB – 2; Pay Band will be 9300 to 34,800 INR per month
and Grade Pay 4800 INR per month.
Staff Nurse
Post
Present Scale (INR)
Name of Pay Band
Pay Bands (INR)
Grade Pay (INR)
Chief Matron
7450 – 11500
PB – 3
15600 – 39100
5400
Matron
6500 – 10500
PB – 3
15600 – 39,100
5400
Nursing Sister
5500 – 9000
PB – 2
9300 – 34800
4800
Staff Nurse
5000 – 8000
PB – 2
9300 – 34800
4600
When a nurse joins railways department they will start their career as staff nurse. Their basic pay scale is about 5000 to 8000 INR per month, it comes under Pay Band PB – 2, Pay band will be 9300 to 34,800 INR per month and Grade Pay 4600 INR per month.
A Nurse
average salary in India starts from 28,400 INR per month. There is difference
in salaries between nurse work in Government Sector and Private Sector. In
government hospital or sector, the nurse earns approximately 38,200 INR per month;
whereas a nurse who works in private sector earns close to 23,450 INR per
month. Nurse salary is determined by the following categories – sector,
location, grade and experience.
Railway Nurse Salary
In Railways
Department there are more openings for nurses in railways divisional hospital
and in production dispensaries. These divisional hospitals are located in all
major cities where main railways junctions are located. Railways Production
units also has dispensaries and small hospital in their production factory
(ICF) where nurses are recruited along with physicians. Their salaries are
structured by the Central Government of India along with the Railways
Department of India. Nurses have good scope to grow in the grade and salary in
railways. Following are the grades and average salaries of the nurses provided
in railways. Nursing Superintendent earns about 44,900 INR per Month (Level –
7) (plus DA and other allowances admissible). Other than salary, railway nurse
will get loan, PF, ESI and pension. Staff Nurse who works in Railways on
contract basis earns 21,000 INR per month as remuneration. Staff nurse who
works as a permanent staff in railways will earn nearly 40,000 INR per month.
Staff Nurse Salary in Central
Government Institution and Hospitals
Nurse salary
will depend on grade, education and experience. For instance, Nurse with Sister
Grade II will get 32,500 INR + 4600 allowance and Sister Grade II will earn
33,600 INR + 4800 allowance. In JIPMER, Psychiatric nurse earn 34,200 INR per
month + 4800 allowance.
In government hospitals, Assistant Nursing Superintendent earns 38,700 INR per
month + 5400 allowance. Sister Tutor will earn 15,400 to 39,100 INR per month +
5400 allowance. Nurse Superintendent gets 15800 to 39,200 INR per month + 6600
allowance. Chief Nursing Officer will get 15,200 to 39,300 INR + 7600
allowance.
In
ESIC (Employees State Insurance Corporation of India), staff nurse earns about
34,000 INR per month + 4300 allowance. Along with basic salary, ESIC nurse will
other benefits such as PF, ESI, Pension etc.
Indian Military Nursing (IMN) Salary
Nurse in
Indian Military will get Basic pay 15,300 INR + 5400 allowance + DA. Military
Nurses start as Rank of Lieutenant with years of experience, nurse salary will
be increased. After military service, nurse will get good pension and benefits.
Nurse Salary in Private Hospitals
Staff nurse
earns average 15,000 INR with nursing registration. Staff nurse depends on
location, education, grade and experience. Staff nurse with 5 to 8 years
experience will get 36,000 INR per month.
Staff Nurse Salary in Different Metropolitan Cities
Bangalore –
17,000 INR per Month
Delhi –
24,000 INR per Month
Mumbai –
22,000 INR per Month
Kolkata –
25,000 INR per Month
Kochi –
23,000 INR per month
Staff Nurse
Work in Government Hospitals and Private Hospitals will earn Basic salary
21,000 INR per Month + allowance.
Highest Paying Nursing Professions in
India
Chief
Nursing Officer is the highest Paying Nursing Profession in India; an average
officer will earn 74,000 INR per month. Main role is to oversee other managers
and directors in health care system.
