RETINAL DETACHMENT – Types and
Causes, Risk Factors, Signs and Symptoms, Diagnostic Evaluation and Management
The retina
is a light-sensitive membrane located at the back of the eye. When retina is
detached from its pigmented epithelium is called retinal detachment. It is
characterized by partial or total loss of vision.
TYPES AND CAUSES
Rhegmatogenous retinal detachment: it
is characterized by tear or hole in retina. This allows fluid from within the
eye to slip through the opening and get behind the retina. The fluid separates
the retina from the membrane that provides it with nourishment and oxygen. The
pressure from the fluid can push the retina away from the retinal pigment
epithelium, causing the retina to detach.
Tractional retinal detachment: it
occurs when scar tissue on the retina’s surface contracts and causes the retina
to pull away from the back of the eye. This is a less common type of detachment
that typically affects people with diabetes
Exudative detachment: this type of
detachment is caused by retinal diseases such as inflammatory disorder or Coats
disease, which causes abnormal development in the blood vessels behind the
retina.
RISK FACTORS
Risk factors
for retinal detachment include:
Posterior vitreous detachment (PVD):
a common condition in aging individuals, in which the fluid in the retina
breaks down, putting strain on the retinal fibers
Extreme nearsightedness
Family history of retinal detachment
Trauma to the eye
Being over 40 years old
Prior history of retinal detachment
Complications from cataract surgery
Diabetes
SIGNS AND SYMPTOMS
There is no
pain associated with retinal detachment, but there are usually symptoms before
the retina becomes detached. Primary symptoms include:
Blurred vision
Partial vision loss
Flashes of light when looking to the
side
Areas of darkness in field of vision
Suddenly seeing many floaters (small
bits of debris that appear as black flecks or strings floating before the eye).
DIAGNOSTIC EVALUATION
Tonometry: to evaluate the eye
pressure
Gonioscopy: to inspect the drainage
angle of eye
Ophthalmolscopy: to evaluate the
optic nerve
SURGICAL
MANAGEMENT
Photocoagulation: it is a laser burn
around the tear site and the resulted scar will fixes the retina to the back of
the eye.
Cryopexy: it consists of application
of freezing probe to the tear site and the resulting scarring will help
hold the retina in place
Retinopexy: in this doctor will put a
gas bubble in eye to help the retina move back into place. Once the retina is
back in place, with the help of laser the holes are sealed out
Scleral buckling: in this the sclera
is pulled near the retina by decreasing the diameter of sclera. A small piece
of silicone maybe sutured on or around the eye in a fashion that indents the
eyeball and brings the retinal break that caused the detachment again in
contact with it. This allows the subretinal fluid to reabsorb and the retina to
reattach. Sometimes an air or gas bubble is injected at the time of surgery to
aid reattachment of the retina.
Vitrectomy: by making tiny incisions into the eyeball,
instruments are able to remove all the vitreous and subretinal fluid and
reattach the retina. The retinal tear or tears that caused the detachment are
then treated with laser to cause a permanent adhesive scar in this area and
prevent a future detachment. A gas bubble, or less frequently and oil bubble,
is instilled in the eye at the end of surgery to maintain the retina in contact
with the eye wall as the laser scar matures
NURSING MANAGEMENT
Nursing
Diagnosis
Anxiety related to possible vision
loss
Disturbed sensory perception related
to visual impairment
Ineffective health maintenance
related to knowledge deficit
Risk for injury related to impaired
vision
Self-care deficit related to impaired
vision
Interventions
Prepare the patient for surgery
Instruct the patient to remain quiet in prescribed (dependent) position,
to keep the detached area of the retina in dependent position
Patch both eyes
Wash the patient’s face with antibacterial solution
Instruct the patient not to touch the eyes to avoid contamination
Administer preoperative medication as ordered
Take measures to prevent
postoperative complications
Caution the patient to avoid bumping head
Encourage the patient no to cough or sneeze or to perform other
strain-inducing activities that will increase intraocular pressure
Encourage ambulation and independence
as tolerated
Administer medication for pain,
nausea and vomiting as directed
Provide quiet diversional activities,
such as listening to a radio or audio books
Teach proper technique in giving eye
medications
Advise patient to avoid rapid eye
movements for several weeks as well as straining or bending the head below the
waist
Advise patient that driving is
restricted until cleared by ophthalmologist
Teach the patient to recognize and
immediately report symptoms that indicate recurring detachment, such as
floating spots, flashing lights and progressive shadows
Advise patient to follow-up
RETINAL DETACHMENT – Types and Causes, Risk Factors, Signs and Symptoms, Diagnostic Evaluation and Management
OSTEITIS DEFORMANS (PAGET’S DISEASE) –
Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluations and
Management
Paget’s
disease of bone disrupts the body’s normal bone recycling process, in which old
bone tissue is gradually replaced with new bone tissue. Overtime, the affected bones may become
fragile and weak. Page’t disease of bone most commonly occurs in the pelvis,
skull, spine and legs. The involved bone can be soft, leading to weakness and
bending of the pelvis, low back (spine), hips, thighs, head and arms.
ETIOLOGY
Both genetic and environmental
factors are thought to play a role
About 15% of people with Paget’s
disease have a family history
Autosomal dominant inheritance has
also been described in some families
Mutations have been identified in
four genes that cause Paget’s disease
Mechanical stress may play a role
Paramyxovirus infection (including
measles and respiratory syncytial virus) has been suggested as a possible
trigger but this has been disputed.
PATHOPHYSIOLOGY
The
metabolic hyperactivity is the main feature of Paget’s disease —- the primary
abnormality is believed to be an intense focal resorption of normal bone by
abnormal osteoclasts, leading to creation of voids and cavities in the bone
—- these osteoclasts are abnormal in size, activity, and quantity and have
excess nuclei —- the physiological compensatory mechanism for repair results
in the deposition of fibrotic tissue and even new bone in the cavities by
osteoblasts —- the osteoblast activity is so rapid that newly formed bone is
not organized and remains irregular and woven in nature —- the newly formed
woven bone is less resistant and more elastic than typical lamellar bone, and
hence prone to deformity and micro-fractures, especially in the weight-bearing
extremities —- there is a high degree of vascularity in the pagetoid bone
cause of pain
Paget’s
disease Evolves Through three Distinct Phases
An initial, short-lived burst of
multinucleate osteoclastic activity causing bone resorption
A mixed phase of both osteoclastic
and osteoblastic activity, with increased levels of bone turnover leading to
deposition of structurally abnormal bone
A final chronic sclerotic phase,
during which bone formation outweighs bone resorption
SIGNS AND SYMPTOMS
Most people
who have Page’s disease of bone experience no symptoms. When symptoms do occur,
the most common complaint is bone pain which may includes:
Pelvis: Paget’s disease of bone in
the pelvis can cause hip pain
Skull: an overgrowth of bone in the
skull can cause hearing loss or headaches
Spine: if spine is affected, nerve
roots can become compressed. This can cause pain, tingling and numbness in an
arm or leg
Leg: as the bones weaken, they may
bend. Enlarged and misshapen bones in legs can put extra stress on nearby
joints, which may cause wear-and-tear arthritis in knee or hip.
DIAGNOSTIC EVALUATIONS
Bone-specific alkaline phosphatase
(BSAP) levels are raised
Urinary excretion of
deoxypyridinoline and N-telopeptide are elevated
Serum calcium, phosphorus, and
parathyroid hormone levels are usually normal but immobilization may lead to
hypercalcemia
X-rays may show a number of signs of
both osteolysis and excessive bone formation occur
Radionuclide bone scans can show the
extent of the disease
Bone biopsy may be needed if
malignant change is suspected
MANAGEMENT
Treatment
approaches can focus on providing physical assistance, including the addition
of wedges in the shoe, walking aids and the administration of physical therapy
and pharmacotherapy
Pharmacotherapy
Nonsteroidal anti-inflammatory drugs
(NSAIDs) and paracetamol may be effective for pain
Anti-resorptive therapy is with
either bisphosphonates or calcitonin
Biphosphonates:
Oral or intravenous bisphosphonates are the main stay of treatment
They are thought to reduce bone turnover, improve bone pain, promote
healing of osteolytic lesions and restore normal bone histology
Newer bisphosphonates such as zoledronic acid may help to better achieve
metabolic control of the disease and so improve these statistics
Pamidronate, risedronate, and zoledronic acid are preferred
Any calcium and vitamin D deficiency needs to be corrected before
starting a bisphosphonate to avoid hypocalcemia
All oral medications
should be taken with a large glass of water (6-8 oz) upon arising in the
morning. Patients should remain upright for the next 30 minutes and not eat
until that time has passed. Any of these treatments can be repeated if
necessary. Side effects of these medicines may involve heartburn and sometimes
increasing bone pain for a short period of time
There are
also injectable medications. Injectable medications that can be given for
Paget’s include:
Pamidronate: which is injected in the
vein once a month or once every few months? The injection takes a few hours.
