INFANT CARE – Physiological
Developments and Role of Nurse in Infant Care (CHILD HEALTH NURSING)
Infant
growth and development is rapid and enables maturation to unfold in a
relatively short time. Health status is based on the infant’s ability to adapt
to these rapid changes. As healthcare providers, the nurse must have an
understanding of these changes to ensure the infant and his or her family
maintains an optimal health
PHYSIOLOGICAL DEVELOPMENTS
Height and
weight: height increases during the first 6 months by approximately one inch
per month. The rate of growth in height slows to approximately 0.5 inches per
month by 12 months of age. The weight gains 1.5 lb per month or 5-7 oz per
week. By 12 months of age, the infant’s birth weight will have tripled
Head growth:
the size of the head changes rapidly during infancy, reflecting rapid brain
growth. By the age of 12 months the infant’s brain will be two thirds the size
of a adult brain. During first 6 months the head circumference will increase by
approximately 0.5 inches per month
Motor
development: motor development is related to physical, cognitive, and social
development, which provides the infant with the means and freedom to explore
the environment. Gross motor development is the ability to use large muscle
groups to maintain balance and postural control or locomotion. Fine motor
development is the ability to coordinate hand-eye movement in an orderly and
progressive manner
Health
screening: health screening provides the opportunity to assess for detect any
problems, the infant may have and includes test to detect phenylketouria (PKU),
iron deficiency anemia, lead poisoning and hypothyroidism. The infant’s health
screening actually begins immediately after birth with the Apgar scoring and
physical examination. The screening visits typically include health assessment,
physical examination, growth indicators, anticipatory guidance, parental
concerns and administration of scheduled immunizations
A ROLE OF A NURSE IN INFANT CARE
The
community health nurse can be instrumental in providing information related to
development, nutrition, elimination, hygiene, safety, immunization and play.
The nurse should provide information about possible reactions the infant might
experience after receiving the immunizations
Feeding of
infants: a child who is on breastfed has greater chances of survival than a
child artificially fed. Prolonged breastfeeding does protect the infant from
early malnutrition and some infections. Artificial feeding given the babies
suffer with prolonged illness or death of the mother
Weaning is not sudden withdrawal of child from the breastfed. It is a gradual process starting around the age of 4-5 months because the mother’s milk alone is not sufficient to sustain growth beyond 4-5 months. It should be supplemented by suitable foods rich in protein and other nutrients. The community health nurse should clearly explain to the mother and family
INFANT CARE – Physiological Developments and Role of Nurse in Infant Care (CHILD HEALTH NURSING)
GROWTH CHART – Uses of Growth Chart,
Alternative Methods of Growth Monitoring and Child Health Problems (CHILD
HEALTH NURSING)
The growth
chart or ‘road to health chart first designed by David Morley and later
modified by WHO. It is visible display of the child’s physical growth and
development. It is designed primarily for the longitudinal follow up of a child
USES OF GROWTH CHART
Growth monitoring which is of great
value in child health care
It is used as diagnostic tool for
identifying “high risk children”
It helps planning and policy making
in relation to child health care at the local and central levels
Educational tool for the mother to
participate more actively in growth monitoring
It helps the health worker on the
type of intervention that is needed. It will help to make referrals easier.
It provides a good method to evaluate
the impact of a program or of special interventions for improving child growth
and development
It is used as tool for teaching, for
example, the importance of adequate feeding
ALTERNATIVE METHODS OF GROWTH MONITORING
The growth
chart or road to health chart is described as a passport to child healthcare.
The road to health chart helps to identify “at a glance”. It also provided on
the card to record important events such as immunization, birth history and if
any treatment given. Growth charting is only one method of growth monitoring;
there are other indications such as height for age, weight for height and arm
circumference
CHILD HEALTH PROBLEMS
Low birth
weight: International agreement of low birth weight has been defined as birth
weight of less than 2.5kg. the measurement being taken preferably within the
first hour of life, before significant postnatal weight loss has occurred.
There are two main groups of low birth weight babies those born prematurely
(short gestation) and those with fetal growth retardation
Malnutrition:
malnutrition makes the child more susceptible to infection. Undernourished
children do not grow to their full potential of physical and mental abilities.
