CHILDHOOD AUTISM – Definition and General Characteristics
The term
autism denotes a state of absorption into ones own world of phantasy with loss
of contact with the reality. Reported incidence of childhood autism is 2-5/10,000
live births.
Childhood autism was originally described by
Leo Kanner in 1943 as Early Infantile Autism. Autistic aloneness, language
abnormality and restricted and compulsive behavior are the main three features
of this disorder. Boys are more affected than girls. The disorder is unmasked
by the third year of life. The child is abnormally quiet, lacks the usual
emotional warmth and likes to be left alone. Eye-to-eye contact is avoided. He does
not communicate through conversation. Pronouns are reversed. ‘You’ is used to
mean ‘I’ Echolalia is common. Words and behavior are stereotypic. The child is
fond of sameness in everything. Bizarre behavior such as rocking, whirling the
head and flapping of hand may be present. Impulsive violence is common. The
arithmetic skill is relatively high. IQ may be around 70 in most cases. Some have
normal IQ. Many cases may be attributable to birth trauma. Autism is strongly a
genetic disorder, and probably arises from multiple genetic defects. Recurrence
within families with one affected child is high.
There is no specific treatment. Antipsychotics are given to control violence and hyperactivity. Behavior therapy may be helpful. Parents are to be counseled regarding management of the child at home. Many improve spontaneously and may be able to attend normal school. A few may require training in special schools. Some require special residential care.
CHILDHOOD AUTISM – Definition and General Characteristics
CHIKUNGUNYA – Etiology, Distribution and Incidence, Transmission and Epidemiology, Clinical Features, Course and Prognosis, Diagnosis, Treatment, Prevention and Control
General Characteristics
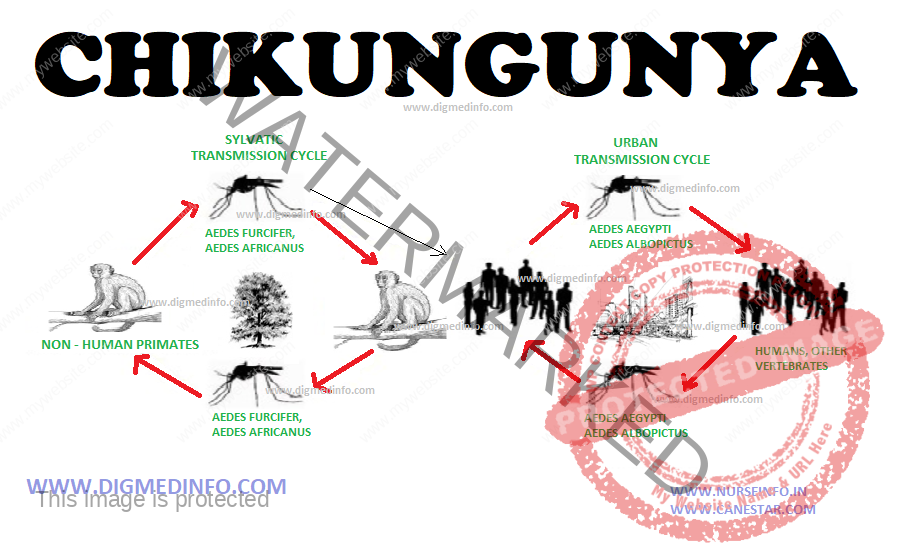
Chikungunya
(CHIK) fever is an acute infective disease, characterized by symmetric
polyarthropathy, fever, rash, and rarely, generalized hemorrhages and CNS
symptoms. The disease derives its name from the sudden onset of severe joint
pain, which cripples the victim. The disease was first described in 1955 following
an outbreak in Africa in 1952.
Etiology
CHIK virus
is an alphavirus in the Semliki Forest complex (Togaviridae) and most closely
related to o’nyong nyong(ONN) virus.
Distribution and Incidence
CHIK is
widely distributed in Africa, the middle east, and Asia. The disease has now
become endemic in several parts of India. In recent years as extensive epidemic
affected several African and Asian countries, affecting millions of people. It
is possible that the original virus has undergone genetic mutation.
Transmission and Epidemiology
In India,
Aedes aegypti mosquito is the main vector. Aedes albopictus is also implicated.
In Africa there is a sylvian cycle involving forest mosquitoes, humans and
possibly other mammals. In Asia, sylvatic viral reservoirs have not been
defined.
CLINICAL FEATURES
The
incubation period varies from 2-10 days, usually 3-7days. The onset is sudden
with abrupt fever (above 40oC), chills and rigor, headache, body pains and joint pains. There may be mild
conjunctivitis, pharyngitis an erythematous rash over the body and face. The
joints may be so inflamed that normal activities, standing and walking become
painful. Arthropathy is symmetric, affecting the extremities and less often the
shoulders and hips. Definite joint effusion is seen in 10% of cases. Small joints
of the hands and feet and major joints of the lower limbs are affected most.
Pain may be excruciating, crippling the patient quite out of propotion to the
general disability. Fever and joint pains persist for up to six days after
which they subside. Residual arthropathy lasting for months may occur in up to
30% of adults; especially in elderly patients. Morning stiffness and pain may
persist for even a few months. Pre-exsisting joint problems and neurological
disorders considerably worsen the disability and delay recovery. Joint pains
are milder and may be even entirely absent in children.
A faint
maculopapular rash may appear concurrently with defervescence. Complications
such as hyperpyrexia, hemorrhagic manifestations, encephalitis, polyneuropathy
of the Guillain-Barré type and ECG chages suggestive of myocarditis were
recorded in the Madras outbreak. Hyperpyrexia caused death in one patient.
Among asymptomatic subjects 38.4% showed hemagglutination (HI) antibodies to
chickungunya virus, confirming the presence of the virus in the community.
Hemorrhagic
manifestations occur occasionally. CNS manifestations like meningism,
convulsions and acute polyneuropathy has been reported in a minority of patients,
especially children and infants.
Course and Prognosis
The diseases
many run a benign course with slow recovery even if untreated. Arthropathy may
persist for varying periods and can be disabling. The acute illness in children
and infants and elderly persons can be fatal. The primary role of uncomplicated
chickungunya as a cause of death is not established. It produces considerable
morbidity and impairment of the quality of life for prolonged periods.