Unusually, there can be inflammation of the eye or loss of bone around the
teeth (osteonecrosis)
Zoledronate: this is injected in the
vein once a year
Calcitonin, a hormone that is
injected under the skin several times a week
COMPLICATIONS
Complications
from Paget’s disease depend on the site affected and the activity of the
disease:
Bone pain
Bone deformity, kyphosis, frontal
bossing of the skull, an enlarged maxilla, an increase in head size
Pathological fractures
Osteoarthritis
Deafness and tinnitus may be due to
compression of cranial nerve VIII
Spinal stenosis
Nerve compression syndromes
NURSING MANAGEMENT
Acute pain related to nerve
compression, muscle spasm
Interventions
Assess complaints of pain, location,
duration of attacks, precipitating factors which aggravate
Maintain bedrest, semi-Fowler
position to the spinal bones, hips and knees in a state of flexion, supine
position
Use logroll (board) during a change
of position
Auxiliary mounting brace
Limit activity during the acute phase
according to the needs
GLAUCOMA – Etiology and Risk Factors,
Pathophysiology, Types, Signs and Symptoms, Diagnostic Evaluation and
Management
Glaucoma is
a disease of the major nerve of vision, called the optic nerve. Glaucoma is
characterized by a particular pattern of progressive damage to the optic nerve
that generally begins with a subtle loss of side vision.
Open-angle glaucoma (chronic):
chronic open-angle glaucoma is the most common form of glaucoma. The ‘open’
drainage angle of the eye can become blocked leading to gradual increased eye
pressure. If this increased pressure results in optic nerve damage, it is known
as chronic open-angle glaucoma. The optic nerve damage and vision loss usually
occurs so gradually and painlessly
Angle-closure glaucoma: angle-closure
glaucoma results when the drainage angle of the eye narrows and becomes
completely blocked. In the eye, the iris may close off the drainage angle and
cause a dangerously high eye pressure. When the drainage angle of the eye
suddenly becomes completely blocked, pressure builds up rapidly, and this is
called acute angle-closure glaucoma
Exfoliation syndrome: exfoliation
syndrome is a common form of a open-angle glaucoma that results when there is a
buildup of abnormal, whitish material on the lens and drainage angle of the
eye. This material and pigment from the back of the iris can clog the drainage
system of the eye, causing increased eye pressure.
Pigmentary glaucoma: pigmentary
glaucoma is characterized by the iris bowing backwards, and coming into contact
with the support structures that hold the lens in place. This position disrupts
the cells lining the back surface of the iris containing pigment, and results
in a release of pigment particles into the drainage system of the eye. This
pigment can clog the drain and can lead to an increase in eye pressure.
Low-tension glaucoma: this is another
form that experts do not fully understand. Even though eye pressure is normal,
optic nerve damage still occurs. Perhaps the optic nerve is over-sensitive or
there is atherosclerosis in the blood vessel that supplies the optic nerve.
SIGNS AND SYMPTOMS
The signs
and symptoms of primary open angle glaucoma and acute angle-closure glaucoma
are quite different.
Signs and
Symptoms of Primary Open-angle Glaucoma
Peripheral vision is gradually lost.
This nearly always affects both eyes
In advanced stages, the patient has
tunnel vision
Signs and
Symptoms of Closed Angle Glaucoma
Eye pain, usually severe
Blurred vision
Eye pain is often accompanied by
nausea and sometimes vomiting
Light appears to have extra halo-like
glows around them
Red eyes
Sudden, unexpected vision problems,
especially when lighting is poor.
Common
Symptoms are:
Unusual trouble adjusting to dark
rooms
Difficulty focusing on near or
distant objects
Squinting or blinking due to unusual
sensitivity to light or glare
Change in color of iris
Red-rimmed, encrusted or swollen lids
Recurrent pain in or around eyes
Double vision
Dark spot at the center of viewing
Lines and edges appear distorted or
wavy
Excess tearing or ‘watery eyes’
Dry eyes with itching or burning
Sudden loss of vision in one eye
Sudden hazy or blurred vision
Flashes of light or black spots
Halos or rainbows around light
DIAGNOSTIC EVALUATION
Eye-pressure test: Tonometer, a
device which measures intraocular pressure. Some anesthetic and a dye are
placed in the cornea, and a blue light is held against the eye to measure
pressure. This test can diagnose ocular hypertension; a risk factor for
open-angle glaucoma.
Gonioscopy:
this examines the area where the fluid drains out of the eye. It helps
determine whether the angle between the cornea and the iris is open or blocked
(closed)
Perimetry
test: also known as a visual field test. It determines which area of the
patient’s vision is missing. The patient is shown a sequence of light spots and
asked to identify them. Some of the dots are located where the person’s
peripheral vision is; the part of vision that is initially affected by
glaucoma. If the patient cannot see those peripheral dots, it means that some
vision damage has already occurred.
Optic nerve
damage: the ophthalmologist uses instruments to look at the back of the eye,
which can reveal any slight changes which may also point towards glaucoma onset
Visual
acuity test: this eye chart test measures how well you see at various distances
Visual field
test: this test measures peripheral (side vision)
Dilated eye
exam: in this exam, drops are placed in eyes to widen, or dilate, the pupils.
Eye care professional uses a special magnifying lens to examine retina and
optic nerve for signs of damage and other eye problems.
MANAGEMENT
Medical
Management
Prostaglandin analogues: these medications
have prostaglandin-like compounds as their active ingredient. They increase the
outflow of the fluid inside the eye. Examples include Xalatan and Lumigan.
(Beta blockers: these medications reduce the amount of fluid the eye produces.
Some patients may experience breathing problems, hair loss, fatigue,
depression, memory loss, a drop in blood pressure. Examples of such medications
include timolol, betaxolol and metipranolol). (Carbonic anhydrase inhibitors:
these also reduce fluid production in the eye. Side effects may include nausea,
eye irritation, and dry mouth, frequent urination, tingling in the fingers or
toes, and a strange taste in the mouth. Examples include brinzolamide and
dorzolamide). (cholinergic agents: also known as miotic agents).
SURGERY
Trabeculoplasty: a high-energy laser
beam is used to unblock clogged drainage canals, making it easier for the fluid
inside the eye to drain out. This procedure nearly always reduces inner eye
pressure. However, the problem may come back.
Filtering surgery (viscocanalostomy):
if eyedrops and laser surgery are not effective in controlling eye pressure,
trabeculectomy is required. This procedure is performed in a hospital or an
outpatient surgery center. Patient receives a medication to help relax and
usually an injection of anesthetic to numb eye. Using small instruments under
an operating microscope, an opening is created in the sclera and removes a
small piece of eye tissue at the base of cornea through which fluid drains from
eye (the trabecular meshwork). The fluid in eye can now freely leave the eye
through this opening. As a result, eye pressure will be lowered.
Drainage implant (aqueous shunt
implant): this option is sometimes used for children or those with secondary
glaucoma. A small silicone tube is inserted into the eye to help it drain out
fluids better.
Laser cycloablation (ciliary body
destruction, cyclophotocoagulation or cyclocryopexy) is another form of laser
treatment generally reserved for patient with severe forms of glaucoma with
poor visual potential. This procedure involves applying laser burns or freezing
to the part of the eye that makes the aqueous fluid. This therapy destroys the
cells that make the fluid, thereby reducing the eye pressure
Aqueous shunt devices: they are artificial
drainage devices used to lower the eye pressure. They are essentially plastic
microscopic tubes attached to a plastic reservoir. The reservoir is placed
beneath the conjunctival tissue. The actual tube is placed inside the eye to
create a new pathway for fluid to exit the eye. This fluid collects within the
reservoir beneath the conjunctiva creating a filtering bleb. This procedure
maybe performed as an alternative to trabeculectomy in patients with certain
types of glaucoma.
NURSING MANAGEMENT
Nursing
Assessment
Evaluate the patient for any of the
clinical manifestations
Assess patient’s level of anxiety and
knowledge base
Assess the patient’s knowledge of
disease process
Nursing
Diagnosis
Pain related to increased to
increased IOP
Fear related to pain and potential
loss of vision
Self-care deficit related to visual
deficit
Anxiety related to lack of knowledge
about the surgical and postoperative experience
Risk for injury related to blurred
vision
Risk for infection related to trauma to
incision
Acute pain related to trauma to
incision
Intervention
Relieving
Pain
Notify health care provider
immediately
Administer medications as directed
Explain to patient that the goal of
treatment is to reduce IOP as quickly as possible
Explain procedures to patient
Reassure patient that with reduction
in IOP, pain and other signs and symptoms should subside
Relieving
Fear
Provide reassurance and calm presence
to reduce anxiety and fear
Prepare patient for surgery, if
necessary
Relieving
Anxiety
Assess the degree and duration of
visual impairment
Orient the patient to new environment
Explain the perioperative routines
Push to perform daily living habits
when able
Encourage the participation of family
Prevention
of Injury
Provided a comfortable position to
the patient
Help the patient to set the
environment
Orient the patient in a room
Discuss the need for use of goggles
when instructed
Do not put pressure over the affected
eye trauma
Used the proper procedures when providing
eye drugs
Promoting
Self-Care
Cleared the all doubts of patient
regarding the disease condition
Maintained good IPR with the patient
Provided calm cool environment to the
patient
Music therapy and pet therapy given
to patient
Relaxation therapy also provided to
relieve the anxiety of patient
Improving
Knowledge
Provided adequate knowledge about a
disease condition
Provided the sunglasses to patient
during exposure to sunlight
Provided medications to patient on
proper time
Advised the patient to talk with
doctor
COMPLICATIONS
If left
untreated, glaucoma will cause progressive vision loss, normally in these
stages:
Blind spots in peripheral vision
Tunnel vision
Total blindness
GLAUCOMA – Etiology and Risk Factors, Pathophysiology, Types, Signs and Symptoms, Diagnostic Evaluation and Management
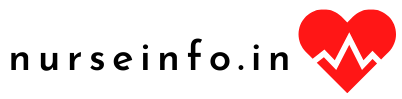
EYE BANKING AND CORNEAL
TRANSPLANTATION STEPS OR PROCEDURE
FUNCTIONS OF EYE BANK,
CONTRAINDICATIONS FOR DONATION, RETRIEVAL PROCEDURE, ROLE OF NURSE DURING
CORNEAL TRANSPLANTATION, AFTER SURGERY and HOME CARE INSTRUCTIONS
It is an
organization that deals with the collection, storage and distribution of donor
eyes for the purpose of corneal grafting
Corned blindness is a major form of
visual deprivation in developing countries. A high percentage of these
individuals can be visually rehabilitated by corneal transplantation
(keratoplasty), a procedure that has very high rate of success among organ
transplants. Quality of donor cornea, the nature of recipient pathology and the
availability of appropriate postoperative care are the factors that determine
the final outcome of this procedure. In corneal grafting, this diseased and
opaque cornea is replaced by a healthy transplant cornea taken from a donor
eye.
