RELAXATION TECHNIQUES – Introduction,
Relaxation with Guided Imagery and Steps of Relaxation Technique
INTRODUCTION
Synder and
Egan (1993) identified relaxation techniques as the major method used to
relieve stress, included in nursing interventions. Commonly used techniques
cited were progressive muscle relaxation, relaxation with guided imagery and
Senson’s relaxation response. The goal of relaxation training is to produce
response that counter the stress response.
Progressive
muscle relaxation involves tensing and releasing the muscles of the body in
sequence and sensing the difference in feeling. It is best if the person lies
on a soft cushion on the floor, in a quiet room, breathing easily. Self-taught
or instructor-directed exercise can involve learning to contract and relax
muscles in a systematic way beginning with face and ending with feet. This
exercise may be combined with breathing exercises that focus on inner self
RELAXATION WITH GUIDED IMAGERY
It is the
powerful use of imagination to achieve relaxation and/or direct attention away
from the undesirable sensations
The nurse
helps the person to select a pleasant scene or experience from his or her past.
This image serves as the mental device in this technique. As the person sits
comfortably and quietly the nurse guides him to review the scene; trying to
feel and relieve the imagery with all of the senses. A tape recording can be
made for description of science of experience for the pleasant son’s relaxation
response. Benson (1984) described the following steps for this response:
STEPS OF RELAXATION TECHNIQUE
Step 1: pick a brief phrase or word
that reflects your basic belief systems
Step 2: choose a comfortable position
Step 3: close your eyes
Step 4: relax your muscle
Step 5: become aware of your
breathing and start using your selected focus word
Step 6: maintain a passive attitude
Step 7: continue for a set period of
time
Step 8: practice the technique twice
a day
The response
combines meditation with relaxation. The other techniques of stress management
will also include the following:
Thought stopping: it is a
self-directed behavioral approach used to gain control of self-defeating
thoughts. When these thoughts occur the individual stops the thought process
and focuses on conscious relaxation
Exercise: regular exercise,
especially, aerobic movement, results in improved circulation, increased release
of endorphins on an enhanced sense of well-being
Humor: in the forms of laughter,
cartoons, funny movies, riddles, audiocassettes, comic books and joke books,
humor can be used for both the nurse and patient
Assertive behavior: open, honest,
sharing feelings, desires and opinions in a controlled way. The individual who
has control over one’s own life is less subject to stress
Social support: this may take the
form of organized support and self-help groups, relationship with family and
friends and professional help
In addition, meditation, breathing techniques, therapeutic touch, music therapy and biofeedback can be used as stress management technique
RELAXATION TECHNIQUES – Introduction, Relaxation with Guided Imagery and Steps of Relaxation Technique
PSYCHOSOCIAL THERAPIES – Behavior
Therapy, Modeling and Observational Learning, Characteristics of Dysfunctional
Families, Family Centered Approach and Technology for Family Therapy (MENTAL
HEALTH NURSING)
BEHAVIOR THERAPY
Behavior is
the internal and external response (feelings, thoughts, words, actions, and
physiological responses) a person makes to environmental stimuli. Behaviors are
measurable and able to be altered through behavior therapy. Behavior and
cognitive therapy is based on the concept that mental disorder represents
learned behavior. Learning principles are applied to modify these behaviors.
Behavioral techniques include the use of token economies, time out, and rewards
or reinforcement for desired behaviors
Types of
Behavior Therapy
Classical
conditioning: if an unconditioned stimulus (food) elicits an unconditioned
response (salivation in a hungry dog), then a conditioned stimulus (a bell)
paired with food, over time will condition the dog to salivate, a conditioned
response, upon hearing a bell. This conditioning can be used to explain and
treat learned anxiety, helplessness. Phobias, obsessive-compulsive disorder,
somatoform disorders and sexual disorders
Operant
conditioning: operant behavior (eating or dieting/exercise) is activity that is
strengthened or weakened by its consequences (weight gain or loss). Operant
behavior is influenced by reinforcement (something that increases the
probability of the response). The reinforcement meets a need and is goal
directed. Positive reinforcement (reward) strengthens a behavior; as well as
removal of a negative reinforcement. Punishment suppresses, but does not
eliminate a behavior. These behavioral principles can be applied in many
clinical situations
MODELING AND OBERVATIONAL LEARNING
A person can
imitate or learn through another’s performance. Observing the behavior of
another can influence a person to behave similarly, especially when the model
is rewarded for his/her behavior
Cognitive
therapy: cognition is the act or process of knowing. This form of therapy
corrects distorted thinking and its underlying faulty assumptions, beliefs and
attitudes. Cognitive therapy proposes that it is not the events themselves that
cause anxiety and maladaptive responses but rather people’s expectations,
appraisals and interpretation of these events. Cognitive therapists believe
that maladaptive responses arise from cognitive distortions. Such distortions
might include errors of logic, mistakes in reasoning, or individualized views
of the world that do reflect reality
Family
therapy: family therapy is broadly defined as “the attempt to modify the
relationships in a family to achieve harmony”. A basic assumption of family
therapy is that there are certain human behaviors patterns that can help people
grow and live creatively, while there are others that lead to dysfunction and
non-communicative action and result in emotional illness in the family
In family
therapy, the family is viewed as a system in which involves are interdependent,
a change in one part (member) of the system affects or creates change in all
the other parts (members). The focus is not on an individual identified client
but rather on the family as a whole. The basic concept of this form of
treatment is that it is more logical, faster, more satisfactory and more
economical to treat all members of a system of relationship than to concentrate
on the person who is supposed to be in need of treatment
CHARACTERISTICS OF DYSFUNCTIONAL FAMILIES
Families who
experience emotional difficulties usually have communication problems. They may
discount or ignore each other’s communication. They may “scapegoat” one of
their members by viewing and treating that member as though he or she is the
cause of all the family’s problems. They may create “triangles” in which two
family members form an alliance and exclude the third person.