Diagnosis
Routine
laboratory investigations are not specific. The ESR may be elevated to 20-50
mm/hr and CRP may also be elevated. Isolating the virus or identifying genomic
products by PCR in acute phase blood specimens can confirm the diagnosis.
Serologically specific IgM or other antibodies can be demonstrated by IgM
capture ELISA test. This test will distinguish the condition form dengue which
is also transmitted by the same vector.
Treatment
Rest and
symptomatic treatment with non-steroidal anti-inflammatory drugs give relief.
Prolonged arthropathy demands symptomatic treatment. Chloroquine given in a dose
of 250 mg od or bd has been reported to be useful. In any case results are not
impressive.
Prevention and Control
An experimental live attenuated vaccine has been shown to produce high levels of neutralizing antibody in human volunteers but efficacy has not been tested. Anti-mosquito measures and personal protection with mosquito repellants will reduce the spread.
CHIKUNGUNYA – Etiology, Distribution and Incidence, Transmission and Epidemiology, Clinical Features, Course and Prognosis, Diagnosis, Treatment, Prevention and Control
CANDIDIASIS – General Characteristics, Diagnosis and Treatment
General Characteristics
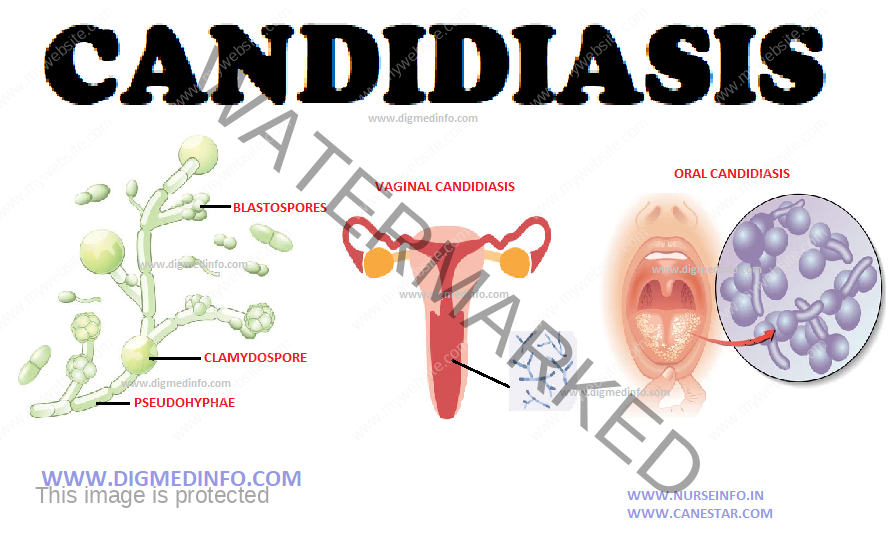
Candida
albicans is a common inhabitant of the oropharyngeal, genital and intestinal
cavities of man. Candidiasis is infection by Candida albicans. In most of the cases
it remains as a local infection affecting the skin or mucous membranes of the
mouth or genitalia. In the mouth it presents as oral thrush which is seen at
the extremes of ages, those on antibiotic therapy or in immunosuppressed
individuals. In the genitalia it usually presents as vulvovaginitis in diabetic
women who are not well-controlled. Cutaneous candidiasis usually affects the intertriginous
areas.
Systemic
candidiasis occurs in immunocompromised individuals and in drug addicts who
share needles. The fungus becomes invasive and spreads through the blood stream
to produce several lesions.
2. Widely
disseminated: Associated with septicemia (candidemia). In disseminated
candidiasis also the main targets of attack are the kidneys, brain, liver,
gastrointestinal tract, eye (endophthalmitis) and heart valves.
Extensive,
recurrent and persistent oropharygeal and esophageal candidiasis is a common
AIDS associated infection.
Diagnosis
The organism
can be demonstrated microscopically by examining samples from local lesion. In
tissues, PAS staining or methenamine silver staining reveals the organism.
The fungus
can be grown in Sabouraud’s medium. Antibodies to Candida can be detected by
ELISA or immunodiffusion. The candidal antigen can be demonstrated by ELISA or
radioimmunoassay.
Treatment
Amphotericin
B, fluconazole, ketoconazole and itraconazole are all effective in appropriate
dosage to control the systemic infection. Local surgical therapy should be
aimed at removal of the source of infection.
Dose:
Amphotericin B up to 50 mg/day IV for 1-2 weeks and more.
Fluconazole
400 mg/day.
Ketoconazole
400 mg/day for several weeks.
Itraconazole
200-400 mg/day.
Itraconazole and fluconazole are less adrenosuppressive compared to ketoconazole. Superficial skin and mucous membrane lesions respond well to nystatin ointment or nystatin mouth washes. Fluconazole given orally is very effective to cure vaginal candidiasis.
CANDIDIASIS – General Characteristics, Diagnosis and Treatment
BRONCHIAL ASTHMA – General Characteristics, Pathology, Clinical Features, Diagnosis, Treatment and Prevention
General Characteristics
The term
‘asthma’ in Greek means ‘breathless’ or ‘breathe with open mouth.’ Asthma is a
common chronic inflammatory condition of the airways whose mechanism is not
completely understood yet. Epidemiological studies suggest that multiple
genetic and environmental factors contribute to the causation of asthma, a
clinical condition that is viewed as a cluster of related disorders. Genetic
factors contribute to the variability with regard to age of onset, sensitivity of
environmental causes and response to treatment.