Nursing
Superintendent will get average 68,000 INR per month. Nursing Hierarchy,
Nursing Superintendent is the second most top Nursing Profession in India.
Nursing
Supervisor will get average 37,000 INR per month. In order to climb up nursing
supervisor grade, staff nurse need to gain minimum 10 years experience. Nursing
supervisor will look after staff nurse and allocate work schedule for nurses.
Home Nurse
will earn average 35,000 INR per month. Their primary work is to take care
patient in home. Home nurse is based on location and experience.
Pediatric
Nurse – 25,000 INR per month (1 to 2 year Experience.
Pediatric
Nurse – More than 5 years experience will get 64,000 INR per month.
Staff Nurse
– 22,000 INR per month (1 to 2 years experience).
Staff Nurse
– 54,000 INR per month (more than 5 years experience).
ICU and
Critical Care Nurse – 25,000 INR per Month (1 to 3 years experience)
ICU and
Critical Care Nurse – 63,000 INR per Month (5 to 8 years experience)
Operation
Theatre (OT) Nurse – 28,000 INR per Month (1 to 3 years experience)
Home Nurse –
35,000 INR per Month
Nursing Supervisor
– 37,000 INR per Month
Nursing Superintendent
– 68,000 INR per Month
Chief Nursing Officer (CNO) – 74,000 INR per Month
Temperature
is a measurement of heat expressed in degrees. Body temperature may be defined
as the degree of heat maintained by the body
Temperature
means the degree of warmth or balance maintained between the heat produced
(thermogenesis) and heat lost (thermolysis) in the body
Temperature is defined as measuring/monitoring patient’s body temperature using clinical thermometer
Types of Thermometers:
Oral Thermometers:
These thermometers are placed under the tongue for temperature measurement.
It’s important not to eat or drink anything for a few minutes before using an oral thermometer to ensure accuracy.
Rectal Thermometers:
These thermometers are inserted into the rectum for temperature measurement.
They are often used for infants and young children but require caution and proper hygiene.
Axillary Thermometers:
Placed in the armpit, axillary thermometers are convenient for temperature measurement, especially in infants and young children.
They may take a bit longer to obtain a reading compared to oral or rectal measurements.
Tympanic (Ear) Thermometers:
Tympanic thermometers measure the infrared radiation emitted by the eardrum.
They are quick and easy to use but may require proper positioning for accurate results.
Temporal Artery Thermometers:
These thermometers use infrared technology to measure the temperature of the temporal artery on the forehead.
They are non-invasive and provide relatively quick results.
Infrared Forehead Thermometers:
These thermometers measure the infrared radiation emitted by the skin on the forehead.
They are quick and non-invasive but may be less accurate than some other methods.
Purpose
To determine body temperature
To assist in diagnosis
To evaluate the patients recovery
from illness
To plan immediate nursing
interventions
To evaluate the patients response
To recognize any variation from the
normal and its significant
Indications
Routine part of assessment on
admission for establishing a base-line data
As per agency policy to monitor any
change in patient condition
Before, during and after
administration of any drug that affects temperature control function
When general condition of patient
changes
Before and after any nursing
intervention that affects temperature of the patient
Normal Body Temperature for Adults
Oral: 37 degree Celcius or 98.6 degree F
Rectal: 37.6 degree Celcius or 99.6 degree F
Axillary: 36.4 degree Celcius or 97.6 degree F
The normal
body temperature of a person varies depending on gender, recent activity, food
and fluid consumption, time of day, and, in women, the stage of the menstrual
cycle. Normal body temperature can range from 97.8 degree F (or Fahrenheit,
equivalent to 36.5 degree celcius, or Celcius) to 99 degree F (37.2 degree
Celcius) for a healthy adult. A person’s body temperature can be taken in any
of the following ways:
Orally: temperature can be taken by mouth using either the classic glass thermometer, or the modern digital thermometers that use an electronic probe to measure body temperature
Rectally: temperatures taken rectally (using a glass or digital thermometer) tend to be 0.5 to 0.7 degrees F higher than when taken by mouth
Axillary: temperatures can be taken under the arm using a glass or digital thermometer. Temperature taken by this route tend to be 0.3 to 0.4 degree F lower than those temperatures taken by mouth
By ear: a special thermometer can quickly measure the temperature of the eardrum, which reflects the body’s core temperature (the temperature of the internal organs)
By skin: a special thermometer can quickly measure the temperature of the skin on the forehead
Body
temperature may be abnormal due to fever (high temperature) or hypothermia (low
temperature). A fever is indicated when body temperature rises about one degree
or more over the normal temperature of 98.6 degree F, according to the American
Academy of Family Physicians. Hypothermia is defined as a drop in body
temperature below 95 degree F
Factors Influences Heat Production
Metabolism – oxidation of food
Muscle activity – exercise
Strong emotional – excitement,
anxiety and nervousness
Change in atmospheric temperature
Disease condition – bacterial
invasion
Sympathetic stimulation – epinephrine
and norepinephrine
VITAL SIGN MEASUREMENT
Normal (oral): 35.8 degree celcius to 37.3 degree celcius
Oral temperature: place the thermometer in the mouth under the tongue and instruct patient to keep mouth closed. Leave the thermometer in place for as long as is indicated by the device manufacturer
Axillary temperature: usually 1 degree celcius lower than oral temperature. Place the thermometer in patient’s armpit and leave it in place for as long as is indicated by the device manufacturer
Tympanic membrane (ear) temperature: usually 0.3 degree celcius to 0.6 degree celcius higher than an oral temperature. The tympanic membrane shares the same vascular artery that perfuses the hypothalamus. Do not force the thermometer into the ear and do not occlude the ear canal
Rectal temperature: usually 1 degree celcius higher than oral temperature. Use only when other routes are not available
Radial pulse: use the pads of your first three fingers to gently palpate the radial pulse at the inner lateral wrist
Apical pulse: taken as part of a focused cardiovascular assessment and when the pulse rate is irregular. Apical heart rate should be used as the parameter indicated in certain cardiac medications (e.g. digoxin). Apical pulse rate should be taken for a full minute of accuracy and is located at the fifth intecostal space in line with the middle of the clavicle in adults.
Carotid pulse: may be taken when radial pulse is not present or is difficult to palpate
Respiration rate: normal testing respiratory rate = 10 to 20 breaths per minute
Count respiratory
rate unobtrusively while you are taking the pulse rate so that the patient is
not aware that you are taking the respiratory rate. Count for 30 seconds or for
a full minute if irregular
The average
BP for an adult is 120/80 mm Hg, but variations are normal for various reasons
The systolic
pressure is the maximum pressure on the arteries during left ventricular
contraction
The
diastolic pressure is the resting pressure on the arteries between each cardiac
contraction
The patient
may be sitting or lying down with the bare arm at heart level. Palpate the
brachial artery just above the antecubital fossa medially. Wrap the BP cuff
around the upper arm about 2.5 cm above the brachial artery
Palpate the
radial or brachial artery, and inflate the BP cuff until the pulse rate is no
longer felt. Then inflate 20 to 30 mm Hg more
Place the
bell of the stethoscope over the brachial artery, and deflate the cuff slowly
and evenly, noting the points at which you hear the first appearance of sound
(systolic BP), and the disappearance of sound (diastolic BP).
Oxygen
saturation (SpO2): a healthy patient will have a SpO2 of
> 97%. A pulse oximeter sensor attached to the patient’s finger or earlobe
measures light absorption of hemoglobin and represents arterial SpO2.