Passive-aggressive behavior is common
FAMILY CENTERED APPROACH
Family
therapy is therapy for the entire family. It is based on the beliefs that the
behaviors of one person in the family affects everyone else in the family, and
that the presence of symptoms such as depression or anger in one family member
is a sign of disorder, pain or problems in the whole family systems. The
behavior of an individual cannot be understood without understanding the
behavior of other family members. Interventions are directed at the family as a
whole and their behaviors, not at an identified client. Family therapy promotes
family cohesion
TECHNOLOGY FOR FAMILY THERAPY
Genogram: a
three generational map of family structure and relationships which may be used
to diagnose and understand family’s history, problems, roles and values
Communication
techniques include
Discussing painful events or family
problems openly
Clarifying members thoughts, feelings
and messages
Dealing with anger openly and
non-judgmentally
Connecting feelings and facts, never
blaming
Expressing empathy with family
members
Experimental and homework activities,
such as planning a family vacation, doing a fun activity together or eating
meals together
PSYCHOSOCIAL THERAPIES – Behavior Therapy, Modeling and Observational Learning, Characteristics of Dysfunctional Families, Family Centered Approach and Technology for Family Therapy (MENTAL HEALTH NURSING)
PSYCHOPHARMACOTHERAPY – Principles of
Psychopharmacologic Therapy, Purposes of Psychopharmacotherapy, Reasons for
Non-compliance to Psychotropic Regimen, Services that Encourage Adherence to
Medication Regimen, Effects on Special Populations and Safe Medication
Administration: The Seven Rights (MENTAL HEALTH NURSING)
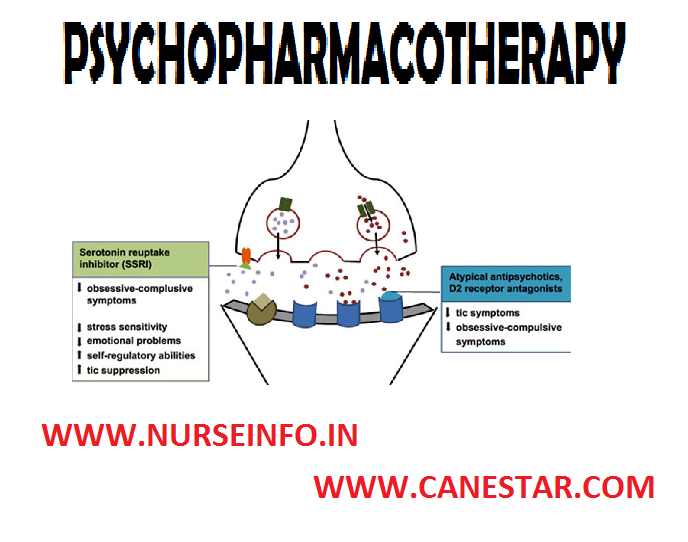
Psychopharmacologic
agents (also called psychotropic or psychotherapeutic medications) are to
relieve symptoms, but not “cure mental illness”. Clients taking psychotropic
medications and their families need education regarding the medications action,
purpose, intended effects, side effects, toxic or dangerous effects, treatment
for side-effects and what to do about adverse or toxic effects. Non-adherence
must be managed; client may not remember to take psychotropic medications or
may refuse to take them at all or as prescribed. Medications may need to be
changed and/or dosage adjusted in accordance with drug effectiveness and client
response. Nurses must observe and document the client’s responses to and
beliefs about medications
PRINCIPLES
OF PSYCHOPHARMACOLOGIC THERAPY
Psychopharmacologic agents do not
“cure” mental illness
Clients require physical and
psychiatric assessments before psychotropic medication is prescribed for them
Clients hold various views about the
use of psychotropic medications; some of these views may bring about nonadherence
to medication treatment
Clients must give informed consent
prior to administration of psychotropic medication including an explanation of
risks versus benefits
Psychotropic medication has different
onsets of actions. Most medications (lithium, antidepressants) require daily
administration for one to several weeks before their intended effects are
evident; some medications (benzodiazepines, antipsychotics) act more
immediately
PURPOSES OF PSYCHOPHARMACOTHERAPY
Relieve or reduce symptoms of dysfunctional
thoughts, moods, or actions, mental illness or disorder
Improve client’s functioning
Increase client’s adherence (or
compliance) and amenability to other therapies. Most psychotropic medications
act by modulating neurotransmitters (brain chemicals), specifically serotonin,
norepinephrine (noradrenaline), dopamine, acetylcholine and glutamate
REASONS FOR NON-COMPLIANCE TO PSYCHOTROPIC REGIMEN
Medications may be expensive and the
client cannot afford them
Clients may refuse to take
medications because of their unpleasant or distressing side-effects
Clients may stop taking their
medications because they begin to feel better and believe that they no longer
need the medications
Clients may not believe they have any
illness requiring medication or fear the stigma associated with having a mental
illness and taking medication
Mental illness itself such as
paranoia, contributes to the client’s denial or fears about medication usage
SERVICES THAT ENCOURAGE ADHERENCE TO MEDICATION REGIMEN
Follow up
interactions with the client will help the nurse verify that the client
understands the purpose, proper administration, intended effects, side and
toxic effects of, and how to treat serious problems associated with
psychotropic medications
Support persons can encourage and
assist the client’s adherence to his or her psychotropic medication regimen