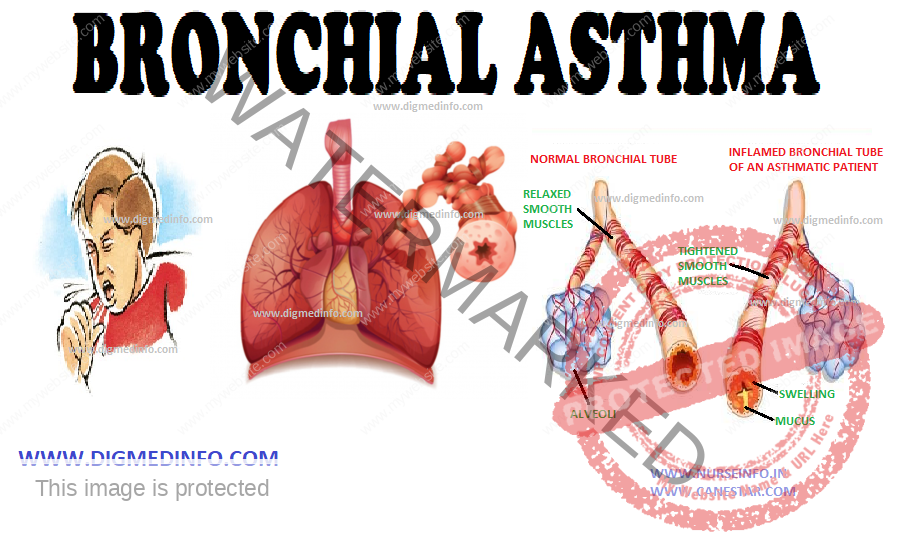
Airway
inflammation is associated with airway hyperresponsiveness, airflow limitation,
and respiratory symptoms. Airway inflammation leads to limitation of airflow by
acute bronchoconstriction, edema of the airway wall, formation of mucus plugs,
and airway remodelling.
The
tracheobronchial tree reveals increased responsiveness to immunological and
non-immunological factors. Several organic dusts, fumes, and chemicals precipitate
immunological mechanisms. Non-immunological stimuli include thermal, chemical
or psychological factors.
Bronchial
asthma used to be classified into the extrinsic (atopic) and intrinsic (cryptogenic)
types. In the former an external precipitating factor is identifiable, whereas
in the latter, it is not. The antigens include ingested, inhaled or
parenterally administered substances.
The serum of
such individuals may show elevated levels of specific antibodies belonging to
the IgE and sometimes IgG classes. Persons developing extrinsic asthma have other
atopic manifestations like eczema. The dermatological and respiratory
manifestations show a see-saw relationship. In many cases family history of
bronchial asthma may be present. Extrinsic asthma generally sets in by the age
of 10-15 years. This type has a better prognosis from the point of response to
therapy and mortality. The age of onset for intrinsic asthma is after 30 years.
Precipitating causes or raised antibody levels are not evident but these
patients show a higher frequency of eosinophilia, aspirin sensitivity, and
nasal polyposis. Common stimuli which precipitate extrinsic asthma are inhaled
allergens like house dust, pollens, fungi, animal hairs, insect scales and
industrial fumes, and foods and drugs which are consumed in day-to-day life.
Once sensitization occurs, these antigens release chemical mediators from the
mast cells by interacting with the IgE molecules on their surface. Type I
hypersensitivity reaction ensues. Asthma can also be caused by Type III
(delayed) hypersensitivity mechanism mediated by IgG. In some individuals both
Type I and Type III reactions occur, the former leading to an immediate
asthmatic paroxysm and the latter leading to a delayed episode.
Exercise-induced
asthma is a problem in children and young adults, in which bronchoconstriction
is provoked by various forms of exercise such as running or climbing stairs,
but others such as swimming may not do so. Provocation of bronchoconstriction
by cold inspired air is a possibility in such cases. In many cases the attacks are
brought on straight by the exercise, but in the others asthma sets in several
hours after the exercise. The mechanism is a Type I hypersensitivity reaction.
Short acting β2-agonists are used to prevent exercise- induced asthma. Inhaled
steroids are indicated and are useful. Systemic steroids are seldom necessary.
PATHOLOGY
Inflammation
of the airways is brought on by several factors. Eosinophils, T-lymphocytes
(CD4+), macrophages and mast cells infiltrate the bronchial wall. The
epithelium is vacuolated and the ciliated cells desquamate. Several cellular
factors play their roles in the inflammatory process. Neuropeptides such as
bradykinins, substance P and neurotensin A lead to bronchoconstriction and excessive
secretion of mucus.
The main
chemical transmitters, which alter the airways, are histamine, prostaglandin
and leukotrienes. These lead to contraction of bronchial muscle, increase in vascular
permeability and excessive secretion of abnormal mucus. Airway inflammation
persists for several years. Its severity correlates with the severity of
asthma. Hyperresponsiveness of the inflamed airways is aggravated by autonomic
and neural mechanisms. The final result is obstruction of the small and medium
sized airways brought about by mucosal edema, tenacious mucus and
bronchoconstriction.
CLINICAL FEATURES
The attacks
start with dyspnea (often at rest), expiratory wheeze, and cough. The onset is abrupt
in most cases. These attacks may occur seasonally or during all times of the
year (perennial asthma). The attacks may last for several hours if untreated.
Severity of the paroxysm varies. In the moderately severe case the patient is
orthopneic and cyanosed, and the accessory muscles of respiration are active.
There may be ineffective cough with only very scanty and tenacious mucoid
expectoration. The asthmatic paroxysm in many individuals is ushered in by a
bout of coughing and sneezing on exposure to the allergen. The pulse is rapid.
Blood pressure is normal or elevated. In severe cases pulsus paradoxus may occur. Expansion of the
chest is considerably diminished, often to less than 2 cm during the attack.
The diagnostic feature of bronchial asthma is the presence of expiratory wheeze
heard all over the chest.
DIAGNOSIS
Diagnosis of
bronchial asthma is clinical. The history of sudden attack of paroxysmal
dyspnea, cough, and the auscultatory hallmark of expiratory wheeze heard all
over the chest are diagnostic. Long duration of complaints, history of allergy,
and positive family history are other helpful clinical points.
Clinical
features which indicate severe ventilatory Impairment
1. Inability
to narrate history continuously or severe distress even on mild exertion,
2. Cyanosis,
flapping tremors,
3. Mental
confusion,
4.
Respiratory rate above 25/minute,
5. Heart
rate persistently above 110/minute.
6.
Inspiratory fall in blood pressure exceeds 16 mm Hg,
7. PEFR less
than 40% of predicted value, and
8. Feeble
breath sounds.
Differential diagnosis:
Bronchial
asthma has to be differentiated from other causes of paroxysmal dyspnea. These
include chronic bronchitis emphysema syndrome (CBES), acute left-sided heart
failure, acute bronchitis, tropical pulmonary eosinophilia, metabolic acidosis,
and tracheal obstruction by foreign bodies or tumours.