Malnutrition in infancy and childhood leads to stunted growth. Micronutrient
malnutrition refers to a group of condition caused by deficiency of essential
vitamins and minerals
Infectious
and parasitic disease: the leading childhood diseases are diarrhea, respiratory
infections, measles, pertussis, polio, neonatal tetanus, tuberculosis, and
diphtheria. Parasitic diseases such as eruptive fevers, poliomyelitis, malaria,
intestinal parasites such as ascariasis, hook worm giardiasis and amoebiasis,
etc. which are common because of poor environmental sanitation and paucity of
portable drinking water
Accidents
and poisoning: children and young adolescents are particularly vulnerable to
domestic accidents including falls, burns, poisoning and drowning. Accidents
among children are home accidents and traffic accidents
Other factors affecting child health: child health is affected by various factors – behavioral problems, maternal health, family environment, socioeconomic circumstances, environment and social support and health care
GROWTH CHART – Uses of Growth Chart, Alternative Methods of Growth Monitoring and Child Health Problems (CHILD HEALTH NURSING)
BABY-FRIENDLY HOSPITAL –
Introduction, Steps in Global BFHI, Objectives of BFHI, Guidelines for
Successful Lactation and International Act (CHILD HEALTH NURSING)
INTRODUCTION
Baby-friendly hospital is a movement
under which breastfeeding is protected and encouraged
Baby-friendly hospital initiative
(BFHI) was launched in 1922 as part of the Innocenti Declaration on promotion,
protection and support of breastfeeding by WHO and UNICEF
BFHI is a global programs organized
by UNICEF, after the introduction in 1922, exclusive demand feeding is accepted
as the only mode of early infant feeding
BFHI plus program incorporates other
child survival and safe motherhood components like immunizations, antenatal
care, oral rehydration therapy, ARI control programs
STEPS IN GLOBAL BFHI
A written breastfeeding policy that
is routinely communicate to all healthcare staff
Training of all cares staff in
skilled necessary to implement this policy
Informing all pregnant women about
the benefits and management of breastfeeding
Helping mothers initiative
breastfeeding within a half hour of birth
Showing mothers how to breastfeed and
how to maintain lactation, even if they should be separated from their infants
Giving newborn infants – no food or
drink other than breast milk
In practicing room, allow mother and
infants to remain together for 24 hours a day
Encouraging breastfeeding on demand
Giving no artificial teats or
pacifiers
Fostering the establishment of
breastfeeding support groups and refer mothers to them on discharge from
hospital or clinic
OBJECTIVES OF BFHI
International
pediatric association conference objectives:
To enable mother to make an informed
choice about how to feed their babies
To support early initiation of breast
feeding
To promote exclusive breast feeding
for the first 4-6 months
To discourage commercial infant milk
substitutes being supplied free to hospital
GUIDELINES FOR SUCCESSFUL LACTATION
Before starting breastfeeding mother
should sit in a comfortable position
Rooming in, bedding in allows the
mother to identify cues and feed immediately
Start feeding the baby before gets
angry or hungry
Wait until mouth is wide open and
move him quickly from below the nipple
Offer the breast in such a way that
the areola is almost inside the baby’s mouth
Hold infant close-facing the breast’s
with chest-to-chest, abdomen-to-abdomen, head and body of infant aligned
Allow him to suckle at one breast for
10-15 min or more. If the infant is still hungry switch on the other breast.
For the next feed start from breast which was fed last
Encourage demand feeding that to
every 2-3 hours, even more frequently if infant desires
End the feed by introducing a finger
in between corner of mouth of the infant and breast tissue to break the suction
to avoid injuring the nipples
Place the baby in right lateral
position
Educate mother that they are feed
their babies when they and their babies have the following illnesses like
vomiting, cough, fever, diarrhea and cold, etc
The importance of support from family