Appropriate laboratory tests must be
conducted to prevent serious complications and assure safe and therapeutic
level of psychotropic medication
Medication groups often provide not
only education, but also peer support to those taking psychotropic medication.
Often clients and their families have misconceptions that are preventing the
client from taking his or her medication
Depot injections (injections of
medication into a body area where it will be deposited and stored) of
antipsychotic medication can provide two or four weeks dosage of the medication
to clients who have difficulty adhering to their medication schedule
EFFECTS ON SPECIAL POPULATIONS
Children:
psychotropic medications should be administered with great caution to children.
Initiating treatment with small dosages and increasing the dosages slowly
diminishes the likelihood of side effects. Although the small volume of
distribution suggests the use of lower doses than in adults, a child’s higher
rate of metabolism suggest that a higher ratio of mg of drug to Kg of body
weight should be used
Elderly: elderly
clients are more susceptible to side effects, especially cardiac effects and
may metabolize and excrete drugs more slowly
Lower doses are needed for the
elderly client because of decreased liver and renal function
Elderly clients are likely to be
taking other drugs; therefore, they have an increased risk for drug-drug
interactions
They may have decreased liver and
renal function, therefore, their BUN (Blood, Urea, Nitrogen), creatinine, and
liver enzymes should be monitored regularly
Regular use of sedating medications
for sleep should be discouraged because they usually return to normal sleeping
patterns after only a few nights of medication use
Discourage sedating medications as
they may cause excessive sedation, confusion or disorientation resulting in
falls and other injuries
Pregnancy:
the basic rule is to avoid administering any drug to a woman who is pregnant
(particularly during the first trimester) or who is breastfeeding a child. This
rule however, occasionally needs to be broken when the mother’s psychiatric
disorder is severe
BASIC PHARMACOLOGIC PRINCIPLES
Pharmacokinetics: it refers to the
movement of medication molecules in the body, including absorption,
distribution, metabolism and excretion of medications
Absorption: the movement of a
medication from its site of administration (e.g. GI tract, muscle, skin or
subcutaneous tissue) tissue to the bloodstream
Distribution: the transportation of a
medication to its site of action by bodily fluids
Metabolism: occurs primarily in the
liver. Individuals diagnosed with liver dysfunction have a increased ability to
metabolize medications and are at risk of undue accumulation of medication and
possible toxicity
Excretion: the elimination of a
medication from the body primarily through the kidneys. Individuals diagnosed
with renal dysfunction should be monitored for an increase in duration and
intensity of medication responses
Medication responses: plasma
medication levels can be regulated to control medication responses. Medication dosing
attempts to maintain plasma levels between the minimum effective concentration
(MEC) and the toxic concentration. When a medication has achieved plasma levels
that are effective and not toxic, the plasma level is within the therapeutic
range
Therapeutic index (TI): medications
with a high TI have a wide safety margin. Therefore, there is no need for
routine serum medication level monitoring. Medications with a low TI should
have serum medication level monitored closely. Monitor peak levels based on the
route of administration. For example, an oral medication may have a peak of 1
to 3 hours after administration. Whereas, if the medication is given
intravenously, the peak time might occur within 10 minutes
Half-life: the plasma half-life is
the time taken for the plasma concentration of the drug to decline to one-half
of its value
Pharmacodynamics (mechanism of
action): describes the interactions between medication and target cell, body
systems, and organs to produce effects. Medications interact with cells in one
or two ways. Medications can mimic the receptor activity regulated by
endogenous compounds or block normal receptor activity regulated by endogenous
compounds. For example, morphine is classified as an agonist because it
activates the receptors that produce analgesia, sedation, constipation and
other effects
KEY POINTS/KNOWLEDGE REQUIRED PRIOR TO MEDICATION ADMINISTRATION
Medication
category/class: medications may be organized according to pharmacologic action,
therapeutic use, body system, chemical make-up, and safe use during pregnancy
Mechanism of