It is
important to distinguish left-sided heart failure (cardiac asthma) from
bronchial asthma. Left-sided heart failure complicates valvular heart disease,
systemic hypertension or ischemic heart disease. It causes paroxysmal dyspnea
in the first half of the night whereas bronchial asthma is more common in the
early hours of the morning.
In bronchial
asthma there is generalized wheeze all over the chest, whereas in cardiac
failure, basal crepitations are more prominent, though generalized bronchospasm
may also be evident at times. In heart failure, gallop rhythm may be evident.
Careful search for the underlying disease may reveal the etiology.
TREATMENT
Treatment
may be described under three heads: (1) treatment of the acute attack; (2)
treatment in between attacks; and (3) treatment of acute severe asthma.
TREATMENT OF THE ACUTE ATTACK
At present
the drugs of choice employed to stop an acute attack are beta 2-agonist drugs.
They act mainly on the bronchial muscle as relaxants without much effect on the
cardiovascular system. These include salbutamol, terbutaline, salmeterol,
bambuterol and others. These can be given orally, as inhalations (aerosol or
powder) or parenterally. The oral dose is effective within 15-20 minutes and
the action lasts for 4-6 hours.
Nebulizers,
which can be carried by the patient or operated in the emergency room, are
available for administration of these drugs. These can deliver larger doses as required.
The drug solution is nebulized by passing oxygen or air under pressure through
it.
PREVENTION
It is
important to avoid known allergens, which can be identified. In the case of
some allergens like house dust and pollen, desensitization can be achieved by
repeated challenges.
Inhaled
corticosteroids 200-800 micro g per day has been recommended as the treatment
of choice for regular preventive therapy of asthma.
Yoga and controlled breathing exercises are of considerable benefit in allaying the paroxysms.
BRONCHIAL ASTHMA – General Characteristics, Pathology, Clinical Features, Diagnosis, Treatment and Prevention
BARBITURATES – General Features, Clinical Features and Treatment
GENERAL FEATURES
Till
recently, barbiturates were the most common drugs used for suicide. Accidental
poisoning is seen in epileptics, psychiatric patients and children who get regular
prescription for these drugs.
The most
widely used barbiturate is phenobarbitone and it is used as an anticonvulsant.
Absorption and metabolism of phenobarbitone are slow. About 10% of the drug is
excreted in urine unchanged. The lethal dose for adult is about 5 gm.
Simultaneous administration of alcohol aggravates its effects.
CLINICAL FEATURES
Central
nervous, respiratory and cardiovascular systems are affected the most.
Drowsiness, slowing of respiration and hypotension follow. Pupils are small and
react to light.
In severe
poisoning, when medullary centers are depressed, the pupils are dilated and
fixed, which indicates a poor prognosis. Tendon reflexes are sluggish or
absent. Necrosis of sweat glands and bullous lesions over the skin develop in a
few as a hypersensitive reaction. These lesions heal slowly.
Diagnosis
can be confirmed by detection of barbiturates in the gastric contents and
estimation of barbiturate in blood.
Treatment
In addition
to general measures, forced alkaline diuresis and dialysis are helpful.
Bemegride (megimide) is considered to be a specific antidote but subsequent
research has disproved this assumption.
Repeated doses of activated charcoal and hemoperfusion are the modalities described. Since pneumonia is a fatal complication, these patients should be observed for a week till recovery is complete.
BARBITURATES – General Features, Clinical Features and Treatment
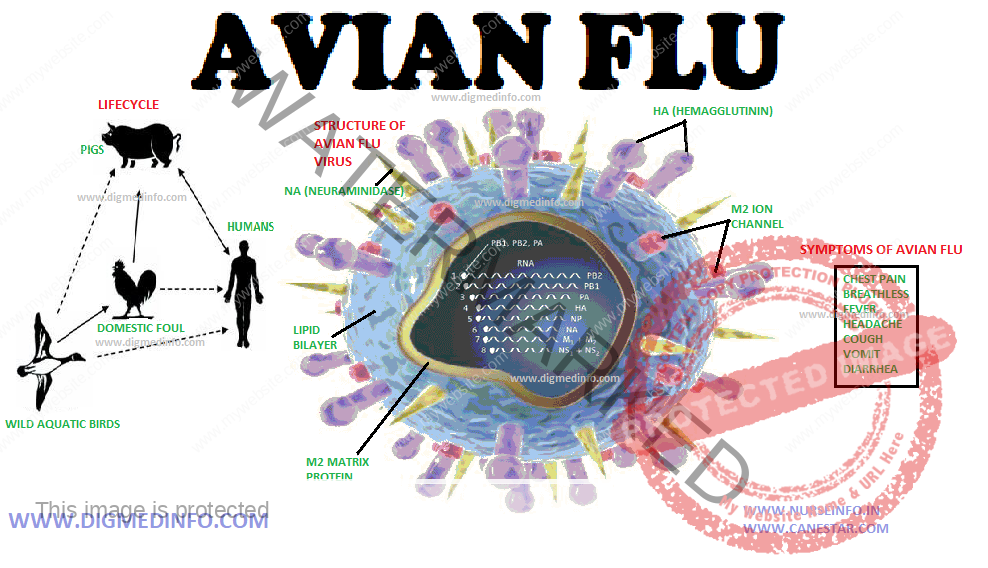
AVIAN FLU (INFLUENZA GROUP A H5N1 VIRUS) – General Characteristics, Clinical Features, Diagnosis and Management
General Characteristics
The subtype
H5 N1 influenza virus is a natural pathogen of chicken, ducks, turkeys and
others. Though it was thought to be pathogenic only to them, the subtype H5N1 has
crossed over to infect humans and caused small outbreaks. Hong Kong (1977)
Thailand, Cambodia, Indonesia and several other Asian countries have reported outbreaks
in poultry by H5N1 virus.
If human to
human transmission of the virus becomes efficient, devastating pandemic more
severe than the previous ones is likely to breakout. Pathologically the lesions
resemble those of classic influenza, but hemophagocytic histiocytosis may also
be seen.
