GENITAL HERPES (HERPES SIMPLEX VIRUS) – General Characteristics, Cytology, Treatment and Prophylaxis
General Characteristics
Several viruses may be transmitted by sexual contact. Important among them are herpes simplex, human papilloma virus, molluscum contagiosum, hepatitis B virus, cytomegalovirus, Marburg virus, and AIDS.
HERPES GENITALIS
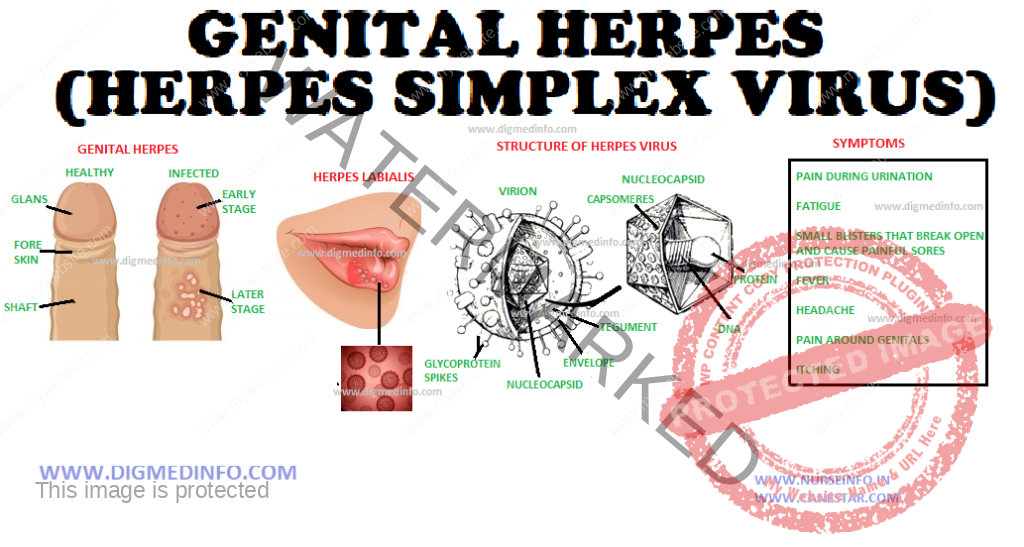
Herpes genitalis is caused by herpes simplex virus (HSV) type 2 and less frequently by HSV type 1. It is moderately infectious. The virus remains dormant in the presacral sensory ganglion cells. Periodically it moves into the skin through the axons of sensory nerves to produce recurrent attacks of herpes simplex locally. Factors which produce the reappearance of herpes are not clear. In many western countries herpes genitalis is emerging as the commonest among the STD. The disease is transmitted by sexual intercourse. The virus is shed from the lesions for up to 2 weeks after apparent healing. Infection of the baby during birth leads to neonatal herpes.
Clinical Features
The incubation period is 2-4 days or rarely longer. The onset of local lesions may be preceded by burning pain in the S1 to S5 dermatomes.
The lesions occur in the external genitalia of men and in the anal canal of homosexuals. Over the penis, it starts with erythema followed by the appearance of papules or vesicles which soon rupture to form shallow painful ulcers. Ultimately, crusts form which dry up and fall off leaving healed scars which fade. Tender inguinal adenopathy develops in the primary attack but not with recurrences. The lesions are infective throughout. Recurrences are generally much milder.
In women the primary lesion and recurrent attacks differ from each other considerably. Primary attack is severe, whereas, subsequent attacks are milder. Lesions occur usually in the vulva and adjacent skin areas. Morphology of the lesion is the same as in men. During the primary attack retention of urine may develop due to extreme pain on micturition. Herpes virus infection is directly or indirectly related to the development of carcinoma of the cervix, vagina, or vulva in later life as the virus is oncogenic. HSV 2 can also act as a cofactor with human papilloma virus for invasive cervical cancer.
Dissemination of the infection is rare in adults, but if it occurs it can be fatal. The skin, the central nervous system, and other internal organs may be affected. HSV2 can also act as a cofactor with human papilloma virus for invasive cervical cancer.
The newborn may acquire herpes during delivery if the mother has active lesions in the genitalia. Lesions develop in the baby usually within two weeks after birth. These occur more commonly with primary maternal herpes than with recurrent attacks. Both HSV-1 and HSV-2 may be responsible but the latter is more common. The lesions in the newborn include meningoencephalitis or generalized herpetic lesions involving several organs. If not treated, mortality and morbidity are very high.
DIAGNOSIS
Laboratory diagnosis is established by isolation of the virus from the lesions. Serological tests using blood include complement fixation test which becomes positive about a week after infections. In primary infection, the first sample is seronegative, the second sample shows a marked rise in titer. In recurrent herpes both samples give the same low titer. Herpes virus can be demonstrated by electron microscopy of vesicle fluid or tissue specimens.In herpes simplex encephalitis the CSF shows antibodies.
Cytology
Papanicolaou’s stained smears from vesicles show multinucleated giant cells with eosinophilic inclusions. In meningoencephalitis CSF shows changes. CT scan, MRI imaging and brain biopsy are employed to diagnose herpetic encephalitis.
Treatment and Prophylaxis
Treatment options for genital herpes:
First clinical episode: Treatment duration-7 days
Acyclovir 200 mg orally 5 times daily or 400 mg t.i.d or
Valacyclovir 1 g orally b.i.d or Famciclovir 250 mg t.i.d.
Recurrent infection: Treatment duration-5 days.
Acyclovir (oral) 200 mg 5 times daily or 400 mg t.i.d or
800 mg b.d or Valaciclovir 500 mg b.d or 1g once daily or
Famciclovir 125 mg twice daily
Suppressive therapy: The condition tends to recur often on cessation of treatment. If the recurrence is too frequent, >6 times a year, suppressive therapy is indicated for prolonged periods.
Acyclovir 400 mg bid or
Valaciclovir 500 mg or 1 g or
Famciclovir 250 mg bid continuously.
Recommended regimen for severe disease is acyclovir 5-10 mg/kg IV every 8 hours for 5-7 days or until clinical resolution is attained.
Severe herpes with coinfection with HIV: Acyclovir 400 mg orally 3-5 times daily until clinical resolution is attained.
Neonatal infection: Acyclovir 10 mg/kg IV 3 times daily for 10-21 days.
If the mother develops primary attack of herpes genitalis after the 36th week of pregnancy, caesarean section is indicated before the rupture of the membranes to avoid infection of the baby and the baby has to be watched for 2-4 weeks for the development of generalized herpes.