members plays a key role successful continuation of exclusive breastfeeding
INTERNATIONAL ACT
International
code of marketing of breast milk substitute (the code) was adopted by the World
Health Assembly (WHA). The code set out simple, basic rule to regulate harmful
marketing practice
No advertising of breast milk
substitutes feeding bottles and teats
No free samples to mothers
No promotion in healthcare facilities,
including no free or low cost formula
No company personnel to contact
mother
No gifts or personal samples to
health workers
No pictures of infants or words
idealizing artificial feeding on the labels of the products
Information to health workers should
be scientific and factual
Information on artificial feeding,
including that on labels, should explain the benefits and superiority of
breastfeeding and the associated with artificial feeding
BABY-FRIENDLY HOSPITAL – Introduction, Steps in Global BFHI, Objectives of BFHI, Guidelines for Successful Lactation and International Act (CHILD HEALTH NURSING)
ULTRASOUND IN OBSTETRICS – ULTRASOUND
WORKING, USE OF ULTRASOUND IN OBSTETRICS, TRANSVAGINAL ULTRASONOGRAPHY, DOPPLER
ULTRASOUND AND MIDWIFE’S RESPONSIBILITY REGARDING PRENATAL SCREENING (Maternal
and Child Health Nursing)
The
ultrasound is a sound wave beyond the audible range of frequency greater than 2
MHz cycles per second). The commonly used frequency range in obstetrics is
3.5-5 MHz. SONAR stands for “Sound,
Navigation and Ranging”. In clinical practice, two main varieties of ultrasound
(sound that is produced at a very high pitch) are used depending upon whether
the reflected waves give audible or visual signals
The apparatus, which interprets the
audible signals – doptone and sonicaid are easy to carry and simple to use even
with batteries. It can detect fetal heartbeats are early as 10 week of
gestation
The apparatus for interpretation of
visible signals – the sonar system, which is a much more sophisticated and
bulky apparatus, issued in three forms
The A-scan, that gives a one-dimensional picture
The B-scan, that gives a composite two-dimensional picture
The real-time scanner that depicts movements – to display cardiac and
breathing activity
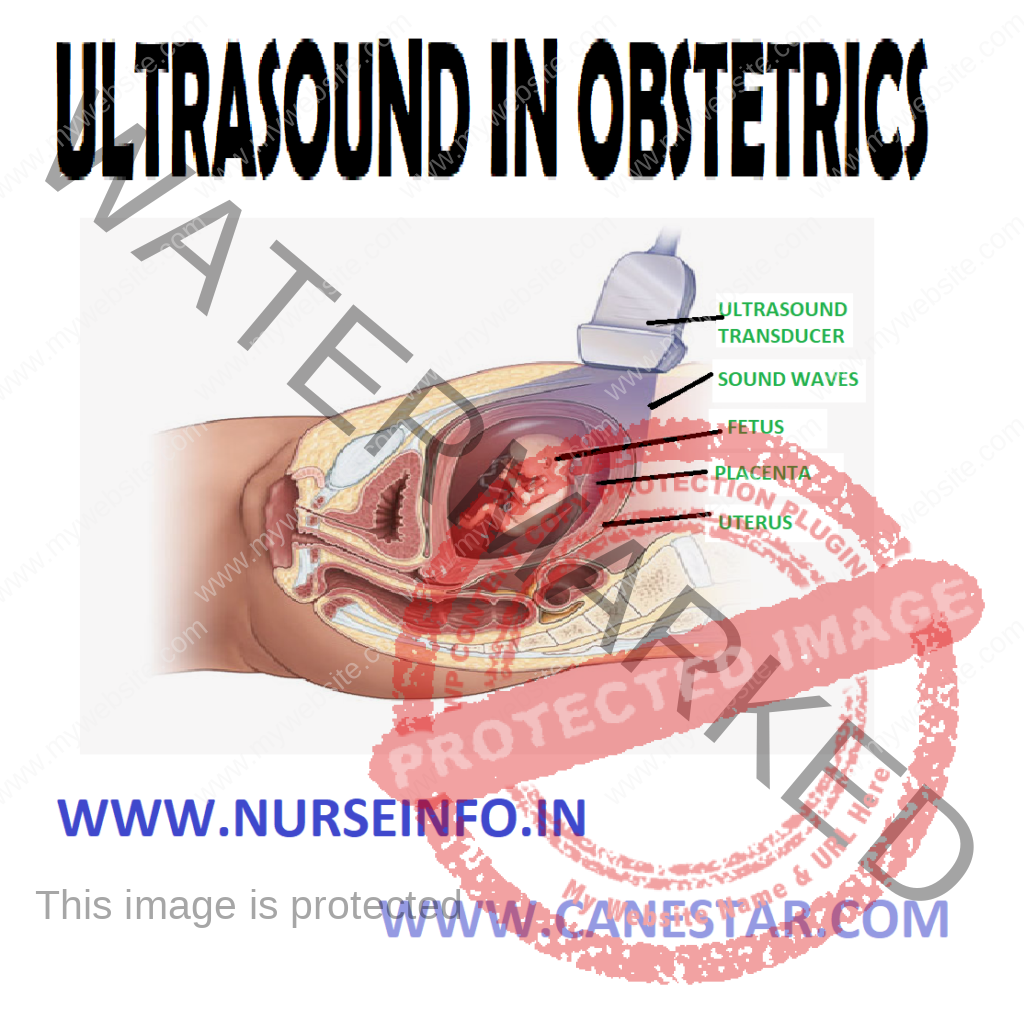
HOW DOES ULTRASOUND WORK?
Scanners are
used to produce static pictures. The picture is built up as a single crystal
transducer (a thin disk to which a wire is attached) is moved backward and
forward across the area scanned. When the transducer is placed on the body and
as it encounters a structure, a fraction of that sound is reflected back. The
echo is detected electronically and transmitted on to the screen as dots. The
amount of sound from the each organ varies according to the type of tissue
encountered:
Strong echoes give bright dots, e.g.
bone
Weaker echoes give various shades of
gray according to their strength
Fluid-filled areas cause no reflexion
and give rise to a black image
The
real-time scanners are so called because it produces a moving picture on the
screen as opposed to scanner that gives static picture. The real-time scanner
can have several types of transducers attached to it, which are interchangeable
and are used according to the type of image needed and the part of the anatomy
to be examined. Types of transducers in common use include the linear array,
the curved linear array, the sector and the vaginal probe. Instead of a single
crystal, all these types of transducers have many crystals that fire off
electrical energy and collect the echoes very rapidly, thus producing the
moving picture.
USE OF ULTRASOUND IN OBSTETRICS
Sonography
is a noninvasive procedure and has been proved safe to the conceptus, even with
repeated exposures at any stage of pregnancy.
Routine sonography in early months is used for:
Diagnosis of pregnancy: detects
gestational ring at 5th week, fetal poles and gestational sac at 6th
week, cardiac pulsation at 7th week and embryonic movements at 8th
week of gestation
Detection of abnormal conceptus prior
to clinical manifestations, and fetal malformations
Accurate determination of gestational
age is possible, which is helpful later in pregnancy when IUGR is suspected.