Clinical Features
The
incubation period for human influenza viruses is short-2 to 3 days (range 1-7
days). However with influenza A H5N1 the median time between exposure and onset
of illness is 3 days (range 2 to 4 days). Most cases have occurred in
previously healthy children and young adults. Symptoms of bird flu in humans
include fever, cough, and sore throat, pneumonia, acute respiratory distress,
and lifethreatening complications. The symptoms of bird flu may vary depending
on the type of virus. Primary viral pneumonia and multi-organ failure are
common. In the present outbreak, more than half of those infected with the
virus have died. Death is due to respiratory failure and multi-organ failure
especially respiratory, renal and cardiac failure.
Criteria for suspecting avian flu
Persons with
illness characterized by fever, (temperature > 38oC), cough and/or sore
throat, severe respiratory symptoms and one or more of the following:
1. Contact
with a confirmed case of influenza A H5N1 during the infectious period,
2. Recent
(less than 1 week) visit to a poultry farm in an area known to have outbreaks
of HPAI (highly pathogenic avian influenza), or
3. Worked in
a laboratory that is processing samples from persons or animals suspected to be
having HPAI infection.
DIAGNOSIS
Procedure to Establish the Diagnosis
1. Suspect
the disease and start investigations. Virus can be isolated from pharyngeal
secretions 2-15 days after the onset of illness. Nasal secretions, blood, CSF
and feces also contain the virus. Children may continue to shed the virus in
nasal discharges for over 2 weeks after recovering from the acute attack.
2. Positive
immunofluorescence antibody (IFA) using H5N1 monoclonal antibodies can be
demonstrated in serum.
Diagnosis is
confirmed by the following tests:
1. Positive
viral culture for influenza A H5N1.
2. Positive
real time PCR for influenza A H5N1.
3. and/or
four-fold rise in H5N1-specific antibody titer.
MANAGEMENT
Avian
influenza virus is resistant to amantadine and rimantadine. Oseltamivir 75 mg
orally twice daily for 5 days and zanamivir would probably be useful if started
as early as possible. No vaccine is available now to protect against H5N1 virus
for general use.
A 2 dose
regimen of 90 μg of sub-virion influenza A (H5N1) given IM over the deltoid
muscle at 28 days interval generates neutralizing antibody. This vaccine is under
trial.
Infection Control Precautions for
Hospital Staff
Patients who
have visited endemic regions within 10 days and who present with severe febrile
illness and respiratory symptoms should be observed for avian influenza, with isolation,
barrier nursing and other precautions.
1. Proper
hand washing before and after contact with the patient.
2. Use
gloves and gowns for all patient contacts. Use separate equipment for
individual patients.
3.
Protection of the eyes with goggles or face shields.
4.
Precautions against droplet infection: Patients should be isolated in monitored
negative air pressure ventilation systems. Health care staff should use a fittested
respirator, or approved N-95 filtering mask when entering the room.
5. Suspected poultry meat and eggs should be properly cooked so that the whole item reaches a minimum temperature 70oC which is needed to destroy the virus.
AVIAN FLU (INFLUENZA GROUP A H5N1 VIRUS) – General Characteristics, Clinical Features, Diagnosis and Management
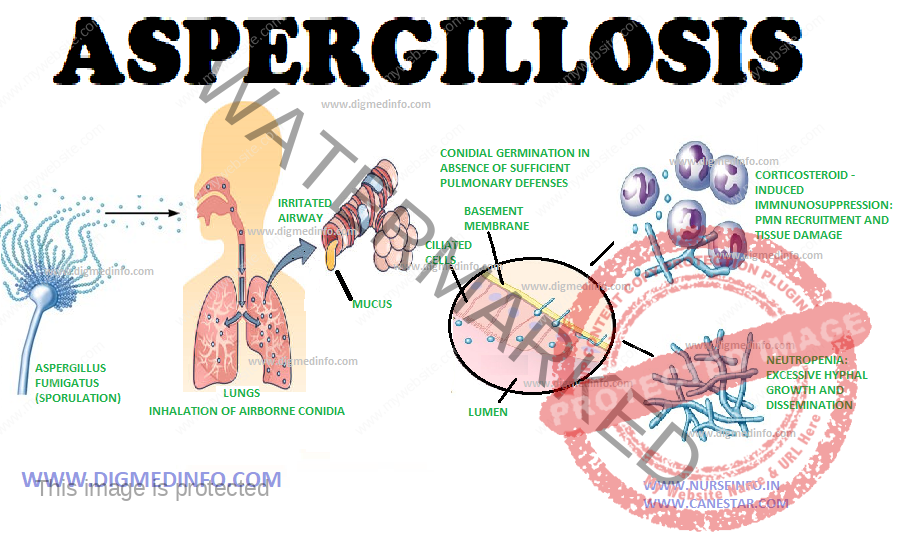
ASPERGILLOSIS – General Characteristics and Treatment
General Characteristics
The species
of aspergillus pathogenic to man are A. fumigatus, A. niger, A. flavus, A.
terrens and A. nidulans. Of these A. fumigatus is most common. Infection occurs
when general resistance is lowered or local disease favours superinfection.
Aspergillus is very widespread in nature and their spores are found in dust.
Both superficial and systemic lesions may develop. The commonest superficial lesion
is otomycosis. Systemic infection may be pulmonary or disseminated. Major
portal of entry is the respiratory tract.
Pulmonary
form: Allergic alveolitis may develop due to inhalation of fungal spores in
sensitized individuals. Aspergillus may grow in the bronchi to produce bronchopulmonary
disease. The hyphae may obstruct the lumen. Healed tuberculous cavities or
other types of cavities may be the seat of colonization by the fungus.
The mycelia
grow to form a tangled fungal ball which is recognizable in X-rays
(aspergilloma). It may remain asymptomatic or may cause massive hemoptysis. Invasive
aspergillosis occurring in immunosuppressed individuals leads to widespread
pulmonary necrosis with marked systemic symptoms.
Other sites
of lesion are the central nervous system and naso-orbital cavities. Diagnosis
can be made by histological demonstration of the fungus and isolation of the
organism from the exudates. Since Aspergillus is a common contaminant in
respiratory secretions, mere isolation does not prove its pathogenic role. Precipitating
antibodies can be demonstrated by gel diffusion test and this test is of great
value in diagnosis.
