
BOWEL WASH – BOWEL ELIMINATION (Purpose, Contraindications, General Instructions, Methods Used, Solutions Used, Preliminary Assessment, Preparation of Patient and Environment, Equipment, Procedure and After Care)
UPDATED 2024
Bowel elimination is a basic bodily function that most people carry out in private and are often embarrassed to discuss publicly. Nurses will encounter patients with bowel elimination issues in all areas of care. Knowledge and understanding of both normal function and the problems that can occur with that process will enable nurses to support and care for patients with bowel elimination problems
BOWEL WASH
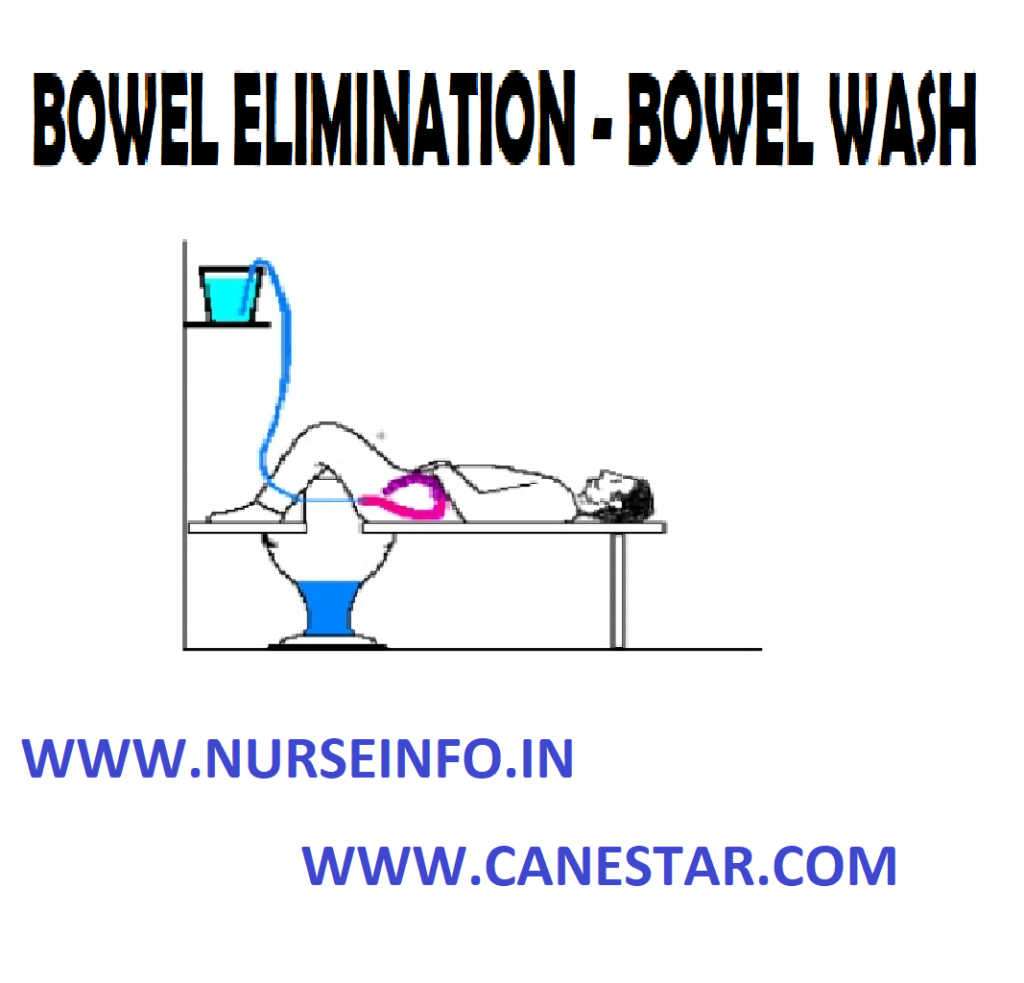
Bowel wash or colonic lavage or enteroclysis is defined as washing out colon with large quantities of solution.