action: this is how the medication produces the desired therapeutic effect
Therapeutic
effect: this is the primary action for which the medication is administered to
a specific client
Adverse
effects: these are any unintended or undesired effect that can occur at a
normal medication dose
Side
effects: there are secondary medication effects that occur at therapeutic
doses. These are usually predictable
Drug-drug
interaction: some medications may be given together to increase or decrease the
therapeutic effect. Two medications together may increase or decrease the
adverse side effects
Drug food
interaction: food may alter medication absorption and/or contain substances
that react with certain medications
Toxicity: an
adverse medication effect that is considered severe and may be life
threatening. It can be caused by an excessive dose, but can occur at
therapeutic dose levels
CONTRAINDICATION/PRECAUTIONS
A specific medication can be
contraindicated for a client based on the client’s condition. For example, a
patient with history of allergy to a particular medication
Precaution should be taken for a
client who is more likely to have an adverse reaction than another client. For
example, morphine depresses respiratory function, so it should be used with
caution for clients who have impaired respiratory function
Preparation, dosage and administration: It is important to know any
special consideration for preparation, recommended doses and how to administer
the medication
Nursing implications: know how to monitor therapeutic effects prevent and
treat adverse effects provide for comfort, and instruct clients in the safe use
of medications
SAFE MEDICATION ADMINISTRATION: THE SEVEN RIGHTS
Right client: verify the client’s
identification each time a medication is given check identification band, name
and/or photograph
Right drug: correctly interpret
medication order (verify completeness and clarity); read label three times;
when container is selected, when removing dose from container, and when
container is replaced; leave unit dose medication in its package until
administration
Right dose: calculate correct
medication dose; check drug reference to ensure dose is within usual range
Right time: give medication on time
to maintain consistent therapeutic blood level. It is generally acceptable to
give the medication ½ an hour before or after the scheduled time
Right route: select the correct
preparation for the ordered route. Know how to safely and correctly administer
medication
Right documentation: immediately
records pertinent information, including client’s responses to the medication
Right to refuse: clients have the
right to refuse to take a medication. Determine the reason for refusal, provide
information regarding risk for refusal, and notify appropriate health care
personnel and document refusal and action taken
PSYCHOPHARMACOTHERAPY – Principles of Psychopharmacologic Therapy, Purposes of Psychopharmacotherapy, Reasons for Non-compliance to Psychotropic Regimen, Services that Encourage Adherence to Medication Regimen, Effects on Special Populations and Safe Medication Administration: The Seven Rights (MENTAL HEALTH NURSING)
PSYCHIATRIC INVESTIGATION – Routine
Tests and Diagnostic Procedures used to Detect Altered Brain Function (Mental
Health Nursing)
The growing
awareness of various physical conditions which can produce psychiatric symptoms
and the increased use of biological therapies have made it mandatory that
appropriate physical investigations should be carried out before starting any
treatment and during it. They serve diagnostic, basal screening and monitoring
purposes
ROUTINE TESTS
A complete hemogram (total and
differential blood count, haemoglobin, ESR) and urinalysis are the basic
minimum of routine test. Leucopenia and agranulocytosis are associated with
certain medications. Treatment with lithium and neuroleptic malignant syndrome
are often associated with leukocytosis
Fasting and post-prandial blood
sugar, chest X-ray and an EEG are often considered routine tests
An EEG is necessary for monitoring
cardiac effects of certain drugs
Serum electrolytes (sodium, potassium
chlorides, bicarbonates, calcium, etc.) are sometimes needed as basal routine
investigations. An electrolyte imbalance causes various neuropsychiatric
symptoms like delirium
Liver function tests: serum glutamic
oxaloacetic transaminase (SGOT), serum glutamic-pyruvic transaminase (SGPT), serum
alkaline phosphatase, prothrombin time, serum bilirubin levels and serum
proteins (total and differential) are some common liver function tests. Liver
function tests are done for all alcoholic patients
Renal function tests: blood urea,