Treatment
Amphotericin B in a dose of 1 mg/kg/day is effective in systemic aspergilloma. Amphotericin B and 5-fluocytosine are effective in CNS disease. The underlying predisposing factor should be attended to. Cavities containing aspergilloma producing intractable hemoptysis have to be removed surgically. Other drugs like clotrimazole which are also effective in vitro are being evaluated. Other drugs effective against aspergillus include oral fluconazole itraconazole, voriconazole and posaconazole. Posaconazole can be given prophylactically against aspergillus and other fungal infections in neutrophilic patients. The dose is 200 mg tds oral. Capsofungin a new antifungal drug effective against aspergillus and other yeast species.
ASPERGILLOSIS – General Characteristics, Pathogenesis and Treatment
ASCORBIC ACID – SCURVY (ANTISCORBUTIC VITAMIN – VITAMIN C)
James Lind,
a Scottish naval physician, recognized the antiscorbutic properties of citrus
fruits in 1753 and this was considered an important discovery with far-reaching
effects.
Dietary
sources Ascorbic acid is present in a wide variety of foods. In the process of
cooking about 50% of vitamin C passes into water and 20% gets destroyed. Fresh
fruits, green leafy vegetables and germinating pulses are rich in ascorbic
acid. The Indian gooseberry and guavas are particularly rich sources. Animal
food like milk and meat contain only small amounts of this vitamin. The vitamin
is present in potato in the layer just below the skin. If the potatoes are
boiled whole with the skin, the vitamin diffuses into the deeper layers.
The minimum
daily requirement for an adult is 30-40 mg and for infants 5 mg per kg body
weight. Normal plasma levels vary between 0.7 and 1.5 mg per dL. Leukocytes,
platelets, and adrenal glands contain large amounts of vitamin C. Deficiency of
vitamin C causes scurvy.
Physiological actions
Vitamin C is
a strong reducing agent. It takes part in biological oxidation-reduction reactions.
Vitamin C is required for the formation of collagen by the hydroxylation of
proline. It takes part in the formation of hemoglobin, erythrocyte maturation
and the conversion of folic acid to tetrahydrofolate. Ascorbic acid reduces
ferric iron to ferrous iron which is more easily absorbed. Body stores of
ascorbic acid are small and, therefore, dietary deficiency leads to the
development of scurvy.
SCURVY
Deficiency
of vitamin C in the diet over a few weeks or months will lead to scurvy.
Clinical features of scurvy
Classic
scurvy is seen only infrequently in India since small amounts of vitamin C are
obtained in vegetables and pickled berries which form essential items of the
Indian diet. Cases do occur among inmates of mental homes, elderly persons and
among the very poor.
Manifestations
of scurvy vary in children and adults. Early symptoms include weakness, lassitude,
and normocytic normochromic anemia. In infancy and childhood subperiosteal
hemorrhages occur, which lead to painful swellings over long bones. Scurvy in
infancy produces pseudoparalysis owing to pain. This condition may mimic
arthritis, osteomyelitis, or poliomyelitis. X-ray abnormalities may develop
over the sternal ends of ribs and ends of long bones. Bleeding from the gums occurs
commonly at the sites of erupted teeth.
Retrobulbar,
subarachnoid, and cerebral bleeding may develop in a few cases. In adults early
manifestation is follicular hyperkeratosis over the skin of the lower limbs.
The lesions are papular with perifollicular hemorrhages which appear as
purpura. Hemorrhage into the deep tissues of the thighs and legs cause tense
induration (“woody leg”). Other sites of hemorrhage include joints, nail beds
and viscera. The gums are hypertrophied and the interdental papillae are red
and prominent (scurvy-buds). They bleed easily. Edentulous subjects do not get
gingival abnormalities. The gum changes are aggravated by infection. The teeth become
loose and may fall off. The hair assumes corkscrew shape since the follicles
are obstructed by keratin plugs. Wound healing is delayed and resistance to infection
is reduced. The condition is fatal if untreated.
Treatment
Scurvy is a
potentially fatal disease and sudden death may occur unexpectedly. Treatment
should be started without delay. In infants and children 25-50 mg of ascorbic
acid given daily three times a day is sufficient to replete the body stores. In
adults 500 mg is given daily in divided doses up to a total of 4 g. A diet rich
in vitamin C should be given to prevent relapse.
Prevention
Infant foods
should contain fruit juices or vitamin C supplements. Children, convalescent
subjects and elderly people who are liable to be neglected, should receive 25
mg of vitamin C daily. As an alternative, 500 mg may be given once a month.
Adverse effects of vitamin C
Side effects like digestive upsets and hypoglycemia occur if the drug is given in doses exceeding 3 g/day. Oxaluria and oxalate stone formation in the urinary tract may result from prolonged overdosage.
ASCORBIC ACID – SCURVY (ANTISCORBUTIC VITAMIN – VITAMIN C) PHYSIOLOGICAL ACTIONS, SCURVY, TREATMETN AND PREVENTION AND OVERDOSE
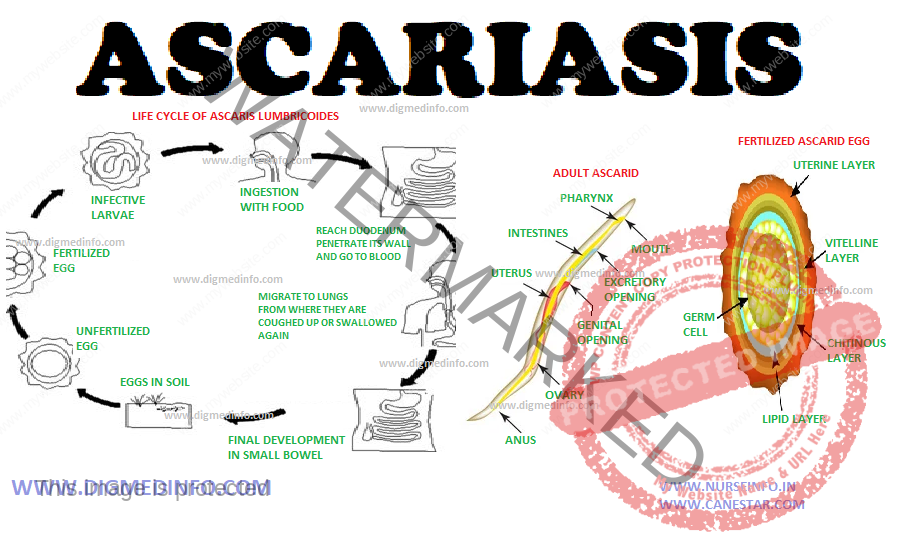
ASCARIASIS – General Characteristics, Life Cycle, Pathogenesis, Clinical Features, Diagnosis, Treatment and Prevention
General Characteristics
Ascariasis
is worldwide in distribution and is caused by the nematode Ascaris
lumbricoides. The worm measures 20-35 cm in length. The female is larger than
the male. The females lay several thousand eggs every day. The eggs are
elliptical, 30-40 μ x 50-60 μ in size with an outer dense mammilated shell and
a smooth translucent inner shell. They are passed in feces. They become
embryonated and infective in the soil in 2- 3 weeks and they can remain viable
under optimum conditions for years.