For this, crown-rump length (CRL) at 10-11 weeks gives the best predictive
value
Diagnosis of twins can be made early
in pregnancy for effective management
To diagnose unsuspected placenta
previa: because of the possibility of placental migration to the upper segment,
repeat scanning should be performed later-around 34th week
Selective
sonography is done when indicated at any time during pregnancy for the
following reasons:
To determine the maturity of the
fetus: crown-rump length (CRL), biparietal diameter (BDP) and femur length (FL)
are the measurements of choice for assessment of gestational age. Determination
of the maturity is important in cases of:
Uncertainty gestational age
Discrepancy between amenorrhea and uterine size
Prior to elective induction of postmaturity or elective cesarean section
Suspicion of
fetal and/or placental abnormalities such as:
Suspected
ectopic pregnancy
Blighted
ovum (empty sac)
Incomplete
abortion
Hydatidiform
mole
Localization
of placenta as in placenta previa
Abruptio
placentae
Intrauterine
growth retardation
Intrauterine
death
Malpresentations,
such as breech, transverse or face
Structural
defects, such as neural tube defects, absent or abnormal limbs
Defects of
gastrointestinal and urinary system and heart defects
Prior to invasive procedures such as
chorion villus biopsy, amniocentesis, cordocentesis, photocopy and intrauterine
fetal therapy
As a part of antepartum or
intrapartum fetal surveillance a biophysical profile
Integrity of a previous cesarean scar
– a weak scar or placental implantation over the scar can be detected
Postpartum period
Secondary PPH
Retained placental bits
Subinvolution due to fibromyoma
Neonatal head screening to diagnose:
Intraventricular hemorrhage
Hydrocephalus
TRANSVAGINAL ULTRASONOGRAPHY
Transvaginal
ultrasonography (TUS) is usually done during the first trimester of pregnancy.
As the transducer is closer to the object, the images are of enhanced quality.
A full bladder is not required. Transvaginal sonography is superior to
transabdominal sonography in diagnosing placenta previa
DOPPLER ULTRASOUND (AUDIBLE SIGNAL)
Ultrasound
transmitted into the body in a narrow beam is transferred back at the same
frequency when the object is still. When moving, there is a change in frequency
known as the Doppler shift. The frequency increases or decreases according to
whether the movement is toward or away from the source of energy
It is used
for monitoring the fetal heart rate, which can be picked up as early as 10th
week of gestation. Uterine and fetal blood flow can be assessed and the fetus
at risk of compromise could be identified. Leg vein thrombosis can be diagnosed
by noting the absence of hissing sound of blood flow through the veins
Midwives
take care of pregnant women in different stages of their pregnancy. They often
need to involve themselves in preparing and counseling women through the
process. When giving information about the screening tests available or
prescribed, it is important to include information regarding;
Why the test is offered
What the test involves and
When and how the results will be
given
In order to
advise women regarding the tests that are available, the midwife needs to keep
up-to-date with current technological advances
Information given to women should also include how the woman needs to prepare herself, e.g. by attending with a full bladder for a scan
ULTRASOUND IN OBSTETRICS – ULTRASOUND WORKING, USE OF ULTRASOUND IN OBSTETRICS, TRANSVAGINAL ULTRASONOGRAPHY, DOPPLER ULTRASOUND AND MIDWIFE’S RESPONSIBILITY REGARDING PRENATAL SCREENING (Maternal and Child Health Nursing)
POSTNATAL CARE – Objectives of
Postpartum Care, Postpartum Examination, Postnatal Assessment, Postnatal Care
and Attention, Complications of Postnatal Period and Role of Nurse in Postnatal
Care (MATERNAL AND CHILD HEALTH NURSING)
Care of the
mother after delivery is known as postnatal or postpartum care or puerperium.
Puerperium is a 6-week period following birth in which the reproductive organs
undergo physical and physiological changes – a process called involution
OBJECTIVES OF POSTPARTUM CARE
To prevent complications of
postpartum period
To provide care for the rapid
restoration of the mother
To provide family planning services
To check adequacy of breastfeeding
To provide basic health education to
mother/family
POSTPARTUM EXAMINATION
Examining
postpartum mother to rule out any fever, tachycardia, laceration and erosion of
cervix, rectocele, cystocele, displacement of uterus and inflammatory swellings
in the abdomen, examining the neonates to rule out birth injuries, congenital
defects and low-birth weight
POSTNATAL ASSESSMENT
It is to
Assessing weight changes of the neonates and the nature and extent of birth
injuries and congenital defects. Assessing the temperature and pulse rate of
the mothers
POSTNATAL CARE AND ATTENTION
Provide for
the care of the perineum, care of the breast, prevention of infection, early
ambulation, immunization and psychological support to mothers. It is also
provided for prevention of infection and care of the cord stump of new born.
Postnatal education and counseling includes breat-feeding, dietary intake,
danger signals, and family planning
COMPLICATIONS OF POSTNATAL PERIOD
Puerperal sepsis: this is infection of the
genital tract within 3 weeks after delivery. This is accompanied by rise in
temperature and pulse rate, foul smelling lochia, pain and tenderness in lower
abdomen, etc. this can be prevented by attention to asepsis before and after
delivery
Thrombophlebitis: this is an
infection of the vein of the legs, frequently associated with varicose vein.