serum creatinine, and creatinine clearance, thyroid function tests (T3, T4 and
TSH) and ECG are routinely done on patients prior to starting lithium therapy
An ECG and chest X-ray are usually
done before a patient is posted for ECT
DIAGNOSTIC PROCEDURES used to DETECT ALTERED BRAIN FUNCTION
Several
diagnostic procedures are used to detect alternation in biologic function that
may contribute to psychiatric disorders
Electroencephalography
(EEG)
Technique:
electrodes are placed on the scalp in a standardized position. Amplitude and
frequency of beta, alpha, theta and delta brain waves are graphically recorded
on paper by ink markers for multiple areas of the brain surface
Purpose: it
measures brain electrical activity; identifies dysrhythmia, asymmetries, or
suppression of brain rhythms; used in the diagnosis of epilepsy, neoplasm
stroke, metabolic or degenerative disease
Computed
Tomography (CT)
Technique:
series of radiographs that are computer constructed into slices of the brain
that can be stacked by the computer giving a three-dimensional image
Purpose:
measures accuracy of brain structure to detect possible lesion, abscesses,
areas of infarction or aneurysm. CT has also identified various anatomic
differences in clients, with schizophrenia, organic mental disorder and bipolar
disorder
Magnetic
Resonance Imaging (MRI)
Technique: a
magnetic field surrounding the head induces brain tissue to emit radio waves
that are computerized to provide clear and detailed construction of sectional
images of the brain. No radiation or contrast
medium is used
Purpose: measures anatomic and biochemical status of various segments of
the brain; detects brain edema, ischemia, infection, neoplasm, trauma and other
changes such as demyelination. Morphological differences between the brains of
clients with schizophrenia and those of control subjects have been noted
Brain Electrical Activity Mapping (BEAM)
Technique: uses computed tomographic techniques to display data derived
from EEG recordings of brain electrical activity that can be sensory evoked by
specific stimuli, such as flash of light or a sudden sound, or cognitive evoked
by specific mental tasks
Purpose: measures brain electrical activity; used largely in research to
represent statistical relationship between individuals and groups or between
two populations of subject (e.g. client with schizophrenia vs. control
subjects)
Positron Emission Tomography (PET)
Technique: an injected radioactive substance travels to the brain and
shows up as a bright spot on the scan; different substances are taken up by the
brain in different amounts, depending on the type of tissues and the level of
activity
Purpose: measures specific brain functioning, such as glucose metabolism,
oxygen utilization, blood flow, and of particular interest in psychiatry
neurotransmitter/receptor interaction
Single Photon Emission Computed Tomography (SPECT)
Technique: the technique is similar to PET but a longer acting radioactive
substance must be used to allow time for a gamma camera to rotate about the
head and gather the data, which are then assembled on the computer into a brain
image
Purpose: measures various aspects of brain functioning as with PET; has also been used to image activity or cerebrospinal fluid circulation
PSYCHIATRIC INVESTIGATION – Routine Tests and Diagnostic Procedures used to Detect Altered Brain Function (Mental Health Nursing)
PERFORMING MENTAL STATUS EXAMINATION
– Definition, Purpose, General Instructions and Format for Mental Status
Examination (Mental Health Nursing)
DEFINITION
Mental
status examination (MSE) is an assessment of general motor behavior, thought
and emotional functioning, along with evaluation of insight and judgment of the
patient’s current status
PURPOSE
Mental status examination serves as a
basis for comparison, to track the progress of patient
It is used to detect changes or
abnormalities in a person’s psychological functioning
Perform a physical assessment from
head to toe including vital signs
Provide a comfortable environment for
mental status examination
Prepare some questions under each
aspect of mental status examination
FORMAT FOR MENTAL STATUS EXAMINATION
Instructions
Write observation findings obtained
from patient in the space given
Give details wherever required
Identification data
Name, b. age, c. sex, d. bed no, e.
data of MSE, f. time of MSE – date of admission, diagnosis:
General appearance
Consciousness, b. body built, c.
personal hygiene, d. grooming, e. facial expression, f. eye contact – well
built/moderately built/emaciated
Speech
Language, b. reaction time, c.
unusual words, d. volume, e. rate, f. characteristics
Motor activity
Level of activity, b. mannerisms, c.
