GUILLAIN-BARRE SYNDROME OR INFECTIOUS POLYNEURITIS – Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
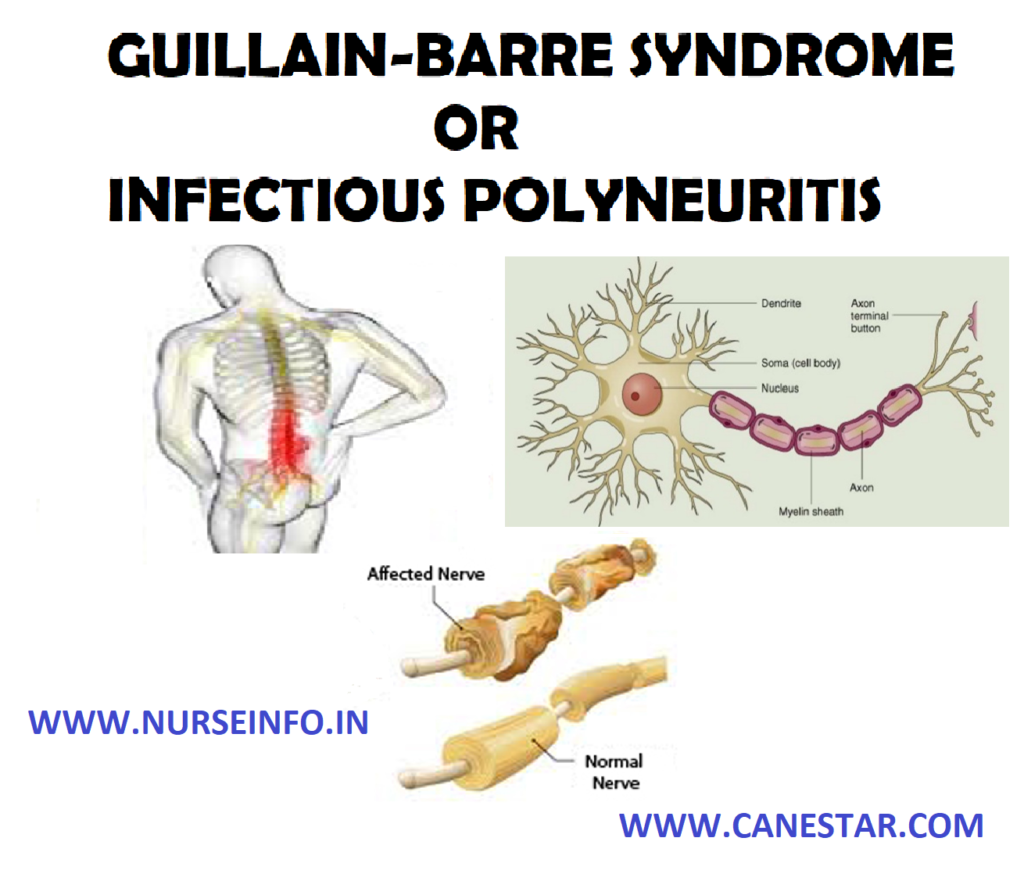
- Guillain-Barre Syndrome (GBS) is a acute condition that involves progressive muscle weakness or paralysis. It is an autoimmune disorder in which the body’s immune system attacks its own nervous system, causing inflammation that damages the myelin sheath of the nerve. This damage (demyleinazation) slows or stops the conduction of impulses through the nerve. The impairment of nerve impulses to the muscles leads to symptoms that may include muscle weakness, paralysis, spasms, numbness, tingling or pin-and-needle sensations and tenderness.
ETIOLOGY
- Camphylobacter jejuni infection: camphylobacter infection is also the most common risk factor for Guillain-Barre. It is often found in undercooked food, especially poultry.