A visual
analog scale (VAS) consists of a line, usually 10 cm long whose ends are
labeled as the extremes of pain – ‘no pain’ to ‘worst pain’. A VAS may have
specific points along the line that are labeled with intensity denoting
adjectives or numbers. Those scales that use adjectives are called graphic
rating scales. Patients are asked to rate their pain along the line that best
represents the intensity of their pain. This distance between the no end and
the mark provided by the patient is measured and this gives the pain intensity
score
Factors Influences Heat Loss
Sleep: body temperature is low
Fasting: leads to decreased heat production
Illness and lower vitality: due to depressed nervous system, the heat production is lowered
Prolonged exposure to cold
Use of narcotic drugs
Body Heat is
lost through
Conduction: transfer of heat from body to substance (air, water and cloths) directly in contact
Radiation: transfer heat from body to heat waves which travel through the space
Evaporation: transfer to heat from body in form of vapors (liquid is converted into vapors)
Convection: it is transfer of heat from the surface of one subject to the surface, such as skin by movements of heated air or fluid particles
Preparation of the Equipment
If a thermometer is included in the
admission pack, keep it at the patient’s bedside and, on discharge, allow him
to take home
Otherwise, obtain a thermometer from
the nurse’s station or central supply department
If use an electronic thermometer,
make sure it’s been recharged
Wipe the thermometer before use
Equipment
Mercury or electronic thermometer,
chemical dot thermometer, or tympanic thermometer
Water soluble lubricant or petroleum
jelly (for rectal temperature)
Facial tissue
Disposable thermometer sheath or
probe cover
Alcohol sponge
Common Sites for Taking Body Temperature
Mouth
Axilla
Groin
Vagina
Rectum
Contraindications
Oral method
Patients who are not able to hold thermometer in their mouth
Patients who may bite the thermometer like psychiatric patients
Infants and small children
Surgery/infection in oral cavity
Trauma to face/mouth
Mouth breathers
Patients with history of convulsion
Unconscious/semiconscious/disoriented patients
Patients having chills
Uncooperative patients
Patients who cannot follow instructions
Rectal method
Patients after rectal surgery
Any rectal pathology (piles/tumor)
Patients having difficulty in assuming required position
Acute cardiac patient
Patients having diarrhea
Reduced platelet count
Axillary method
Any surgery/lesion in axilla
Types of Thermometer
The clinical thermometer: it is an instrument used for measuring temperature of bodily heat or cold in which the mercury remain stationary at registration point until shaken down
Electronic thermometer: it consist of a battery powered display unit, a thin wire cord and a temperature sensitive probe covered by a disposable plastic sheath to prevent transmission of infection separate probes are available for oral and rectal insertion
Disposable thermometer: it is a single use thermometer, made of thin plastic strips with chemically impregnated paper, they are used for children to take oral and axillary temperature only 45 second are needed to record temperature it is less accurate
Tympanic membrane thermometer: small hold device similar to hodoscope with disposable speculum. Infrared-sensing electronic and liquid crystal displays. Results are displayed 1 to 2 seconds after placing their speculum in the outer third of the ear canal. It is accurate
Scales of Thermometer
Centigrade/Celcius: boiling point 100
degree and freezing point zero degree
Fahrenheit: boiling point 212 degree
and freezing point 32 degree
Parts of Thermometer
A bulb contains mercury and in a
stem, mercury rises. There is graduated scale on the stem, which represents the
degree of temperature
The bulbs are of different sizes and
shapes. The oral thermometers are with along and slender bulbs. The rectal
thermometers are with short and fat bulbs
The stem has a curved surface which
magnifies the lines and figures on the scale. The stem has a flattened back
with a sharp ridge that makes is easier to read the scale. The flat surface
prevents rolling
Reason for Mercury Used in the Thermometer
Very sensitive to small changes in
temperature
Silver appearance helps in easy
visible
It’s boiling point is 357 degree
celcius ad freezing point is 39 degree F
The expansion of mercury is uniform
Mercury is 13.5 times heavier than
water, so small glass tube can be used
Care of Thermometer
Grasp the thermometer securely by the
upper end of the stem, never hold it by bulb
Shake it down by quick movements of
the wrist
Move away from articles before
shaking the thermometer
Be careful that the thermometer will
not fall or strike against anything
Thermometer is never washed with hot
water because heat expands the mercury
The used thermometer should be washed
with soap and water and should be disinfected with a disinfectant
Advantages of using mercury are low
price, wide availability and reliable accuracy
Disadvantages are delay for recording
and easy breakability
TEMPERATURE & THERMOMETER – Purpose, Indications, Vital Signs, Measurement, Preparation, Equipment Common sites, Contradictions, Thermometer – types, scales, parts, care
Measuring oral temperature is a common method to assess an individual’s body temperature.