type of activity
Mood of affect
Sad/happy/irritable/angry/suspicious/fearful/restless/worried/any
other (specify)
Perception
Hallucination: present/absent, if
present specify
Type:
visual/auditory/tactile/olfactory
Illusion: present /absent
Thought
Stream of thought: normal/increased/reduced/blocked/any
other, if present specify
Content: neologism/clang association,
if present specify
Form: circumstantiality/tangentiality/flight
of ideas, if present specify
Orientation
Oriented to time, place, person:
present/absent
Confusion: present/absent
Memory
Remote: intact/impaired
Recent: intact/impaired
Immediate: intact/impaired
Judgment
Logical/illogical (specify)
Attention
and concentration: good/distracted/pre-occupied/any other
Intelligence
Educational status,
b. learning disability:
present/absent, if present specify
I.Q. level
General knowledge
Insight:
present/absent
Psychological
factors
Stressor: present/absent, if present
specify
Coping skills (specify)
Social relation: good/poor
Occupation
Physiological
factors
Bowel and bladder habits
Appetite
Sleep
Libido
Summary
List of problems
PERFORMING MENTAL STATUS EXAMINATION – Definition, Purpose, General Instructions and Format for Mental Status Examination (Mental Health Nursing)
NURSING MANAGEMENT OF STRESS –
Nursing Interventions in Stress Management (MENTAL HEALTH NURSING)
The client
faces an array of potential stressors, or demands that can have health
consequences. The nurse needs to be aware of the situations that are likely to
result in stress and also must assess the client’s appraisal of the situations.
The major areas that provide the nurse with useful guide in the assessment
process include demands, human response to stressors and coping. It is always
better to observe the following indices of stress, in which some are
psychologic some are physiologic, some behavioral and some reflect social
behavior and thought process
Some of
these reactions may be coping behaviors
General irritability, hyperexcitation
or depression
Dryness of the throat and mouth
Overpowering urge to cry or run and
hide
Easily fatigued, loss of interest
Floating anxiety – do not know what
or why
Easily started
Stuttering or other speech
difficulties
Hypermobility, pacing, moving about,
cannot look still
GI symptoms – butterflies in the
stomach, diarrhea, vomiting
Change in menstrual cycle
Loss or excessive appetite
Increased use of legally prescribed
drugs, e.g. tranquilizers
Accident proneness
Disturbed behavior
Pounding of the heart
Impulsive behavior, emotional
instability
Inability to concentrate
Feelings of unreality, weakness or
dizziness
Tension, alertness
Nervous laughter
Grinding of teeth
Insomnia
Perspiring
Increased frequency of urination
Muscle tension and migraine, headache
Pain in the neck, and lower back
Increased smoking
Alcohol and drug addiction
Nightmares
The probable
nursing diagnosis in coping-tolerance pattern will be as follows:
The first
step in managing stress is to become aware of its presence. This includes
identifying and expressing stressful feelings (as stated above). The role of
the nurse is to facilitate and enhance the coping and adaptation. Nursing
interventions depend on the severity of the stress experience and demand. The
nurse’s efforts are directed to life-supporting interventions and to the
occlusion of approaches aimed at the reduction of additional stressors to the
client
The
importance of cognitive appraisal in the stress experience should prompt the
nurse to assess if changes in the way the client perceives and label particular
events or situations (cognitive reappraisal) are possible. So the nurse should
also consider the positive effects that result from successfully meeting and
stressful demands. Greater emphasis should also be placed on the part of
cultural values and beliefs enhancing or constraining various coping options
An
individual personal resource that aids in coping includes health and energy. A health-promoting
lifestyle provides these resources and buffers or cushions the impact of
stressors. Lifestyle or habits that contributed to the risk of developing
illness can be reduced or eliminated. Health risk appraisal is an assessment
method designed to promote health by examining the individual personal habits
and recommending change where health risk is identified. For example, smoking
causes lung cancer and can be prevented by reducing or leaving the habit of
smoking
Coping
enhancement: coping enhancement is a nursing intervention and defined as
“assisting a patient to adapt to perceived stressors, changes, or threats which
interfere with meeting life demands and roles”. After completing a health risk
approach, the nurse could use “coping enhancement to assist the patient in an
analysis of the appraisal and to explore methods to improve the person’s coping
abilities including appraisal of his or her own personal resources
The
activities of coping enhancement are as follows:
Appraise the patient’s adjustment to
change in body image as indicated
Appraise the impact of the patient’s
life situations on roles and relationships
Encourage the patient to identify a
realistic description of change in role
Approve the patient’s understanding
of the disease process
Approve and discuss alternative
responses to situation
Use a calm reassuring approach
Provide an atmosphere of acceptance
Assist patient in developing an
objective appraisal of an event
Help the client to identify the
information he/she made interested in obtaining
Provide factual information
concerning diagnosis, treatment and prognosis
Provide the patient with realistic
choices about certain aspects of care
Encourage an attitude to realistic