A corneal transplant can take one of
two forms: a full-thickness penetrating keratoplasty, involving excision and
replacement of the entire cornea, or a lamellar keratoplasty, which removes and
replaces a superficial layer of corneal tissue.
FUNCTIONS OF EYE BANK
Procurement
and supply of donor cornea to the corneal surgeons is the primary goal of eye
banks.
The eye bank collects the eyes of
voluntary registered eye donors after their death of those deceased person when
enlightened relatives agree to donate the eyes as a service to humanity. From
hospital deaths and from postmortem cases, after obtaining the consent from the
next of kin.
These eyes are processed by the Eye
Bank and are supplied to eye surgeons for corneal grafting and other sight
restoring operations
Before proceeding for recovery eye
bank personnel should ascertain the following details: location, age of the
donor, cause of death and time of death.
CONTRAINDICATIONS FOR DONATION
All eye banks have age limits both
minimum and maximum
Previous corneal graft
Death of unknown cause
Dementia
Creutzfeldt-Jacob disease
Subacute sclerosing panencephalitis
Congential rubella
Reyes syndrome
Active viral encephalitis or
encephalitis of unknown origin
Active septicemia
Rabies
Retinoblastomas, tumors of the
anterior segment
Active ocular infections
Pterygia or other superficial
disorders of the conjunctiva or corneal surface
Certain intraocular or anterior
segment surgeries
Leukemia
Active disseminated lymphomas
Hepatitis B and C, HTLV-1 or 2, HIV,
syphilis
Behavioral and or social issues, i.e.
homosexual or other high-risk sexual behavior within the last 5 years
Intravenous drug use for nonmedical
reasons within the last 5 years
Exposure to infectious disease within
the last year by contact with an open wound, needle stick, or mucous membrane
Tattooing or piercing within the last
12 months using shared instruments
RETRIEVAL PROCEDURE
Retrieval procedure could be either
enucleation or corneal scleral rim excision
Eye Bank team on arrival at the
location should locate the next of kin and convey condolence and obtain death
certificate
In the absence of a death certificate
the registered medical practitioner should satisfy self that life is extinct
The eye bank team should obtain
consent on a consent form from the legal custodian of the donor
After obtaining consent the donor
should be identified either through a tag or through the next of kin
The eye bank team should then proceed
to prepare the site
Gross physical examination should be
conducted with utmost respect for observations regarding build: average,
healthy or emaciated
Eye bank team should look out for
needle marks on the arm, skin lesions, etc
Eye bank team should look out for
ulcers or gangrene in exposed areas
Ocular examination should be
conducted
Medical records and medical
information should be obtained
Information for hemodilution should
be obtained
Social history of the donor should be
obtained wherever possible from the next of kin
ROLE OF NURSE DURING CORNEAL TRANSPLANTATION
Explain the transplant procedure to
the patient and answer any questions he may have
Advise him that healing will be slow
and that his vision may not be completely restored until the sutures are
removed, which may be in about a year
Tell the patient that most corneal
transplants are performed under local anesthesia and that he can expect
momentary burning during injection of the anesthetic
Explain to him that the procedure
will last for about an hour and that the he must remain still until it has been
completed
Tell the patient that analgesics will
be available after surgery because he may experience a dull aching
Inform him that a bandage and
protective shield will be placed over the eye
As ordered, administer a sedative or
an osmotic agent to reduce intraocular pressure
Ensure that the patient has signed a
consent form
AFTER SURGERY
After the patient recovers from the
anesthetic, assess for and immediately report sudden, sharp, or excessive pain,
bloody, purulent, or clear viscous drainage or fever
As ordered, instill corticosteroid
eyedrops or topical antibiotics to prevent inflammation and graft rejection
Instruct the patient to lie on his
back or on his unaffected side, with the bed flat or slightly elevated as
ordered. Also, have him avoid rapid head movements, hard coughing or sneezing,
bending over, and other activities that could increase intraocular pressure;
likewise, he should not squint or rub his eyes
Remind the patient to ask for help in
standing or walking until he adjusts to changes in his vision
Make sure that all his personal items
are within his field of vision
HOME CARE INSTRUCTIONS
Teach the patient and his family to
recognize the signs of graft rejection (inflammation, cloudiness, drainage, and
pain at the graft site)
Instruct them to immediately notify
the doctor if any of these signs occur
Emphasize that rejection can occur
many years after surgery; stress the need for assessing the graft daily for the
rest of the patient’s life. Also, remind the patient to keep regular
appointments with his doctor
Tell the patient to avoid activities
that increase intraocular pressure, including extreme exertion, sudden, jerky
movements, lifting or pushing heavy objects and straining during defecation
Explain the photophobia, a common
adverse reaction, gradually decreases as healing progresses
Suggest wearing dark glasses in
bright light
Teach the patient how to correctly
instill prescribed eyedrops
Remind the patient to wear an eye
shield when sleeping
Tell the patient to consult with the
surgeon before driving or participating in sports or other recreational
activities
FUNCTIONS OF EYE BANK, CONTRAINDICATIONS FOR DONATION, RETRIEVAL PROCEDURE, ROLE OF NURSE DURING CORNEAL TRANSPLANTATION, AFTER SURGERY and HOME CARE INSTRUCTIONS
CATARACT – Risk Factors and Etiology,
Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
A cataract
is a clouding or opacity of the normally clear lens of eye. The patient may
have a cataract in one or both the eyes. Cataract is the third leading cause of
preventable blindness.
RISK FACTORS AND ETIOLOGY
Increasing age
Diabetes
Drinking excessive amounts of alcohol
Excessive exposure to sunlight
Exposure to ionizing radiation, such
as that used in X-rays and cancer
radiation therapy
Family history of cataracts
High blood pressure
Obesity
Previous eye injury or inflammation
Previous eye surgery
Prolonged use of corticosteroid
medications
Smoking
PATHOPHYSIOLOGY
Following
are the various mechanisms involves in the occurrence of cataract:
Caused by degeneration and
opacification of existing lens fibers, formation of aberrant fibers or
deposition of other material in their place.
Loss of transparency occurs because
of abnormalities of lens protein and consequent disorganization of the lens
fibers
Any factor that disturbs the critical
intra and extra-cellular equilibrium of water and electrolytes, the colloid
system within the fibers causing opacification
Fibrous metaplasia of lens fibers
occurs in complicated cataract
Epithelial cell necrosis occurring in
angle closure glaucoma leads to focal opacification of the lens epithelium
Abnormal products of metabolism,
drugs or metals can be deposited in storage diseases, metabolic diseases and
toxic reactions
Three
biochemical factors are evident in cataract formation:
Hydration: seen particularly in
rapidly developing forms. Actual fluid droplets collect under the capsule
forming lacunae between fibers, the entire tissue may swell and becomes opaque,
and this process is reversible in early stage, as in juvenile insulin dependent
diabetes. Hydration maybe due to osmotic changes in the lens or due to changes
in the semipermeability of the capsule
Denaturation of lens protein: if the
proteins are denatured with an increase in insoluble protein, a dense opacity
is produced. This stage is irreversible and opacity does not clear, this change
is seen in young lens or the cortex of the adult nucleus where metabolism is
active
Sclerosis: inactive fibers of the
nucleus suffer from degenerative change of slow sclerosis
Altered the
metabolic process within lens —- reduction in oxygen uptake —- increase in
water content followed by dehydration —- protein in the lens undergoes
numerous age related changes —- causes the formation of cataract
TYPES OF CATARACT
Nuclear cataracts: a nuclear cataract
may at first causes more nearsighted. But with time, the lens gradually turns
more densely yellow and further cloudy. As the cataract slowly progresses, the
lens may even turn brown. Advanced yellowing or browning of the lens can lead
to difficulty distinguishing between shades of color.