The leg may become tender, pale, and swollen
Secondary hemorrhage: bleeding from
vagina anytime from 6 hours after delivery to the end of puerperium (6 weeks)
is called secondary hemorrhage and may be due to retained placenta or membranes
Others: urinary tract infection and
mastitis, etc
ROLE OF NURSE IN POSTNATAL CARE
Care during postpartum period to the
mother-enquire and observe her condition generally and with reference to sleep,
diet, after the pain subsides. Check vital signs, inspect perineum for
discharge and inspect breast and nipples
Care of newborn is an interwoven
activity along with the care to mother. It involves taking body temperature,
checking skin, color, eyes, bowel movements, urination, watching the cry,
checking the sleeping and feeding
POSTNATAL CARE – Objectives of Postpartum Care, Postpartum Examination, Postnatal Assessment, Postnatal Care and Attention, Complications of Postnatal Period and Role of Nurse in Postnatal Care (MATERNAL AND CHILD HEALTH NURSING)
MEASUREMENT OF FUNDAL HEIGHT –
Methods and Procedures (MATERNAL AND CHILD HEALTH NURSING)
METHOD AND PROCEDURES
Ask the woman to completely empty her
bladder immediately before proceeding with the abdominal examination. This is
important as even a half full bladder might result in an increase in the fundal
weight
Ask the woman to lie on her back with
the upper part of her body supported by cushions. Never make a pregnant woman
lie flat on her back as the heavy uterus may compress the main blood vessels
returning to the heart and cause fainting (supine hypotension). Ask her to
partially flex her hips and knees
Stand on the right side of the woman
to examine her in a systematic manner
The attention of the woman may be
diverted by conversation
Your hand must be warm and should be
placed on the abdomen till the uterus is relaxed before the palpation is
actually begun. Poking the abdomen with the fingertips should be avoided at all
costs
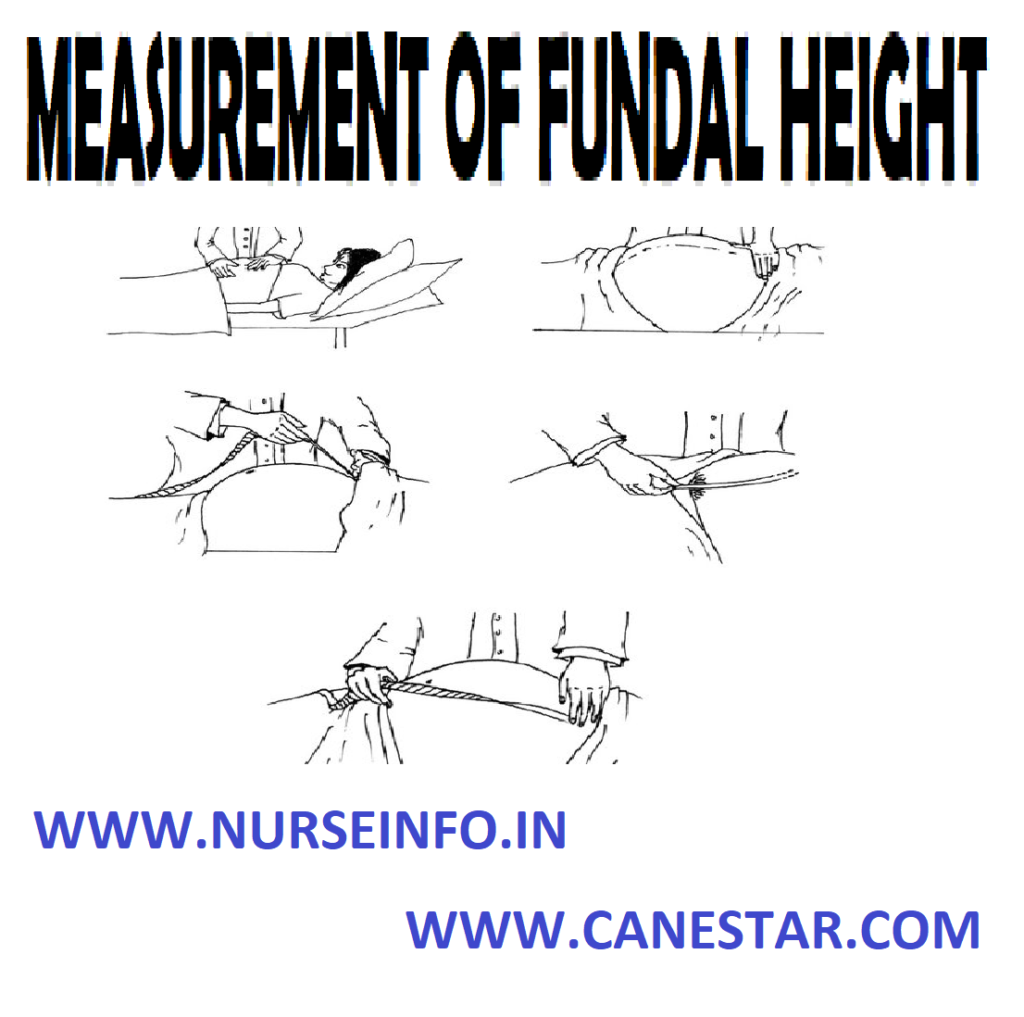
To measure the fundal height, place
the ulnar (medial/inner) border of the hand on the woman’s abdomen, parallel to
the symphysis pubis. Start from the xiphisternum (the lower end of the
sternum/breastbone), and gradually proceed downwards towards the symphysis
pubis, lifting you hand between each step down, till your finally feel a
bulge/resistance, which is the uterine fundus
Mark the level of the fundus. Using a
measuring tape (a tailor’s tape measure which is made of non-stretchable
material), measure the distance (in cm) from the upper border of the symphysis
pubis to the top of the fundus. After 24 weeks of gestation, the fundal weight
(in cm) corresponds to the gestational age in weeks (within 1-2 cm deviation).