Bowel irrigation or enteroclysis is defined as washing out of the colon after the feces has been expelled by using large quantities of prescribed solution
PURPOSE
- To prepare for diagnostic examination or before certain surgery
- To relieve inflammation
- To stimulate peristalsis
- To supply fluid and electrolyte those are absorbed from intestine
- To dilute and remove toxic agents
- To reduce temperature in hyperpyrexia
- To relieve fecal incontinence
- To supply medications locally
- To clean the colon of feces, gas and barium
- To treat infection and other pathological condition of colon
CONTRAINDICATIONS
- Rectal infection
- Fistula in anus
- Painful and bleeding hemorrhoids
- Painful skin lesions around the anus
- Massive carcinoma or tumors of the rectum
- Loose sphincter
- Polypus and diverticula of the intestine
GENERAL INSTRUCTIONS
- A cleaning enema should be given one hour before the colon irrigation
- The bladder should be emptied before colonic irrigations
- The temperature of the solution is kept constant throughout the procedure
- Allow only 200 to 300 ml of fluid to run into the rectum at a time
- Make sure that the return flow is not blocked
- Use a smooth and flexible rectal tube and lubricate it well
- Prevent air entry into the intestines
- Stop the procedure temporarily the patient complaints of pain
- Listen to the complaints of the patient and should not ignore any discomfort however small they may be
METHODS USED FOR BOWEL IRRIGATION
- Funnel and catheter
- Y connection and a rectal tube
- Two tube method
SOLUTION USED
- Tap water
- Cold water
- Normal saline
- Sodium bicarbonate 1 to 2 %
- Antiseptic solution KNMO4
- Boric solution 1 to 2 %
- Tannic acid 1: 100
- Alum 1: 100
TEMPERATURE OF THE SOLUTION
- Cleaning purpose 104 degree F (40 degree Celcius)
- Thermal effect 110 to 115 degree F (43.3 to 46 degree celcius)
- Reducing temperature 80 to 90 degree F (27 to 32 degree celcius) amount of water used for bowl, irrigation is 2 to 3 liters or till the return flow is clear
PRELIMINARY ASSESSMENT
Check
- Doctors order for any specific precautions
- Diagnosis of the patient
- General condition of the patient
- Self-care ability of the patient
- Mental status to follow instructions
- Any contraindications
- Need for any extra help
- Articles available in the unit
PREPARATION OF THE PATIENT AND ENVIRONMENT
- Explain the sequence of the procedure
- Arrange the articles at the bed side
- Provide privacy
- Place the Mackintosh and towel under the patient
- Place the patient in left later position
- Keep the bucket on a low stool or receive the out flow of fluid
- Remove the back rest and extra pillows
EQUIPMENTS
A clean tray containing
- Funnel and tubing with glass connection
- Mackintosh and towel
- Rectal tube placed in a kidney tray
- Vaseline
- Rag pieces in a container
- Hot and cold water in jugs
- Prescribed solution in jug
- Paper bag
- Bucket
- Toilet tray if needed
- Clean linen if needed
- Bath thermometer
PROCEDURE
- Wash hands thoroughly
- Prepare the solution at the required temperature
- Attach the tubing and the rectal tube with the funnel, pour solution in it and check for any leakage
- Lubricate the tip of the rectal tube about 4 inches
- Separate patient’s buttocks to visualize anus clearly and insert tip of tube about 4 to 5 inches, while patient takes deep breath
- Lower funnel below level of rectum and empty return flow into bucket
- Fill funnel again. Pour 200 to 300 ml of fluid each time. Raise funnel and allow fluid to run continuously. When 200 to 300 ml of fluid has gone in pinch tube before tunnel is completely. Lower and invert tunnel over bucket and siphon fluid, noting characteristics of return flow
- Repeat this process, till return flow is clear
- Remove the rectal tube by using rag pieces
AFTER CARE
- Remove rectal tube by using rag pieces
- Discard rag piece in to K-basin
- Place patient comfortably, provide bedpan if needed
- Change linen if soiled, replace equipment after cleaning
- Hand wash and record the procedure in nurse’s record sheet
HOT APPLICATION & COLD APPLICATION
PATIENT POSITIONING , COMFORT DEVICES
NURSING PROCEDURES LIST CLICK HERE