Cortical cataracts: a cortical
cataract begins as whitish, wedge-shaped opacities or steaks on the outer edge
of the lens cortex
Posterior subcapsular cataracts: a
posterior subcapsular cataract starts as a small, opaque area that usually
forms near the back of the lens, right in the path of light on its way to the
retina
Congenital cataracts (Aphakia): some
people are born with cataracts or develop them during childhood. Such cataracts
maybe the result of the mother having an infection during pregnancy
Hypermature shrunken cataract: when
cortex disintegrates and transform into mass. The lens become inspissated and
shrunken, the anterior capsule becomes thickened
Morgagnian Hypermature Cataract: sometimes
cortex becomes liquefies and nucleus sink into the bottom. The liquefied cortex
become milky and nucleus is seen as brown mass, visible as semicircular line in
pupillary area altering its position with change in position of the head
SIGNS AND SYMTPOMS
Clouded, blurred or dim vision
Increasing difficulty with vision at
night
Sensitivity to light and glare
Seeing ‘halos’ around lights
Frequent changes in eyeglass or
contact lens prescription
Fading or yellowing of colors
Double vision in a single eye
DIAGNOSTIC EVALUATION
Visual acuity test: a visual acuity
test uses an eye chart to measure how well an eye can read a series of letters
Slit-lamp examination: with this
examination, the eye can be visualizing at large scale by magnifying the eye.
The microscope is called a slit lamp; it uses an intense line of light, a slit,
to illuminate cornea, iris, lens and the space between iris and cornea
Retinal examination: to visualize the
retina
Other tests:
Snellen visual acuity test
Opthalmoscopy
Slit lamp bimicroscopic examination
Glare testing
Keratometry
Ocular examination
Perimetry: to determine the scope of
visual fields
MANAGEMENT
Objective of
Cataract Surgery
The objective of cataract surgery is
to remove the opacified lens
Successful treatment of acute attack
and prompt alleviation of manifestations
Prevention of complications and
further attacks
Rehabilitation and education of the
clients and significant others
Pharmacologic
Therapy
Beta carotene
Vitamin C and E
Antioxidant supplements
Selenium
Multivitamin supplements
Contact lenses
Strong bifocals
Glasses
Mydriatics: Phenylephrine HCL acid
Cyloplegics: Tropicamide
Homatropine
Atropine
Surgical
Management
Phacoemulsification: in this method,
surgery can usually be performed in less than 30 minutes and usually requires
only minimal sedation. Numbing eyedrops or an injection around the eye is used
and, in general, no stitches are used to close the wound, and often no eye
patch is required after surgery
Extracapsular cataract extraction
surgery: this procedure is used mainly for very advanced cataracts where the
lens is too dense to dissolve into fragments. This technique requires a larger
incision so that the cataract can be removed in one piece without being
fragmented inside the eye. An artificial lens is placed in the same capsular
bag as with the phacoemulsification technique. This surgical technique requires
a various number of sutures to close the larger wound, and visual recovery is
often slower. Extra capsular cataract extraction usually requires an injection
of numbing medication around the eye and an eye patch after surgery
Intracapsular cataract surgery: this
surgical technique requires an even larger wound than extracapsular surgery,
and the surgeon removes the entire lens and the surrounding capsule together.
This technique requires the intraocular lens to be placed in a different
location, in front of the iris
Aphakia: (absence of the lens) is
corrected by the use of eyeglasses, contact lenses
NURSING MANAGEMENT
Nursing
Assessment
Assess knowledge level regarding
procedure
Assess the level of fear and anxiety
Determine visual limitations
Postoperative Assessment
Assess pain level
Sudden onset: maybe due to ruptured vessel or suture and may lead to
hemorrhage
Severe pain: accompanied by nausea and vomiting maybe caused by
intraocular pressure
Assess visual acuity in unoperated eye
Assess patient’s ability to ambulate
Assess patient’s level of independence
Nursing
Diagnoses
Self-care deficit related to visual
deficit
Anxiety related to lack of knowledge
about the surgical and postoperative experience
Risk for injury related to blurred
vision
Risk for infection related to trauma
to incision
Acute pain related to trauma to
incision
Nursing
Intervention
Relieving
Pain
Give medication to reduce pain as
analgesics
Give cold compression demand for
blunt trauma
Encourage to the use of sunglasses in
strong light
Vital signs must assess frequently
Physical rest in bed with backrest
elevated to provide comfort
Relieving
Anxiety
Assess the degree and duration of
visual impairment
Orient the patient to new environment
Explain the preoperative routines
Push to perform daily living habits
when able
Encourage the participation of family
Prevention
of Injury
Provided a comfortable position to
the patient
Help the patient to set the
environment
Orient the patient in a room
Discuss the need for use of goggles
when instructed
Do not put pressure over the affected
eye trauma
Used the proper procedures when
providing eye drugs
Promoting
Self-Care
Cleared the all doubts of patient
regarding the disease condition
Maintained good IPR with the patient
Provided calm cool environment to the
patient
Music therapy and pet therapy given
to patient
Relaxation therapy also provided to
relieve the anxiety of patient
Improving
Knowledge
Provided adequate knowledge about a disease
condition
Provided the sunglasses to patient
during exposure to sunlight
Provided medications to patient on
proper time
Advised the patient to talk with
doctor
Followed the recommendations that
ensure regular eye checkup by the ophthalmologist
Health Education
Advised the patient to wear
sunglasses during exposure
Advised the patient to take
analgesics to reduce pain
Advised the patient to take proper
diet
Advised the patient to take care of
eyes after surgery
Advised patient to prevent eyes from
dirt and dust
Advised patient to preventing eyes
from trauma
Advised patient to report to doctor
for early complications
Advise patient to increase activities
gradually as directed by health care provider
Caution against activities that cause
patient to strain
Instruct patient and family in proper
use of medications
Advise patient to apply plastic
shield over the eye at night to avoid accidental injury during sleep
Infirm about fitting temporary
corrective lenses for the first 6 weeks
COMPLICATIONS
Capsular rupture
Vitreous loss
Endothalemitis
Pseudoexfoliation
Myopia
After Care
Before the
patient goes home, may receive the following:
A patch to wear over eye until the
follow-up exam
Eyedrops to prevent infection, treat
inflammation, and help with healing
Wear dark sunglasses outside after
removing the patch
Wash hands well before and after
using eye drops and touching eye. Try not to get soap and water in eye when are
bathing or showering for the few days
CATARACT – Risk Factors and Etiology, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
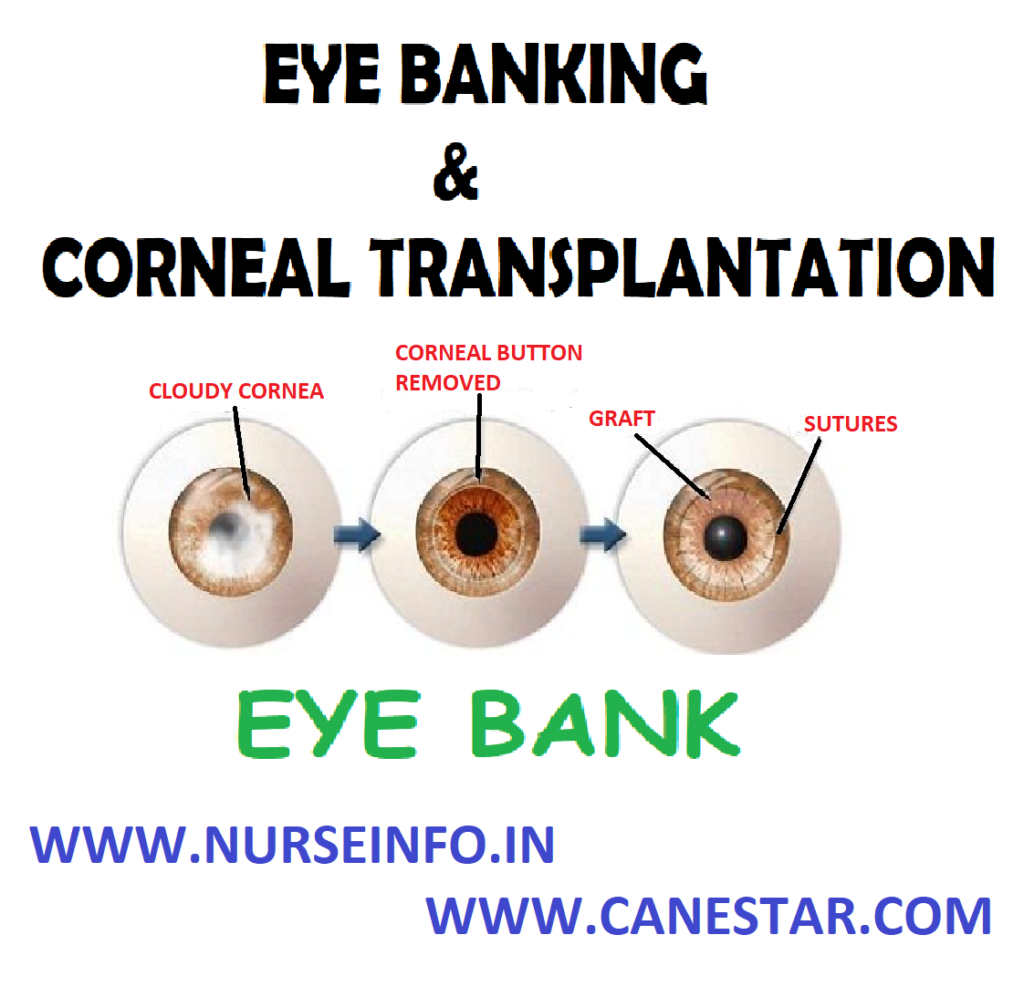
RHEUMATOID ARTHRITIS – Etiology and
Risk Factors, Pathophysiology, Clinical Manifestations, Diagnostic Evaluations
and Management
Rheumatoid
arthritis is a chronic inflammatory disorder that typically affects the small
joints in hands and feet.