Purpose
To determine the body temperature of
the patient
To aid in making diagnosis
Position the tip of the thermometer
under the patient’s tongue, as far back as possible on either side of the
frenulum linguae
Placing the tip in this area promotes
contact with superficial blood vessels and contributes to an accurate reading
Instruct the patient to close his
lips but to avoid biting down with his teeth
Biting can break the thermometer,
cutting the mouth or lips or causing ingestion of broken glass or mercury
Leave a mercury thermometer in place
for at least 2 minutes or a chemical dot thermometer in place for 45 seconds to
register temperature, for an electronic thermometer; wait until the maximum
temperature is displayed
For a mercury thermometer, remove and
discard the disposable sheath then read the temperature at eye level, noting it
before shaking down the thermometer, note the temperature, and then remove and
discard the probe cover
For the chemical dot thermometer,
read the temperature as the last dye dot that has changed color, or fired, then
discard the thermometer and its dispenser case
Preliminary Assessment
Determine the need of measure
client’s body temperature
Assemble equipment
Identify the patient, greet the
patient and explain the procedure
Place the client in comfortable
position, assess site most appropriate for temperature measurement
Wait 20 to 30 minutes before
measuring oral temperature if client has ingested hot or cold liquid or foods
Cutaneous thermometer: the patient has a skin sensor attached, which is a small sensor connected with the device measuring the temperature. It is usually attached to the fingers – the index finger of the right hand or to the toes. It is a reliable method of measuring temperature although it can be obscured by the patient’s movement or sweating.
The location
of the cutaneous sensor is altered in regular intervals to avoid a pressure
ulcer forming. The best place for the sensor is under the patient’s back, but
not in the area of shoulder blades, which is a high risk area of developing
pressure ulcers. This method is primary used in the overall monitoring of a patient
or a patient in postoperative care
Chemical thermometers: used for a quick indicative measuring of body temperature. These are placed on a dry forehead. The measured value is displayed by a color change. The measured value is only approximate. Another form of chemical thermometer is a strip, which is inserted into the mouth, either to the right or to the left towards the buccal mucosa
Equipment
Oral clinical thermometer
Swab in a container
Kidney basin or thermometer container
Blue pen
Watch with second hand
Graphic TPR chart
Paper bag
Procedure
Hold the color coded end or system
glass thermometer with finger tips
If thermometer stored in disinfectant
solution, rinse in cold water before using
Take swab and wipe thermometer bulb
end towards fingers in rotating fashion. Dispose of tissue
Read mercury level while holding
thermometer horizontally and gently rotating at eye level. If mercury is above
desired level, grasp at the tip of thermometer securely and sharply flick wrist
downward. Continue shaking until reading is below 35.5 degree celcius
Ask client to open mouth and gently place
thermometer under tongue in posterior sublingual, lateral to center of lower
jaw
Ask client to hold thermometer with
lips closed. Caution against biting down on thermometer
Leave thermometer in place for 2
minutes or according to agency policy
Carefully remove thermometer and read
at eye level while holding thermometer horizontally
After Care
Wipe secretions from thermometer with
soft tissue. Wipe in rotating fashion from fingers towards bulb. Dispose of
tissue
Wash thermometer in lukewarm water,
rinse in cold water, dry and replace in container
Record the temperature on the chart
Wash hands
Report any unusual variation to the
charge nurse
Contraindications
Injuries, inflammation and surgeries
of oral cavity
Infants, children below 6 years, and
patients who cannot retain thermometer in mouth
Unconscious, delirious,
non-cooperative and mentally disturbed patients
Patients with mouth breathing, convulsions,
oxygen masks, frequent and severe cough
ORAL TEMPERATURE – Purpose, Assessment, Equipment, Procedure, After care, Contradictions