Life Cycle
Embryonated
eggs are ingested with food or water and the larvae hatch out in the small
intestine. They penetrate the intestinal mucosa to enter the venules or lymphatics
and travel to the lungs, where they develop for about 10 days. They then enter
the alveoli to be coughed up and swallowed. During the pulmonary phase the
larvae undergo four moultings and become resistant to gastric acid. The larvae
grow and mature in 2-3 months. Life span of this worm is 6-15 months.
Pathogenesis
During the
stage of larval migration, pulmonary symptoms like cough, wheezing and
hemoptysis may occur (Loeffler’s syndrome) and used to be a common cause of respiratory
symptoms in children. The adult worms ingest nutrients from the small intestine
and lead to nutritional deprivation. Large number of adults may form tangled
masses and obstruct the small intestines. The worm may migrate to ectopic sites
like the stomach, nasal cavity, biliary tree, pancreatic ducts, respiratory
passages, female genital tract or others. Absorption of the products of living
and dead worms leads to the development of allergy and toxic symptoms.
Clinical Features
Those due to
larvae: Respiratory symptoms such as cough, hemoptysis or wheezing may develop
1-5 days after swallowing the eggs. Eosinophilia may be present. Clinical
severity depends upon the worm load and reactivity of the host. The liver may
be enlarged and histology may show centrilobular necrosis. Rarely larvae may
reach the brain, giving rise to convulsions. Other organs may also be affected.
Those due to
adult worms: Light infestations are asymptomatic. Moderate worm loads produce
abdominal pain, pica, diarrhea,
abdominal distention and grinding of the teeth (bruxism). Infected children
have voracious appetite but they remain malnourished despite adequate intake of
food. Migration of worms to biliary ducts or pancreatic ducts leads to
obstruction. In heavy infection the masses of worms may lead to intestinal
obstruction and they may be palpable.
Diagnosis
It is made
from the history of passing round worms in the stool or the children may vomit
round worms. Diagnosis is confirmed by demonstrating the characteristic ova in
feces. In the rare event of infection by male worms alone, ova may not be
present in feces. During the stage of larval migration, the diagnosis has to be
presumptive
Treatment
The adult
worms respond to a variety of anthelmintics. Effective, safe and polyvalent
anthelmintics are preferred at present. In more than 30% of patients multiple helminths
occur, common combination being roundworm, whipworm and hookworm and broad
spectrum anthelmintics are more advantageous in them.
Benzimidazole
drugs which include albendazole and mebendazole bind to nematode β tubulin and
inhibit parasite microtubule polymerisation which causes death of adult worms
which may take a few days to complete.
Prevention
Improvement in nutritional status of children, health education, especially pertaining to personal hygiene and environmental sanitation reduce the infection rates. Mass deworming campaigns are helpful in endemic areas to reduce worm loads temporarily but reinfection withinmonths is the rule.
ASCARIASIS – General Characteristics, Life Cycle, Pathogenesis, Clinical Features, Diagnosis, Treatment and Prevention
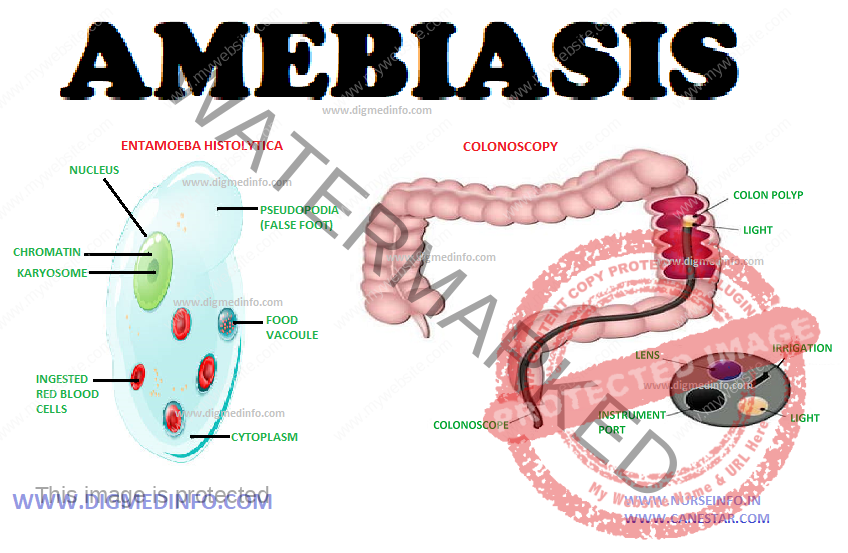
AMEBIASIS – General Characteristics, Pathology, Clinical Manifestations, Acute Amebic Dysentery, Hepatic Amebiasis and Treatment of Amebiasis
General Characteristics
The term
amebiasis includes all lesions caused by infection by the protozoan parasite Entameba
histolytica. These amebae cause ulcerative lesions in the large intestine
causing dysentery and from there they spread to several organs to produce
necrotic lesions.
There is a
great tendency for the intestinal infection to become chronic and persistent
for long periods. E.dispar is morphologically identical to E.histolytica, but
nonpathogenic. It is genetically different. It is a commensal. However, E.
histolytica can also remain in the bowel for many years without causing major symptoms.
Amebiasis is
worldwide in distribution, but it is very prevalent in tropical climates.
Chronic carrier state, poverty, insanitary disposal of excreta, unhygienic food
handling, and proliferation of flies are responsible for this high prevalence.
Though all age groups are susceptible, adults suffer more often.