It is an
autoimmune disorder, it occurs when immune system mistakenly attacks own body’s
tissues. In addition to causing joint problems, rheumatoid arthritis sometimes
can affect other organs of the body – such as the skin, eyes, lungs and blood
vessels.
ETIOLOGY AND RISK FACTORS
The causes of rheumatoid arthritis
are unknown
It is believed that the tendency to
develop rheumatoid arthritis may be genetically inherited (hereditary)
RISK FACTORS
Age: risk increases with age
Gender: women are more affected than
men
Genetic risk: there is a strong
familial link in some cases
PATHOPHYSIOLOGY
Due to any
cause —- synovitis —- increase in the lymphocytes and plasma cells —-
articular cartilage destruction —- granulation tissue grows across the surface
of cartilage (pannus) from the ending of joint —- articular surface shows
loss of cartilage beneath the expanding pannus —- inflammatory pannus causes
causes focal destruction of bones —- deformity and soft tissue swelling
CLINICAL MANIFESTATIONS
Fatigue
Anorexia
Weight loss
Stiffness
Lack of appetite
Low-grade fever
Muscle and joint aches
Specific
articular involvement is manifested
Pain stiffness limitation of motion
and signs of inflammation (heat swelling tenderness)
Extra-articular
Manifestations
Peripheral edema
Peripheral neuropathy
Myositis
Tenocynovitis
Rheumatoid vasculitis
Sjorgen’s syndrome
Amyloidosis
Fetly syndrome
COMPLICATIONS
Osteoporosis: rheumatoid arthritis
itself, along with some medications used for treating rheumatoid arthritis, can
increase the risk of osteoporosis – a condition that weakens bones and makes
them more prone to fracture
Carpal tunnel syndrome: if rheumatoid
arthritis affects wrists, the inflammation can compress the nerve that serves
most of hand and fingers
Heart problems: rheumatoid arthritis
can increase risk of hardened and blocked arteries, as well as inflammation of
the sac that encloses heart
Lung diseases: people with rheumatoid
arthritis have an increased risk of inflammation and scarring of the lung
tissues, which can lead to progressive shortness of breath
DIAGNOSTIC EVALUATION
History collection
Physical examination: check points
for swelling, redness and warmth. Also check reflexes and muscle strength
Laboratory tests
Complete blood count (CBC): people with rheumatoid arthritis
tend to have an elevated erythrocyte sedimentation rate (ESR), which indicates
the presence of an inflammatory process in the body.
Radiographic studies of joint: X-rays
help to track the progression of rheumatoid arthritis in your joints overtime
Synovial fluid analysis
TREATMENT
NSAIDs: are medications that can
reduce tissue inflammation, pain, and swelling, e.g. brufen, etc
Steroids: corticosteroids medications
such as prednisone reduce inflammation and pain and slow joint damge
Disease-modifying antirheumatic drugs
(DMARDs): these drugs can slow the progression of rheumatoid arthritis and save
the joints and other tissues from permanent damage. Common DMARDs include
methotrexate, leflunomide, hydroxychloroquine and sulfasalazine
Calcium and vitamin D supplements: to
prevent thinning of the bones due to osteoporosis
Surgical
Management
If
medications fail to prevent or slow joint damage, surgery may help to restore
ability to use joint
Rheumatoid
arthritis surgery may involve one or more of the following procedures:
Total joint replacement: during joint
replacement surgery, surgeon removes the damaged parts of joint and inserts a
prosthesis made of metal and plastic
Tendon repair: inflammation and joint
damage may cause tendons around joint to loosen or rupture. Repair the tendons
around joint
Joint fusion: surgically fusing a
joint may be recommended to stabilize or realign a joint and for pain relief
when a joint replacement is not an option
NURSING MANAGEMENT
Nursing
Diagnosis
Chronic pain related to joint
inflammation and overuse
Interventions
Perform a comprehensive assessment of
pain to include location characteristics, onset, duration, frequency, severity
Evaluate with patient and health care
team, effectiveness of past pain control measures that have been used
Reduce or eliminate the factors that
increase the pain experience (e.g. fear fatigue lack of knowledge)
Teach use of nonpharmacological
techniques (relaxation, distraction, massage)
Provide optimal pain relief with
prescribed analgesics
Impaired physical mobility related to
joint pain and stiffness
Interventions
Determine the limitations of joint
movement and affect on function to establish baseline plan of care
Collaborate with physical therapy
into establish exercises program to improve the joint function
Explain the plan and purpose of
exercises to the patient and family
Initiate pain control measures before
beginning of joint exercises (hot packs, warm shower)
Assist patient to do active, passive
joint movements (selection of proper footwear use of assistive devices)
Self-care deficit related to disease
progression, weakness
Interventions
Monitor patient’s ability for
independent self care
Monitor patients need for hygiene,
dressing, grooming, eating
Establish a routine for self-care
activities assist patient in accepting dependency needs to ensure all needs are
meet
Teach family to encourage
independence and to intervene only when patient is unable
RHEUMATOID ARTHRITIS – Etiology and Risk Factors, Pathophysiology, Clinical Manifestations, Diagnostic Evaluations and Management
OSTEOMYELITIS – Causes and Risk
Factors, Modes of Transmission, Pathophysiology, Signs and Symptoms, Diagnostic
Evaluation and Management
Osteomyelitis
is an infection of a bone caused by Staphylococcus aureus. Infection with a
fungus is a rare cause.
MODES OF TRANSMISSION
If some
bacteria settle on a small section of bone, they can multiply and cause
infection. Bacteria can get to bone:
Via the bloodstream: this is the most
cause in children. Bacteria sometimes get into the blood from an infection in another
part of the body and then travel to a bone
Following an injury: bacteria can
spread to bone if you have a deep cut on the skin. In particular, if you have a
broken bone which you can see through the cut skin
PATHOPHYSIOLOGY
Infection
from bacteria —- the initial response to infection is inflammation, increased
vascularity, and edema —- after 2 or 3 days, thrombosis of the blood vessels
occurs —- ischemia with bone necrosis —- if it is not treated properly, a
bone abscess forms —- new bone growth (the involucrum) forms and surrounds
the sequestrum —- produces recurring abscesses —- chronic osteomyelitis
CAUSES AND RISK FACTORS
Anyone at
any age can develop osteomyelitis. However, one has an increased risk if:
Have recently fractured (broken) a
bone
Have bone prosthesis (an artificial
hip, a screw in a bone following surgery, etc)
Have recently had surgery to a bone
Have a poor immune system. For
example, AIDS, taking chemotherapy, seriously ill with another disease, etc
Have had a previous episode of
osteomyelitis
Have reduced skin sensation. This can
lead to damage and infection of the skin which can spread to the blood or to
local bone. For example, some people with diabetes have reduced sensation in
their feet
Have regular kidney dialysis
SIGNS AND SYMPTOMS
Pain and tenderness over an area of
bone
A lump may develop over a bone, which
is usually very tender
Redness of overlying skin may then
develop
Feeling generally unwell with fever
(high temperature) as the infection develops
DIAGNOSTIC EVALUATION
X-ray
CT scan
MEDICAL
TREATMENT
Antibiotics
An
antibiotic is usually started as soon as possible. The initial antibiotic
chosen is one that is likely to kill the bacteria which commonly cause
osteomyelitis. However, the antibiotic is sometimes changed to a different one
when the results of the tests confirm which bacterium is causing the infection.
The symptoms may settle quite quickly after taking an antibiotic. Penicillin
and cephalosporin is the drug of choices
To control
pain you may be given painkillers
Surgical
Management
Surgery is
required if:
An abscess develops. The pus in an
abscess needs to be drained.
The infection presses on other
important structures. For example, an infection in the spine may press on the
spinal cord
The infection has become chronic
(persistent) and some bone has been destroyed. Dead and infected bone may need
to be removed to allow the infection to clear. Sometimes, plastic surgery is
needed at the same time to cover any wound to give the best chance of cure
Rarely, amputation of a foot or leg is needed if infection
persists in a leg bone
NURSING MANAGEMENT
Acute pain related to inflammation
and swelling
Assess the level of pain
The affected part may be immobilized
with a splint to decrease pain and muscle spasm
Elevation reduces swelling and
associated discomfort
Comfortable position is given
Analgesic given to treat pain
Impaired physical mobility related to
pain, use of immobilization devices, and weight-bearing limitations
Assess the normal level of activity
The joints above and below the
affected part should be gently placed through their range of motion
The nurse encourages full
participation in ADLs within the physical limitations to promote general
well-being
Analgesics are given
Deficient knowledge related to the
treatment regimen
Assess the level of knowledge by
verbalization with the patient
Answer each question of the patient
Clarify all doubts of the patient
OSTEOMYELITIS – Causes and Risk Factors, Modes of Transmission, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management
OSTEOMALACIA – Etiology, Signs and
Symptoms, Pathophysiology, Diagnostic Evaluation and Management
Osteomalacia
refers as a metabolic disease of bones, often caused by a vitamin D deficiency.