Remember, at the time of measuring the fundal height in cm, the legs of the
woman should be kept straight and not flexed
The supine position in late pregnancy
and labor has also been shown to be associated with higher fundal height
readings; therefore, this can give to false readings and an inaccurate estimate
of the gestational age. It is therefore, recommended that the woman lies down
in a half-lying position when measuring the fundal height
When the same operator is measuring
the fundal height at each visit, this technique has been shown to have good
predictive values, especially for identifying major intrauterine growth
retardation (IUGR) and multiple pregnancies
The normal fundal height is different
at different weeks of pregnancy. To estimate the gestational age through the
fundal height, the abdomen is divided into parts by imaginary lines. The most
important one is the one passing through the umbilicus. Then divide the lower
abdomen (below the umbilicus) into 3 parts with 2 equidistant lines between the
symphysis pubis and the umbilicus. Similarly, divide the upper abdomen into three
parts, again with two imaginary equidistant lines, between the umbilicus and
the xiphisternum
Look where the fundal height is and
judge as given below:
At 12th week: just palpable above the symphysis pubis
At 16th week: lower one-third of the distance between the
symphysis pubis and umbilicus
At 20th week: two-thirds of the distance between the symphysis
pubis and umbilicus
At 24th week: at the level of the umbilicus
At 28th week: lower one-third of the distance between the
umbilicus and xiphisternum
How to
Determine Fetal Lie and Presentation
At 32nd week: two-thirds
of the distance between the umbilicus and xiphisternum
At 36th week: at the week
of the xiphisternum
At 40th week: sinks back
to the level of the 32nd week, but the flanks are full, unlike that
in the 32nd week
The pelvic grips
(four in number) are performed to determine the lie and the presenting part of
the fetus
Fundal palpation/fundal grip
This palpation helps determine the lie and presentation of the fetus
Palpate the uterine fundus gently by laying both hands on the sides of
the fundus in an attempt to determine which pole of the fetus (the breech or
the head) is occupying the uterine fundus. The head feels like a hard globular
mass which is ballotable (moves between the fingertips of the two hands),
whereas the breech is of a softer consistency and has an indefinite outline
In the case of a transverse lie, the fundal grip will be empty
Lateral palpation/lateral grip
This palpation is used to locate the fetal back to determine the fetal
lie
Place the hands on either side of the uterus at the level of the
umbilicus and apply gentle pressure. The back of the fetus is felt like a
continuous hard, flat surface on one side of the midline and the limbs are felt
as irregular small knobs on the other side
In the case of a transverse lie, the back is felt transversely, i.e.
stretching across both sides of the midline
First pelvic grip/superficial pelvic
grip
The third maneuver must be performed gently, or it will cause pain to the
woman. Spread you right hand widely over the symphysis pubis, with the ulnar
border of the hand touching the symphysis pubis. Try to approximate the finger
and thumb, putting gentle but deep pressure over the lower part of the uterus.
The presenting part can be felt between the fingers and the thumb. Determine
whether it is the head or the breech (in the case of a longitudinal lie)
The mobility of the presenting part can also be determined by gripping
the presenting part and trying to move it. If it cannot be moved, it indicates
that the presenting part is “engaged”. The fetal head is said to be engaged if
the widest diameter of the fetal head has passed through the brim of the
pelvis, or only two finger-breadths are felt above the pelvic brim
In the case of a transverse lie, the third grip will be empty
Second pelvic grip/deep pelvic grip
To perform this grip, you must face the foot end of the mother. Keep both
the palms of your hands on the sides of the uterus, with the fingers held close
together, pointing downward and inward, and palpate to recognize the presenting
part
If the presenting part is the head (felt like a firm, round mass, which
is ballotable, unless engaged), this maneuver, in experienced hands, will also
be able to tell us about its flexion
If the woman cannot relax her muscles, tell her to flex her legs slightly
and to breathe deeply. Palpate in between the deep breaths
How to auscultate for fetal heart
sounds (FHS):
Use a fetoscope or the bell of the stethoscope for this. Remember, the
FHS is best heard on the side where the spine/back of the fetus is. For a
normal vertex presentation, the FHS is best heard midway between the line
joining the umbilicus and the anterior superior iliac spine, on the side where
the back is
In a breech presentation, the fetal heart is usually heard above the
umbilicus
Count the FHR rate for one full minute
MEASUREMENT OF FUNDAL HEIGHT – Methods and Procedures (MATERNAL AND CHILD HEALTH NURSING)
INTRANATAL CARE – Aims of Good Intranatal Care, Objectives of Intranatal Care, Intranatal Examination, Intranatal Assessment, Intranatal Care and Attention, Intranatal Education and Counseling and Role of the Nurse in Intranatal Care (MATERNAL AND CHILD HEALTH NURSING)
Childbirth is
a normal physiological process but complications may arise. The need for
effective intranatal care is therefore indispensable, even if the delivery is
going to be a normal one. The emphasis is on the cleanliness. It entails clean
hands and finger nails, a clean surface for delivery, clean cutting and care of
the cord and keeping the birth canal clean by avoiding harmful practices
AIMS OF GOOD INTRANATAL CARE
Thorough asepsis
Delivery with minimum injury to the
infant and mother
Readiness to deal with complications