hope as a way of dealings with feelings of helplessness
Evaluate patient’s decision-making
ability
Seek to understand the patient’s
perspective of a stressful situation
Discourage decision-making when
patient is under severe stress
Encourage gradual mastery of the
situation
Encourage patience in developing relationships
Encourage relationships with persons
who have common interests and goals
Encourage social and community
activities
Encourage the acceptance of
limitation of others
Acknowledge the patient’s
spiritual/cultural background
Encourage the use of spiritual
resources if desired
Explore the patient’s previous
achievement of success
Explore patient’s reason for
self-criticism
Confront patient’s ambivalent (anger
or depression) feelings
Foster constructive outlets of anger
and hostility
Arrange situations that encourage
patient’s autonomy
Assist patient in identifying
positive responses from others
Encourage the identification of
specific life values
Explore with the patient previous
methods of dealing with life problems
Introduce the patient to persons (or
group) who have successfully undergone the same experience
Support the use of appropriate
defense mechanisms
Encourage verbalization of feelings,
perceptions and fears
Discuss consequences not dealing with
guilt and shame
Encourage the patient to identify own
strength and abilities
Assist patient in identifying
appropriate short and long-term goals
Assist the patient in breaking down
complex goals into manageable steps
Assist the patient in examining
available resources to meet the goal
Reduce stimuli in the environment
that could be misinterpreted as threatening
Appraise patient’s needs/desires for
social support
Assist the patient to identify
available support systems
Determine the risk of the patient’s
inflicting self-harm
Encourage family involvement as
appropriate as possible
Encourage the family verbalize
feelings about ill family member
Provide appropriate social skills
training
Assist the patient to solve problem
in a constructive manner
Instruct the patient about the use of
relaxation techniques as needed
Assist the patient to grieve, and
work through the losses of chronic illness and/or disability if appropriate
Assist the patient to clarify
misconceptions
Encourage the patient to evaluate
his/her own behavior
NURSING MANAGEMENT OF STRESS – Nursing Interventions in Stress Management (MENTAL HEALTH NURSING)
INDIVIDUAL PSYCHOTHERAPY – Levels of
Individual Therapy (MENTAL HEALTH NURSING)
Psychotherapy
is the use of techniques that facilitates or allows people to modify their
feelings, attitudes and behaviors. Individual psychotherapy focuses on the
needs and problems of the client. In therapy two people come together in an
encounter that is specifically designed for the purposes of relieving emotional
pain, treating mental illness and facilitating change and growth. In a therapy
situation one person is designated as the therapist (the facilitating or
helping person) and the other is called client (the person seeking help). As
individual psychotherapy develops the client and therapist will discuss some
historical information, current challenges, pass successes, feelings, needs and
goals. Because of their objectivity and specialized knowledge, therapists
generally can be more effective than family or friends in facilitating the
client’s with challenges and growth
LEVELS OF INDIVIDUAL THERAPY
Supportive:
the client is provided a caring, safe relationship in which to explore problems
and make decisions. The therapist reinforces client’s existing coping skills
and does not attempt to teach him/her new coping methods
Re-educative:
the client explores new ways to perceive and behave through a systematic
approach. The client and therapist sign a contract that identifies goals and
desired changes in behaviors and feelings. An effective approach is reality
based focused on solutions and directly deals with concrete issues. Examples
include cognitive restructuring and behavior modification
Reconstructive: the client may spend two to five years exploring all aspects of his/her life through analysis or deep psychotherapy. Outcomes include self-understanding and understanding of others greater emotional freedom, maximizing one’s potential, and a greater capacity for love and work
INDIVIDUAL PSYCHOTHERAPY – Levels of Individual Therapy (MENTAL HEALTH NURSING)
GROUP THERAPY – Types of Therapy,
Physical Conditions that Influence Group Dynamics and Curative/Therapeutic
Factors of Group Therapy (According to Yalom) (MENTAL HEALTH NURSING)
The goal of
group therapy is to help individuals develop more functional and satisfying
relationships. When an individual’s dysfunctional pattern is demonstrated in
the group, the task of the group is to assist members to understand the
patterns of interacting within the group and to help clients generalize this
information to their lives outside the group
TYPES OF GROUP
Task groups: a group formed to
accomplish a specific outcome
Teaching groups: focus is to convey
knowledge and information to a number of individuals
Supportive/therapeutic groups: the
concern of these groups is to prevent possible future upsets by educating the
participants in effective ways of dealing with emotional stress arising from
situational or developmental crises
Self-help groups: composed of
individuals with a similar problem
PHYSICAL CONDITIONS THAT INFLUENCE GROUP DYNAMICS
Seating: it
is best when there is no barrier between the members. For example, a circle of
chairs is better than chairs set around a table
Size: seven or
eight members provide a favorable climate for optimal group interaction and
relationship development
Membership:
two types of groups exist: open ended groups (those in which members leave and
others join at any time during the existence of the group) and closed ended
groups (those in which all members join at the time the group is organized and
terminated at the end of the designated length of time)
CURATIVE/THERAPEUTIC FACTORS OF GROUP THERAPY (ACCORDING TO YALOM)
Instillation of hope: client believes
he/she will get better through groups therapy
Universality: client learns that
other group members have similar problems and feelings
Imparting of information: client
learns didactic information which occurs in a group setting
Altruism: client help each other in
the group, resulting in increased self-esteem
Corrective recapitulation of the primary family group: client’s family
background influences client behavior and client can relieve and correct early
conflicts
Development of socializing techniques:
client develops social skills in the group
Initiative behavior: client
identifies with and imitates healthy behavior of group members
Interpersonal learning: client’s
interpersonal distortions are connected
Group cohesiveness: client
experiences bonding with the group, group norms are protected and positive
client outcomes result
Catharsis: group members express
feelings, even deep and powerful emotions, and then learn new ways to handle
their problems
Existential factors: responsibility,
existence, awareness, and mortality are explored
GROUP THERAPY – Types of Therapy, Physical Conditions that Influence Group Dynamics and Curative/Therapeutic Factors of Group Therapy (According to Yalom) (MENTAL HEALTH NURSING)
DISCHARGE – Discharge of Voluntary
Patient, Order of Discharge on the Undertaking of Relatives or Friends, etc,
for Due Care of Mentally ill Person (Mental Health Nursing)
Discharge
planning begins when the client is admitted, whether it is the hospital, home
care, or any other treatment program. The client, and when appropriate, the
family must be involved in this process for it to be successful
The patient who
is voluntarily admitted to the hospital can leave at any time. The voluntarily
admitted patient can be discharged by the staff when maximum benefit has been
received from the treatment. Voluntary patients also may request discharge. Two
key factors in deciding to release a voluntary psychiatric patient are:
Assessment of the patient’s
competency
Assessment of the patient’s potential
danger to self or others
An
involuntarily admitted patient has lost the right to leave the hospital when he
or she wishes. If a committed patient leaves before discharge, the staff has
the legal obligation to notify the police and courts
DISCHARGE OF VOLUNTARY PATIENT
Patients
admitted on voluntary basis, is they request for discharge are obliged to be
discharged by the medical officer in charge within 24 hours of receiving the
request, provided the medical officer is convinced that the discharge will not
harm the interest of the voluntary patient. In such case, the medical officer
would constitute a board of two medical officers and seek their opinion. If the
board is of the opinion that such voluntary patient needs further treatment in
the psychiatric hospital/psychiatric nursing home, the medical officer shall
not discharge the voluntary patient but continue his treatment for a period not
exceeding 90 days at a time
ORDER OF DISCHARGE ON THE UNDERTAKING OF RELATIVES OR FRIENDS, ETC. FOR DUE CARE OF MENTALLY ILL PERSON
Where any relative or friend of a
mentally ill person detained in a psychiatric hospital or psychiatric nursing
home under section 22, 24 or 25 desires that such person shall be delivered
over to his care and custody, he may make an application to the medical officer
in charge
Where an application is received, the
authority shall, on such relative or friend furnishing a bond, with or without
sureties for such amount as such authority may specify in this behalf,
undertaking to take proper care of such mentally ill person, and ensuring that
the mentally ill person shall be prevented from causing injury to himself or to
others, make an order of discharge and thereupon the mentally ill person shall
be discharged
DISCHARGE OF PERSON SUBSEQUENTLY FOUND ON INQUISITION TO BE OF SOUND MIND
If any
person detained in a psychiatric hospital or nursing home in pursuance of a
reception order made under this Act is subsequently found, on an inquisition,
to be of sound mind is capable of taking care of himself and managing his
affairs the medical officer in charge shall forthwith on the production of a
copy of such finding duly certified by the District Court, discharge such
person from such hospital or nursing home
Apart from
Admission and Discharge detailed procedures have been laid down under various
sections of the MHA for (to mention a few)
Being taken into custody by the
police, confinement and security of mentally ill persons or prisoners in a
mental hospital
Ensuring proper care and custody to a
mentally ill person by his legal relatives, through the police stations
For safety in hospital or during
leave or absence or transfer to another hospital
Safe custody and protection of
property of the patient. Physical or mental cruelty to mentally ill patients is
forbidden. Similarly, conduct of research on a mentally ill patient is
forbidden, unless voluntarily consent from patient or relative is obtained. The
human rights of a mentally ill person are protected penalties and fines for
contravening the provisions of the Act have been discussed in various sections
of the MHA
DISCHARGE – Discharge of Voluntary Patient, Order of Discharge on the Undertaking of Relatives or Friends, etc, for Due Care of Mentally ill Person (Mental Health Nursing)