Metabolic disorder characterized by inadequate or delayed mineralization of
bone and it result from a defect in the bone-building process
ETIOLOGY
Body uses
calcium and phosphate to build strong bones. Osteomalacia may occur if bodies
do not get enough of these minerals in diet or if body does not absorb them
properly. These problems may be caused by:
Vitamin D deficiency: people who live
in areas where sunlight hours are short or eat a diet low in vitamin D can
develop osteomalacia. Vitamin D deficiency is a common cause of osteomalacia
Certain surgeries: normally, the
stomach breaks down food to release vitamin D and other minerals that are
absorbed in the intestine. This process is disrupted if one has surgery like
gastrectomy and may result in osteomalacia. Surgery to remove or bypass small
intestine also can lead to osteomalacia
Celiac disease: in this autoimmune
disorder, the lining of small intestine is damaged by consuming foods
containing gluten, a protein found in wheat, barley and rye. A damaged
intestinal lining does not absorb nutrients, such as vitamin D, as well as a
healthy one does
Kidney or liver disorders: problems
with kidneys or liver can interfere with ability to process vitamin D
Drugs: drugs used to treat seizures,
including phenytoin and Phenobarbital, can cause osteomalacia
SIGNS AND SYMPTOMS
Bone pain
Tenderness
Difficulty in changing position
Muscle weakness
Bowing of bones
Pathologic fractures
PATHOPHYSIOLOGY
Due to any
cause —- decreased level of vitamin D —- decreased absorption of calcium
and phosphorus from intestine —- serum level of calcium and phosphorus
decreases —- activate parathyroid gland —- result in less of calcium and
phosphorus from bones —- deformity of bones —- bone became soft and unable
to bear stress and weight
DIAGNOSTIC EVALUATION
Physical examination: check for
skeletal deformity like spinal kyphosis, bowed legs
Blood and urine tests: in cases of osteomalacia
caused by vitamin D deficiency or by phosphorus loss, abnormal levels of
vitamin D and the minerals calcium and phosphorus are often detected
X-ray: slight cracks in bones that is
visible on X-rays
Bone biops: during a bone biopsy,
doctor inserts a slender needle through skin and into bone to withdraw a small
piece of bone for viewing under a microscope. This procedure is done after
using a local anesthetic and takes only about a half-hour. Although a bone
biopsy is very accurate in detecting osteomalacia
MANAGEMENT
Vitamin D, phosphorus, calcium
supplements are prescribed
Exposure to sunlight is also advised
to patient (for short period of time)
Vitamin D rich diet (fortified milk
and milk products, cereals, egg, etc) is given to the patient
NURSING MANAGEMENT
Nursing
Diagnosis
Impaired physical mobility related to
decalcification and stretching of the muscles
Interventions
Encourage patient to do the daily
activities
If person is not able to perform
daily routine then assist him
Ask patient for some exercises but
also ready with some pain control measures
Provide supplements of calcium as
prescribed by the physician
Bone pain related to weakness and
stretching of muscles
Interventions
Assess the intensity, duration, onset
of the pain
Assess the measures use by the health
care time previously
Provide comfort devices
Provide medications as prescribed by
the physician
Provide psychological support and
assist while changing the position
Risk for fractures related to calcium
deficiency and muscle weakness
Interventions
Assess for any cracks on the bones
Encourage for vitamin D rich diet
Provide calcium supplements to the
patient as prescribed by physician
OSTEOMALACIA – Etiology, Signs and Symptoms, Pathophysiology, Diagnostic Evaluation and Management
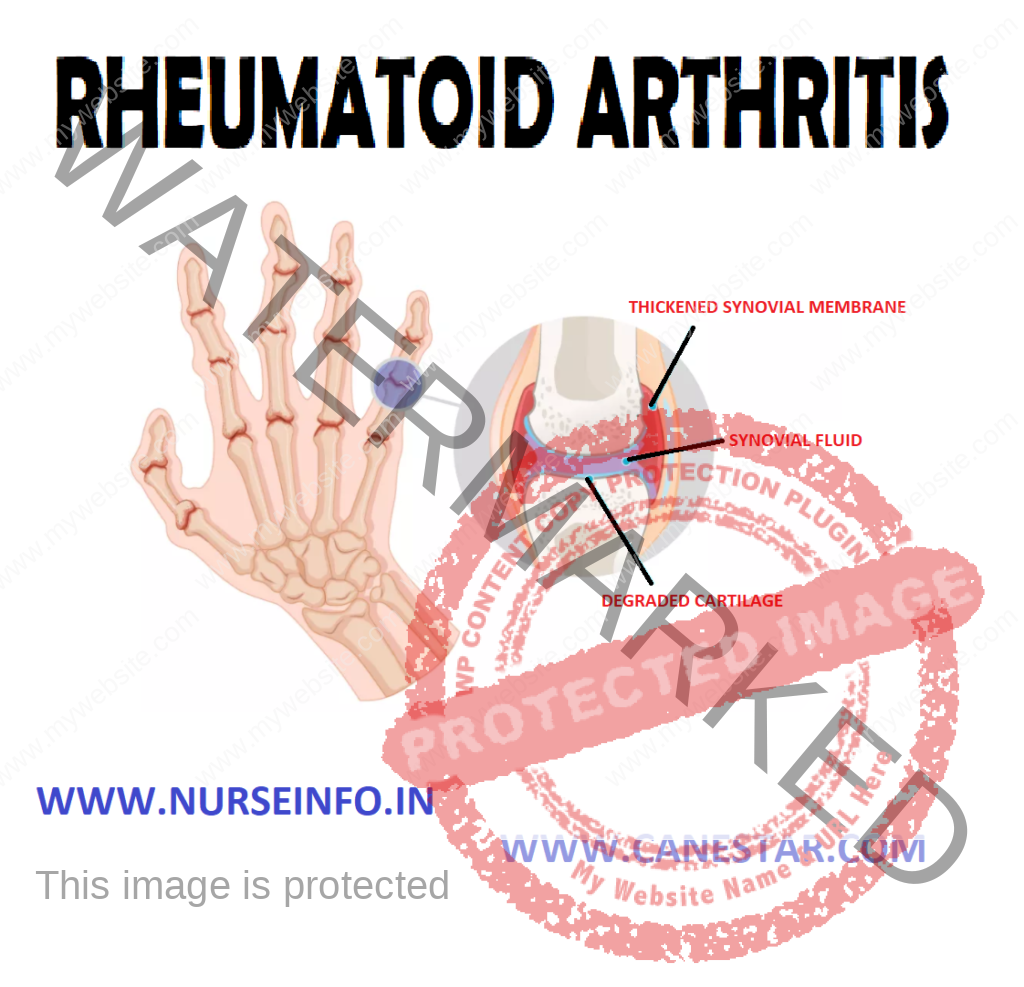
INTESTINAL OBSTRUCTION – Etiology,
Risk Factors, Types, Signs and Symptoms, Pathophysiology, Diagnostic
Evaluations and Management
Intestinal
obstruction is an interruption in the normal flow of intestinal contents along
the intestinal tract. The obstruction may occur in small intestine or colon and
can be partial or complete, may be mechanical or may be paralytic, may or may
not comprise of the vascular supply.
Intestinal
obstruction exists when there is blockage, mechanical or functional, that prevents
the normal flow of the intestinal contents through the intestinal tracts. It
can occur at any level distal to the small intestine or large intestine and is
a medical emergency
ETIOLOGY
Obstructions of the small intestine
may be caused by narrowing of the intestinal lumen as a result of inflammation,
neoplasms, adhesions, hernia, volvulus, intussusceptions, food blockage or
compression from outside the intestine
Paralytic ileus, vascular problems,
such as mesenteric embolus and thrombus, hypokalemia from diuretics or
antihypertensive agents also may result in small bowel obstructions
Cancer accounts for about 80% of
obstructions of the large intestine, with mostly occurring in the sigmoid
colon. Other causes are diverticulitis, ulcerative colitis, and previous
abdominal surgery. Factors that are caused are mechanical, neurogenic or
vascular.
RISK FACTORS
Mechanical factors: a physical block
to passage of intestinal contents without disturbing blood supply of bowel.
High small bowel, or low small bowel obstructions occur four times more
frequently than chronic obstructions. These includes:
Extrinsic
Adhesions: these fibrous bands of
scar tissue can become looped over a portion of the bowel. The loops then can
become either the focus around which the bowel can twist or the band that
mechanically obstructs the bowel by external pressure. The presence of multiple
adhesions increases the risk of obstruction
Hernia: an incarcerated hernia may or
may not cause obstruction, depending on the size of the hernia ring. However,
the potential for obstruction is always present in any hernia. A strangulated
hernia is always obstructed because the bowel cannot function when its blood
supply is cut-off.
Volvulus: volvulus is a twisting of
the bowel that commonly occurs about a stationary focus in the abdominal
cavity. It can cause infraction of the bowel and can occur in either the large
or small bowel. Volvulus sometimes can be corrected without surgical
interventions. Successful decompression of the bowel with a long tube releases
pressure against the proximal end of the loop, thus allowing bowel volvulus to
relax
Neurologic factors: neurogenic
factors are responsible for a dynamic obstruction, also called paralytic ileus,
which is caused by lack of peristaltic activity and commonly occurs after
abdominal surgery. Extensive surgical procedures in the bowel and in the
retroperitoneal area may cause a postoperative neurologic problem. Treatment
involves aspiration of secretions by NG suction until the bowel begins to function
Vascular factors: when the blood
supply to any part of the body is interrupted, the part ceases to function and
pain occurs. Blood is supplied by way of the celiac and superior and inferior
mesenteric arteries. These vessels have autosomotic intercommunications at the
head of the pancreas and along the transverse bowel. Obstruction of blood flow can
arise as a result of complete occlusion (mesenteric infarction) or partial
occlusion (abdominal angina).