such as prolonged labor, antepartum hemorrhage, convulsions, malpresentations
prolapse of the cord, etc
Care of the baby at delivery –
resuscitation, care of the cord, care of the eyes, etc
OBJECTIVES OF INTRANATAL CARE
To maintain the health and well-being
of pregnant women and their off-springs during the intranatal period
To keep the women in labor under
close observation and avoid interference with the natural process of delivery unless
there is a valid reason to do so
To encourage and support women in
labor and extend personal attention to them
To ensure a safe delivery; outcome in
the form of healthy mothers healthy babies
INTRANATAL EXAMINATION
Examining
mother is to rule out any rise in temperature and blood pressure intrauterine
bleeding and maternal distress. Examining fetuses for observing heart rate,
fetal movements and color of the liquor
INTRANATAL ASSESSMENT
Assessing
birth weight and also the Apgar score of the new-borns on the basis of heart
rate, muscle tone, respiratory effort, response to nasal stimulation and
cyanosis, if any undertaking the follow-up action
INTRANATAL CARE AND ATTENTION
Provided for
prevention of infection to birth canal, establishment of respiration of the
newborn prevention of heat loss, care of the eyes and cutting the umbilical
cord
INTRANATAL EDUCATION AND COUNSELING
Provided on
the desirability of colostrums feeding bonding personal hygiene, etc
ROLE OF THE NURSE IN INTRANATAL CARE
The community health nurse should
inspect perineum for any laceration or tear watch for bleeding
Clean the mother fex napkin;
demonstrates the perineal care
Place the mother comfortably on the
bed after delivery and provide some hot drink (coffee or tea)
Provide the instructions to family,
such as watch for bleeding in the mother as well cord bleeding in baby, to give
normal diet to the mother, report to the health authorities about the birth
INTRANATAL CARE – Aims of Good Intranatal Care, Objectives of Intranatal Care, Intranatal Examination, Intranatal Assessment, Intranatal Care and Attention, Intranatal Education and Counseling and Role of the Nurse in Intranatal Care (MATERNAL AND CHILD HEALTH NURSING)
EXAMINATION OF PLACENTA – Examination
of the Placenta, Membranes and the Umbilical Cord (MATERNAL AND CHILD HEALTH
NURSING)
A one-minute
examination of the placenta performed in the delivery room provides information
that may be important to the care of both mother and infant. The findings of
this assessment should be documented in the delivery records. During the
examination, the size, shape, consistency and completeness of the placenta
should be determined, and the presence of accessory lobes, placental infarcts,
hemorrhage, tumors and nodules should be noted. The umbilical cord should be
assessed for length, insertion, number of vessels, thromboses, knots and the
presence of wharton’s jelly. The color, luster and odor of the fetal membranes
should be evaluated, and the membranes should be examined for the presence of
large (velamentous) vessels. Tissue may be retained because of abnormal
lobation of the placenta or because of placenta accreta, placenta increta or
placenta percreta
Numerous
common and uncommon findings of the placenta, umbilical cord and membranes are
associated with abnormal fetal development and perinatal morbidity. The
placenta should be submitted for pathologic evaluation if an abnormality is
detected or certain indications are present
EXAMINATION
OF THE PLACENTA, MEMBRANES AND THE UMBILICAL CORD
Examine the
placenta and the membranes for completeness as follows:
Maternal
surface of the placenta
Hold the placenta in the palms of the
hands, keeping the palms flat and the maternal surface facing you. Look for the
following:
All the lobules must be present
The lobules should fit together
There should be no irregularities in the margins
After rinsing the maternal side
carefully with water, it should shine because of the decidual covering
If any of the lobes are missing or
the lobules do not fit together, suspect that some placental fragments may have
been left behind in the uterus
Fetal
surface
Hold the umbilical cord in one hand
and let the placenta and membranes hand down like an inverted umbrella
The umbilical vessels will be seen
passing from the cord and gradually fading into the edge of the placenta
Look for free-ending vessels and
holes which may indicate that a succenturiate lobe has been left behind in the
uterus
Look for the insertion of the cord,
particularly the velamentous insertion (the point where the cord is inserted
into the membranes and from where it travels to the placenta)
Membranes
The chorion is the layer in contact
with the uterus. It is rough and thick
The amnion is the inner layer. It is
thin and shiny
The amnion can be peeled up to the
level of insertion of the cord
Both the layers can be seen at the
edge of the hole where the membranes rupture and the fetus comes out
If the membranes are ragged, place
them together and make sure that they are complete
UMBILICAL CORD
The umbilical cord should be inspected. It has two arteries and one vein. If only one artery is found, look for congenital malformations in the baby
EXAMINATION OF PLACENTA – Examination of the Placenta, Membranes and the Umbilical Cord (MATERNAL AND CHILD HEALTH NURSING)
BLOOD PRESSURE MONITORING – Palpatory
Method and Auscultatory Method (MATERNAL AND CHILD HEALTH NURSING)
Palpatory Method
This method
is useful for measuring the systolic BP only. This is used in the absence of a
stethoscope
Ask the woman to sit or lie down
comfortably and relax. If the woman has come walking, let her rest for 5-10
minutes before measuring her BP
The woman should be titled to her
left side using a cushion placed behind her back
Place the sphygmomanometer on a flat
surface, level with the woman’s heart
Ensure that the pointer on the dial
is at zero. If not, adjust it by rotating the knob attached to the dial
Fix the inflatable cuff on the upper