- Influenza
- Cytomegalovirus
- Epstein-Barr virus infection
- Mycoplasma pneumonia
- HIV or AIDS
PATHOPHYSIOLOGY
A condition of symptoms characterized by a widespread, inappropriate inflammatory immune response —- the syndrome progresses from the feet up and generally affects one side more than the other —- nerve condition is interrupted as T-cells are activated and antibodies attack the myelin sheath —- a polyneuropathies, that include the associated neurological symptoms related to immune response —- symptoms continually progress in severity over the course of a few hours to several days —- symptoms initiate in lower extremities with symmetrical paresthesia that may advance to paralysis
SIGNS AND SYMPTOMS
- Loss of tendon reflexes in the arms and legs
- Tingling or numbness (mild loss of sensation)
- Muscle tenderness or pain (maybe a cramp-like pain)
- Uncoordinated movement (cannot walk without help)
- Low blood pressure or poor blood pressure control
- Abnormal heart rate
- Blurred vision and double vision
- Clumsiness and falling
- Difficulty moving face muscles
- Muscle contractions
- Feeling the heartbeat
EMERGENCY SYMPTOMS
- Breathing temporarily stops
- Cannot take a deep breath
- Difficulty breathing
- Difficulty swallowing
- Drooling
- Fainting
- Feeling light-headed when standing
DIAGNOSTIC EVALUATION
- Spinal tap: this test is also referred to as a lumbar puncture. A spinal tap involves taking a small amount of fluid from the spine in the lower back. The fluid is then tested to detect protein levels. People with Guillain-Barre typically have higher-than-normal levels of protein in their cerebrospinal fluid
- Electromyography: an electromyography is a nerve function test. It reads electrical activity from the muscles and help to learn if the muscle weakness is caused by nerve damage or muscle damage
MANAGEMENT
- Physical therapy: before recovery, a caregiver may need to manually move the arms and legs. This will help the muscles strong and mobile. After recovery, physical therapy will helps to strengthen and flex the muscles again. Therapy includes massages, exercises and frequent position changes.
- Plasmapheresis: the immune system produces protein called antibodies that normally attack harmful foreign substances, such as bacteria and viruses. Guillain-Barre occurs when the immune system mistakenly makes antibodies that attack the healthy nerves of the nervous system. Plasmapheresis is intended to remove the antibodies attacking the nerves from the blood. During this procedure, blood is removed from the body by machine that removes the antibodies from the blood and then the blood is returned to the body
- Intravenous immunoglobulin: high doses of immunoglobulin can also help to block the antibodies causing Guillain-Barre.
NURSING MANAGEMENT
Nursing Diagnosis
- Ineffective breathing pattern and airway clearance related to respiratory muscle weakness or paralysis, decreased cough reflex, immobilization
- Impaired physical mobility related to paralysis, ataxia
- Risk for impaired skin integrity, pressure sores related to muscle weakness, paralysis, impaired sensation, changes in nutrition, incontinence
- Imbalanced nutrition, less than body requirements related to difficulty chewing, swallowing, fatigue, limb paralysis
- Impaired elimination: constipation, diarrhea, related to inadequate food intake, immobilization
- Impaired verbal communication related to the VII cranial nerve paralysis, tracheostomy
- Ineffective copying related to the patient’s disease state
Interventions
- Monitor respiratory status through vital capacity measurements, rate and depth of respirations and breath sounds
- Monitor level of muscle weakness as it ascends toward respiratory muscles. watch for breathlessness while talking which is a sign of respiratory fatigue
- Monitor the patient for signs of impending respiratory failure
- Monitor gag reflex and swallowing ability
- Position patient with the head of bed elevated to provide for maximum chest excursion
- Avoid giving opioids and sedatives that may depress respirations
- Position patient correctly and provide range-of-motion exercises
- Provide good body alignment, range-of-motion exercises, and change of position to prevent complications such as contractness, pressure sores, and dependent edema
- Ensure adequate nutrition without the risk of aspiration
- Encourage physical and occupational therapy exercises to help the patient regain strength during rehabilitation phase
- Provide assistive devices as needed (cane or wheelchair) to maximize independence and activity
- If verbal communication is possible, discuss the patient’s fears and concerns
- Provide choices in care to give the patient a sense of control
- Teach patient about breathing exercises or use of an incentive spirometer to re-establish normal breathing patterns
- Instruct patient to wear good supportive and protective shoes while out of bed to prevent injuries due to weakness and paresthesia
- Instruct patient to check feet routinely for injuries because trauma may go unnoticed due to sensory changes
- Urge the patient to maintain normal weight because additional weight will further stress monitor function
- Encourage scheduled rest periods to avoid fatigue