Intraluminal: foreign body, fecal or
barium impaction, polyp, gallstones, meconium in infants. In postoperative
patients, approximately 90% of mechanical obstructions are due to adhesion.
Other Causes
Spinal cord injuries, vertebral
fractures
Postoperatively after any abdominal
surgery
Peritonitis, pneumonia
Wound dehiscence
GI tract surgery
Strangulation – obstruction comprises
blood supply, leading to gangrene of the intestinal wall, caused by the
prolonged mechanical obstruction
TYPES
It is a
series that depends on the region of bowel that is affected, the degree to
which the lumen is occluded and the degree to which the blood circulation in
the bowel wall is disturbed. Treatment involves aspiration of the secretion
which involves aspiration of the secretion by gastric suction until the bowel
begins to function
Partial occlusion
Complete occlusion
Complete
Occlusion: an occlusion of arterial blood supply to the bowel as in mesenteric
thrombosis effectively stops bowel function. The usual cause is an embolus. The
extent of the resulting symptoms is determined by:
Size of the vessels that is occluded
The length of the bowel that is
without a supply of blood
The rapidity with which the occlusion
occurs
SIGNS AND SYMPTOMS
Crampy pain that is wave-like and
colicky in character
The patient may pass blood and mucus
but no fecal matter and no flatus
Vomiting
Obstruction
Crampy, lower abdominal pain
Fecal vomiting
Shock
Constipation
Abdominal distension
DIAGNOSTIC EVALUATION
X-ray studies: abdominal X-ray will
show abnormal qualities of gas or fluid in the bowel.
Lab studies: complete blood cell
count, electrolytes, and blood urea nitrogen will reveal dehydration and loss
of plasma volume and possibly infection. An elevated WBC count will indicate
strangulation or perforation
Hematocrit: this will indicate
hemoconcentration, decreased hemoglobin and HCT values indicate bleeding from
neoplasm or strangulation with necrosis. Increased BUN will indicate
dehydration, stool to be checked for occult blood
PATHOPHYSIOLOGY
Due to any
mechanical or nonmechanical cause —- intestinal content, fluid and gas
accumulate above the intestine —- the abdominal distension and retention of
fluid reduce the absorption of fluids and stimulate more gastric emptying —-
with increasing distension, pressure within the intestinal lumen increases,
causing a decrease in venous and arteriolar capillary pressure —- this causes
edema, congestion, necrosis, and eventual rupture or perforation of intestinal
wall, with resultant peritonitis —- this may lead to vomiting due to
abdominal distention —- vomiting may lead to loss of hydrogen ions and
potassium from the stomach, reduction of chlorides and potassium in blood and
metabolic alkalosis —- excessive loss of water leads to acidosis and that all
results in small bowel obstruction
MANAGEMENT
Assessment
Assess the signs and symptoms of
abdominal pain, indigestion, nausea and vomiting
Take the history of prolonged
constipation and complaint of dysphagia and abdominal pain
Assess for the diagnostic studies of
the radiography of the flat and upright abdomen.
Assess for the abdominal distension
through bowel sounds
Decompression
of the bowel through a nasogastric tube by the removal of gas, and fluid,
correction and relief of the obstruction
Decompression
of the bowel is done by inserting the NG tube or intestinal tube
Surgical
Management
Surgical
management involves resection of the obstructed segment of bowel anastomosing
the remaining healthy bowel. Partial or total colectomy, colostomy or ileostomy
may be required when extensive obstruction or necrosis is present, e.g. hernia
and adhesions.
Nonsurgical
Treatment
Introducing colonoscope for the
removal of polyps, dilated strictures, and removing necrotic tumors with laser
Correction of fluid and electrolyte
imbalances with normal saline or Ringer’s solution with potassium as required
NG suction to decompress bowel
Treatment of shock and peritonitis
TNP may be necessary to correct
protein deficiency from chronic obstruction, paralytic ileus, or infection
Analgesics and sedatives, avoiding
opiates due to GI mobility inhibition
Ambulation for the patients with paralytic
ileus to encourage return of the peristalsis
NURSING MANAGEMENT
Nursing
Diagnosis
Ineffective breathing pattern related
to abdominal distension, interfering with normal lung expansion
Acute pain related to obstruction,
distension and strangulation
Risk for fluid deficit volume related
to impaired fluid intake, vomiting, and diarrhea from intestinal obstruction
Risk for electrolyte imbalance
related to suctioning
Diarrhea related to obstruction
Risk of injury related to
complication and severity of illness
Fear related to life-threatening
symptoms of intestinal obstruction
Ineffective breathing pattern related
to abdominal distension, interfering with normal lung expansion
Interventions
Keep the patient in Fowler’s position
to promote ventilation
Provide oxygenation to the patient
Monitor ABG level for oxygenation to
decompress
Acute pain related to obstruction,
distension and strangulation
Interventions
Provide supportive care during NG
intubation to assist with discomfort
To relieve air-fluid syndrome, turn
the patient from supine to prone position every 10 minutes until enough flatus is
passed to decompress the abdomen
A rectal tube may be indicated
Administer prescribed analgesics
Risk of fluid deficit volume related to
impaired fluid intake, vomiting and diarrhea from intestinal obstruction
Interventions
Measure and record all intake and
output
Administer IV fluid and parental
nutrition as prescribed
Monitor electrolytes, urine analysis,
haemoglobin and blood cells count and report any abnormalities
Monitor renal output to assess the
renal function and to detect urine retention due to bladder compression by the
distended intestine
Monitor vital signs, a drop in BP may
indicate decrease circulatory volume due to blood loss from strangulated hernia
Risk for electrolyte imbalance
related to suctioning
Interventions
Monitor electrolyte values to
identify imbalances
Monitor vital signs and watch for
signs of electrolyte for imbalances such as weakness accompanied by low
potassium levels to identify imbalances for prompt treatment
Give ice chips sparingly if ordered
by the physician, melted ice increases electrolyte and hydrochloric acid
removal when suctioned from the stomach, and electrolyte imbalance and
metabolic alkalosis occur
Diarrhea related to obstruction
Interventions
Collect stool sample for test for
occult blood if occur
Maintain adequate fluid balance
Record and amount of consistency of
stools
Maintain NG tube as prescribed to
decompress bowel
Fear related to life threatening
symptoms of intestinal obstruction
Interventions
Recognize the patient’s concerns and
initiate measures to provide emotional support
Encourage the presence of support
person
COMPLICATIONS
Dehydration due to loss of water,
sodium and chloride
Peritonitis
Shock due to loss of electrolyte and
dehydration
Death due to shock
HEALTH EDUCATION
Explain the rational for NG suction,
NPO status, and IV fluids initially. Advise the patient to progress diet slowly
as tolerated once home
Advise plenty of rest and slow
progression of activity as directed by surgeon or other health care provider
Teach wound care, if indicated
Encourage the follow-up directed and
to call surgeon or health care provider, if increasing abdominal pain,
vomiting, or few occur prior to follow-up
INTESTINAL OBSTRUCTION – Etiology, Risk Factors, Types, Signs and Symptoms, Pathophysiology, Diagnostic Evaluations and Management
CROHN’S DISEASE – Etiology, Types, Pathophysiology,
Signs and Symptoms, Diagnostic Evaluation and Management
Crohn’s
disease is a chronic idiopathic inflammatory disease that can affect any part
of GI tract, usually the small intestine and large intestine that characterized
by ulceration, swelling and scarring of the part of intestine. It is also known
as regional enteritis
ETIOLOGY
IBD is most
commonly begins during adolescence and early adulthood (usually between the
ages of 15 and 35). There is a small second peak of newly diagnosed cases after
age 50. Although the reason for this is not completely understood
The exact cause of Crohn’s disease is
unknown
Family history of inflammatory bowel
disease
Immune system problems: for some
reason, people with Crohn’s disease have an immune system that reacts
inappropriately
Genetics: brothers, sisters, children
and parents of person with IBD, including Crohn’s disease, are slightly more
likely to develop the disease themselves
Environmental factors: environmental
factors may help trigger Crohn’s disease. Associated environmental factors may
include any of the following:
Substances from something you have seen
Microbes such as bacteria or viruses
Cigarette smoke
Other substances that are yet unknown
TYPES
Crohn’s colitis
Crohn’s enteritis
Crohn’s terminal ileitis
Crohn’s enterocolitis and ileocolitis
Crohn’s colitis is inflammation that is confined to the
colon. Abdominal pain and bloody diarrhea are the common symptoms. Anal
fistulae and perirectal abscesses can also occur.
Crohn’s enteritis refers to inflammation confined to the
small intestine (the first part, called the jejunum or the second part, called
the ileum). Involvement of the ileum alone is referred to as Crohn’s ileitis.
Abdominal pain and diarrhea are the common symptoms. Obstruction of the small
intestine can also occur.
Crohn’s terminal ileitis is inflammation that affects only
the very end of the small intestine (terminal ileum), the part of the small
intestine closest to the colon. Abdominal pain and diarrhea are the common
symptoms. Small intestinal obstruction can also occur.
Crohn’s enterocolitis and ileocolitis are terms to describe
inflammation that involve both the small intestine and the colon. Bloody
diarrhea and abdominal pain are the common symptoms. Small intestinal
obstruction can also occur.