part of either arm, after removing all clothing from that arm. The lower border
of the cuff should not be more than 2.5 cm from the cubital fossa (elbow)
The dial/manometer is placed at the
same level as your eye
Feel for the brachial artery over the
cubital fossa, just medial to the biceps tendon, or alternatively feel for the
pulse at the wrist of the arm, to which the cuff is tied, with your left hand
Tighten the screw of the rubber bulb
and inflate the cuff by repeatedly squeezing the bulb with your right hand
The pointer of the dial will show
increasing deflections above zero as the pressure increases within the cuff
Keep on inflating the cuff and
increasing the pressure by squeezing the rubber bulb till you do not feel the
pulse
Note the manometer reading. Increase
the pressure by 10 mm Hg above the level at which the pulse disappeared
Deflate the cuff gradually till you
feel the pulse appear again. The level at which the pulse reappears gives the
systolic BP
Deflate the cuff by loosening the
screw of the rubber bulb, and remove the cuff from the woman’s arm
AUSCULTATORY METHOD
This method
is used if a stethoscope is available. It measures both the systolic and the
diastolic BP levels
Follow the same initial steps as
mentioned in the palpatory method, and note them the woman’s systolic BP
Now raise the pressure of the cuff to
30 mm Hg above the level at which the radial pulse was no longer palpable
Place the stethoscope on the cubital
fossa, ensuring that the diaphragm is in contact with the fossa. Ideally, you
should not hear any sounds. Ensure that you are using the stethoscope
correctly, with the ear pieces facing forwards when placed in the ears
Lower the pressure of the cuff slowly,
about 2 mm Hg at a time, till you start hearing repetitive thumbing sounds. The
reading at which the sound first starts is the systolic BP
Continue lowering the pressure until
the sound first muffles and finally disappears. The reading at which the sound
finally disappears is the diastolic BP of the woman
The blood pressure is noted down on
paper as “systolic BP/diastolic BP”
BLOOD PRESSURE MONITORING – Palpatory Method and Auscultatory Method (MATERNAL AND CHILD HEALTH NURSING)
ANTENATAL CARE – Objectives,
Antenatal Examination, Antenatal Assessment, Antenatal Care and Attention and
Role of Community Health Nurse at Antenatal (MATERNAL AND CHILD HEALTH NURSING)
Antenatal
care began as a social service in Paris in 1788 for women who had committed the
double inconvenience of being pregnant and destitute. Antenatal care to be
provided to pregnant women to help them tide over the period of pregnancy
successfully and to ensure a healthy pregnancy outcome
OBJECTIVES
To maintain the health and well-being
of pregnant women and their fetuses through the period of pregnancy
To identify risk factors and apply
appropriate measures of intervention as early as possible
To identify complications of
pregnancy and institute immediate remedial measures, including referral care
To impart health education to women
on pregnancy and childbirth, and to sensitize them on the desirability of
family planning, fertility control and breastfeeding
To lay the foundations of a healthy
pregnancy outcome and good mother-child relationship
ANTENATAL EXAMINATION
Examining
mother to record height, weight, blood pressure and to rule out anemia,
jaundice, edema, varicosities, breast tumors, nipple deformities, hydramnios,
multifetal pregnancy, anteversion or retroversion of the uterus and also to
observe the height of fundus and presentation, position and attitude of fetus
ANTENATAL ASSESSMENT
Assessing
maternal risk on the basis of gravidity maternal age, maternal weight,
pregnancy weight gain, previous obstetric experience and accordingly placing
mothers in low risk class for appropriate management
ANTENATAL CARE AND ATTENTION
The care
provided for risk intervention, anemia prophylaxis and tetanus prophylaxis
Antenatal
education and counseling provided about diet, work, exercise, travel, smoking,
drinking, bathing, clothing, chemotherapy, family planning, breastfeeding,
mental preparation, active participation and warning signals
ROLE OF COMMUNITY HEALTH NURSE AT ANTENATAL
The community health nurse should
assist the parents in understanding the anatomy and physiology of pregnancy,
labor and birth
Contact every expected mother early
in pregnancy and help her seek adequate medical supervision
Teach mother to monitor visual
disturbances, edema of face, epigastric pain, signs of infection, burning on
urination, any vaginal discharge and absence of or decrease in fetal movements
after initial pressure
Respond to mother’s questions about
bathing, douching, work, sex, exercise, etc
Help parents discuss and explore
feeling related to child bearing and rearing
Prepare mother for physical work of
labour through the use of relaxation and breathing exercises for the various
phases of labor
Teach the mother to avoid over the
counter or prescription drugs without checking with her care provider because
many drugs considered harmless may be teratogenic to the developing fetus
Teach the mother the importance of
adequate fluid intake and moderate exercise to promote circulation and prevent
stasis
Demonstrating and teaching to mother
and relatives on several aspects of maternity care
The community health nurse acting as
liaison between the hospital, health center, clinic and home in referring
mothers to appropriate agency for safe delivery, when indicated
Maintaining adequate records all
mother in her area and recording relevant information adequately on follow-up
visits
Training midwives and dais and
participating in training programs for nurses, midwives, village health nurses
(health worker F/M)
ANTENATAL CARE – Objectives, Antenatal Examination, Antenatal Assessment, Antenatal Care and Attention and Role of Community Health Nurse at Antenatal (MATERNAL AND CHILD HEALTH NURSING)