PATHOPHYSIOLOGY
In the early
stages, Crohn’s disease causes small, scattered, shallow, crater-like
ulcerations (erosions) on the inner surface of the bowel —- these erosions
are called aphthous ulcers. This erosion becomes deeper and larger, ultimately
becoming true ulcers (which are deeper than erosions) —- it will cause
scarring and stiffness of the bowel —- as the disease progresses, the bowel
becomes increasingly narrowed, and ultimately can become obstructed —- deep
ulcers can puncture holes in the wall of the bowel, and bacteria from within
the bowel can spread to infect adjacent organs and the surrounding abdominal
cavity —- narrowing of the small intestine to the point of obstruction —-
when the intestine is obstructed, digesting food, fluid and gas from the
stomach and the small intestine cannot pass into the colon —- the symptoms of
small intestinal obstruction then appear, including severe abdominal cramps,
nausea, vomiting and abdominal distension
SIGNS AND SYMPTOMS
Common
symptoms of Crohn’s disease include abdominal pain, diarrhea, and weight loss.
Less common symptoms include poor appetite, fever, night sweats, rectal pain,
and occasionally rectal bleeding. The symptoms of Crohn’s disease are dependent
on the location, the extent, and the severity of the inflammation.
Swelling of the tissue of the anal
sphincter, the muscle at the end of the colon that controls defecation
Development of ulcers and fissures
(long ulcers) within the anal sphincter. These ulcers and fissures can cause
bleeding and pain with defecation
Development of anal fistulae
(abnormal tunnels between the anus or rectum and the skin surrounding the
anus). Mucus and pus may drain from the openings of the fistulae on the skin.
Development of perirectal abscesses
(collections of pus in the anal or rectal area). Perirectal abscesses can cause
fever, pain and tenderness around the anus.
DIAGNOSTIC EVALUATION
The
diagnosis of Crohn’s disease is suspected in patients with fever, abdominal
pain and tenderness, diarrhea with or without bleeding, and anal diseases
Laboratory blood tests may show
elevated white blood cell counts and sedimentation rates, both of which suggest
infection or inflammation
Other blood tests may show low red
blood cell counts (anemia), low blood proteins, and low body minerals,
reflecting loss of these minerals due to chronic diarrhea
Colonscopy: it is more accurate than
barium X-rays in detecting small ulcers or small areas of inflammation of the
colon and terminal ileum. Colonoscopy also allows for small tissue samples to
be taken and sent for examination under the microscope to confirm the diagnosis
of Crohn’s disease. Colonscopy also is more accurate than barium X-rays in
assessing the degree (activity) of inflammation
Computerized axial tomography (CAT)
or (CT): scanning is a computerized X-ray technique that allows imaging of the
entire abdomen and pelvis. It can be especially helpful in detecting abscesses
Video capsule endoscopy (VCE): VCE
has also been added to the list of tests for diagnosing Crohn’s disease. For
video capsule endoscopy, a capsule containing a miniature video camera is
swallowed. As the capsule travels through the small intestine, it sends video
images of the lining of the small intestine to a receiver carried on a belt at
the waist. The images are downloaded and then reviewed on a computer.
Stool specimens: mainly composed of
mucus, blood, pus and intestinal organisms, especially Entamoeba histolytica
(active stage). Fecal leukocytes and RBCs indicate inflammation of GI tract.
Stool positive for bacterial pathogens, ova and parasites or clostridium
indicates infections. Stool positive for fat indicates malabsorption
Barium enema: may be performed after
visual examination has been done, although rarely done during acute, relapsing
stage, because it can exacerbate condition.
Electrolytes: decreased potassium,
magnesium and zinc are common in severe diseases
COMPLICATIONS
Bowel strictures
Nutritional deficiencies
Loss of weight
Anemia
Growth retardation
Delayed puberty
Formation of fistulas
Massive intestinal bleeding
MANAGEMENT
The aim of
the management is
To understand the natural history and
prognostic factors of Crohn’s disease
To understand when to use early
combination therapy with an anti-TNF agent and immunomodulator in moderate to
severe Crohn’s patients.
To understand the side effects of
anti-TNF therapy
To understand when to administer
appropriate vaccinations to inflammatory bowel disease patients both before and
during immunosuppressive therapy
MEDICAL MANAGEMENT
Immunosuppressant – to reduce the
inflammation. This drug includes:
Azathioprine
Cyclosporine
Infliximab
Tacrolimus
Mycohenoate mofetil
Aminosalicylates (oral)
Olsalazine: antibacterial action
Balsalazine
Mesalamine
Corticosteroids (oral)
Prednisolone
Prednisone
Corticosteroids (rectal)
Hydrocortisone intrarectal form
Retention enema
Immune Modifiers
9-mercaptourine
Azathioprine
Cyclosporine
Monoclonal antibodies
Infiximab reduces inflammation
Antibiotics
Metronidazole IV
Ciprofloxacin
These drugs
are helpful to reduce harmful intestinal bacteria and suppress the intestine’s
immune system
Iron supplements should also be
prescribed to restore the iron level to normal
Surgical
Management
Surgery
plays important but different roles in management of Crohn’s disease and
ulcerative colitis. Surgery is indicated for patients whose disease is
refractory to medical therapy and for the management of complications. It plays
a curative role in ulcerative colitis
Surgical
intervention is avoided whenever possible in Crohn’s disease because of high
rates of recurrence of disease process in the same area. Surgical approaches to
Crohn’s disease focus on sparing and conserving as much of the bowel as possible,
particularly when the small bowel is involved
DIETARY RECOMMENDATIONS
Eat regularly, do not skip meals.
Empty bowels produce gas
When adding new food to your diet,
try a little bit with other foods you know will be easy to digest
Small, frequent meals are best,
always chew thoroughly
Rice, potatoes, or pasta once daily
may reduce bowel frequency and irritation
High potassium foods will help offset
the side effects of diarrhea
Limit foods containing simple sugars.
They aggravate diarrhea
The
following are potential anal irritants:
Coconut
Dried fruits (raisins, figs)
Foods with seeds or nuts
Raw fruits (oranges, apples)
Raw vegetables (celery, corn,
coleslaw)
Spicy foods
NURSING MANAGEMENT
The goal of
nursing management is:
To control the inflammatory process
To relieve symptoms
To correct metabolic and nutritional
problems and promote healing
To achieve the previous health status
Nursing
Diagnosis
Diarrhea related to inflamed
intestinal mucosa
Deficit fluid volume related to
diarrhea
Chronic pain-related inflammatory
disease of small intestine
Imbalanced nutrition less than the
body requirement related to pain
Ineffective coping related to feeing
of rejection
Diarrhea related to inflamed
intestinal mucosa
Interventions
Anti-diarrheal medications are
commonly used to treat diarrhea
Nurse monitors the number and
consistency of stools
Perineal area must be clean with
antiseptic solution and then with water
Perineal area must be clean in every
evacuation
Report reduction in frequency of
stools, return to more normal stool consistency
Identify and avoid contributing
factors
Promote bed rest, provide bedside
commode
Deficit fluid volume related to
diarrhea
Interventions
Monitor intake and output chart
Provide fluids as prescribed by the
doctor to maintain hydration
Monitor electrolytes and acid base
balance because diarrhea can lead to metabolic acidosis
Watch for cardiac dysrhythmias and
muscular weakness due to loss of electrolytes
Chronic pain-related inflammatory
disease of small intestine
Interventions
Administer medications for control of
inflammatory process as prescribed
Observe and record changes in pain,
frequency, location, characteristics, precipitating events and duration
Monitor for distension, increased
temperature, hypotension and rectal bleeding – all signs of obstruction due to
inflammation
Clean the rectal area and apply
ointments as necessary to decrease discomfort from skin breakdown
Prepare the patient for surgery if
response to medical and drug therapy is unsatisfactory
Imbalanced nutrition less than the
body requirement related to pain
Interventions
Encourage a diet that is low in
residue fiber and fat and high in calories, protein and carbohydrates with vitamin
and mineral supplements
Monitor weight daily
Provide small frequent feeding to
prevent distension
Have the patient participate in meal
planning to encourage compliance and increased knowledge
Ineffective coping related to feeling
of rejection
Interventions
Offer understanding concern and
encouragement
Facilitate supportive psychological
counseling, if appropriate
Encourage the patients usual support
by people to be involved in management of disease
Encourage health-promoting behavior
HEALTH
EDUCATION
Provide comprehensive education about
anatomy and physiology of GI system, the chronic disease process, drug therapy,
potential complications and potential surgery
Instruct patient about all prescribed
medications including the purpose, dosage and adverse effects
Encourage regular follow-up and
report signs of complications
Increasing abdominal distension
Cramping pain
Diarrhea, malaise, fever
Explain the importance of adequate
hydration and nutrition monitoring weight
Encourage the patient to participate
in stress-reducing activities, such as exercise, relaxation techniques, music
therapy
For further information and support
Information about IBD must be given
in a way that promotes positivity and reassurance
Nutrition and dietary considerations
need to be discussed
If the patient is on medications,
instruct regarding the dose, when and how to take the drug, why it is ordered
and also about the side effects
Instructions regarding the daily care
provided if patient has an ileostomy or colostomy
Encourage regular follow-up and to
report signs of complications
Encourage the patient to participate
in stress-reducing activities, such as exercise, relaxation techniques, etc
CROHN’S DISEASE – Etiology, Types, Pathophysiology, Signs and Symptoms, Diagnostic Evaluation and Management