Amebae are
widely distributed in nature. The common pathogen is E. histolytica. It exists
in two forms—the cyst and the trophozoite. The cysts are round or oval in shape
and measure 10 to 15 μ in diameter. In iodine-stained preparations the cysts
show one, two or four nuclei depending on their maturity. Cysts resist adverse environment.
In addition to the nucleus, one or more rodlike structures called chromidial
bars, and a glycogen mass are also seen. Cysts are formed in the bowel when the
environment becomes unfavorable for the trophozoite and are then passed out in
feces. Cysts are responsible for transmission of the disease from person to
person. The vegetative form (trophozoite) is actively motile by the aid of
pseudopodia. It measures 20 to 50 μ in diameter.
Invasive
trophozoites are identified by the presence of ingested erythrocytes within
them. Amebae multiply by binary fission. The trophozoite is the invasive form
and is responsible for all lesions. A large number of trophozoites is seen in
the feces of dysenteric patients. Trophozoites and cysts occur in the feces of
carriers. Outside the body, the trophozoites survive only for an hour or so.
Normal gastric juice destroys them in the stomach. Cysts survive external
environment for long periods.
Transmission
Humans are
the only reservoir for E.histolytica. Cysts are passed in the feces of cases
and carriers. These are ingested along with food or water. Cysts resist acid
digestion in the stomach. Excystation occurs in the intestines, Trophozoites
develop from cysts and they establish themselves in the colon, feeding on the
bacteria and desquamated epithelial cells. They multiply by binary fission.
These non-invasive forms may persist for long periods without producing any
symptoms. Under favourable conditions these become invasive.
PATHOLOGY
Intestinal
amebiasis: The invasive trophozoites adhere to colonic mucosa with the help of
specific lectins and ulcerate the mucous membrane and penetrate deep into the
submucosal layers of the colon. The basic pathological process is a lytic
necrosis of tissue. This is due to an extra cellular cysteine kinase enzyme
causing proteolytic destruction of the tissue, producing flask shaped ulcers.
E.
hystolytica which produce lytic enzymes kills host cells which come into
contact with them. The host cells become immobile on contact with E.
histolytica, and the cells die. E. histolytica can also induce apoptosis in
host cells. The cellular response consists of mononuclears and a few polymorphs.
Amebae are seen in the invading margins of the lesions. Cecum, ascending and
descending colon, and rectum are the sites of predilection.
The appendix
may be involved. The terminal ileum may be affected rarely. The ulcers have
undermined edges and are covered by dense yellow or brown slough. The mucous
membrane between ulcers is healthy. Ulceration may extend to blood vessels
causing severe hemorrhage at times. Perforation of the bowel may occur, but it
is rare. Sometimes ameboma or amebic granuloma develop due to repeated infection
by ameba and bacterial pathogens. The acute inflammatory process has a tendency
to subside spontaneously.
In many
patients chronic infection persists with microscopic lesions which harbour E.
histolytica for many years. The lesions may heal in a few cases. Persistence of
the chronic lesions accounts for the carrier state. E. histolytica infection is
associated with transient immunosuppression. Activated macrophages form the major
defence against invasive amebae. The resistance against invasive amebiasis is
mainly cell mediated immunity.
Extra-intestinal Lesions
Amebic liver abscess: Invasive amebae reach the liver through
the portal blood stream from the colon which is the primary seat of infection.
In the liver they multiply and cause colliquative necrosis of liver cells to
produce abscess.
Possibly
malnutrition, alcoholism and consequent immunosuppression favour the
development of liver abscess. Unlike pyogenic abscess, the wall of the amebic abscess
is made up of necrotic and compressed liver tissue and it is devoid of
granulation tissue. Active amebae are found near the expanding margins. The pus
is made up of necrotic tissue which shows amorphous material and erythrocytes.
It is sterile on culture.
In most
cases the colour of the pus is reddish brown or chocolate. Amebae are seen only
rarely in the pus aspirated from the center of the abscess, they are more often
demonstrable in the pus aspirated from near the walls on subsequent occasions.
The site of the abscess is more commonly the right lobe. It is usually single
and may attain very large size.
The abscess
may enlarge progressively and spread by contiguity to the chest wall, colon,
diaphragm, pleura, and pericardial cavities. Amebic abscess does not impair hepatic-function
significantly. Jaundice is generally mild or absent, but pressure over a major
hepatic duct can give rise to obstructive jaundice. On aspirating the pus the
liver tissue comes into apposition and complete healing occurs without structural
damage or fibrosis.
During acute
amebic dysentery, the liver may enlarge as a result of diffuse inflammation
caused by the products of inflammation of the colonic tissue and bacteria
reaching the liver in the blood stream. The hepatic lesion clears up with cure
of the dysentery. This lesion should not be mistaken for liver abscess.
Other foci
for embolic lesions include the lungs, brain, spleen and other tissues. Direct
invasion of the skin by active vegetative amebae leads to extensive spreading necrotic
ulceration-cutaneous amebiasis.
CLINICAL MANIFESTATIONS
The
incubation period varies from a few weeks to months.
Spectrum of
illnesses caused by E. histolytica
Intestinal amebiasis
1.
Asymptomatic infection
2.
Symptomatic non-invasive infection
3. Acute
proctocolitis (Dysentery)
4. Toxic
megacolon
5. Chronic
non dysenteric colitis
6. Ameboma
7. Peri anal
ulcers
Extra intestinal amebiasis
1. Liver
Absces
2. Pleuro
-Pulmonary involvement
3.
Pericarditis
4.
Peritonitis
5. Brain
abscess
6. Genito
urinary disease
ACUTE AMEBIC DYSENTERY
This
presents with sudden or subacute onset of lower abdominal pain and diarrhea
with blood and mucus in stools. The frequency ranges from 3 to 10 in a day. At times
watery diarrhea with large amounts of blood and mucus may occur. Constitutional
symptoms are mild and these include low grade fever and vague discomfort.
Palpation of
the abdomen reveals colonic tenderness and mild hepatomegaly. The feces are
semisolid or liquid, showing fecal matter mixed with blood and mucus. Microscopic
examination shows erythrocytes, a smaller number of leukocytes and trophozoites
of E. histolytica. In the majority of cases, the condition subsides after several
weeks even without treatment, to exacerbate again with dietary irregularity, psychological
stress or other factors.
Complications
are rare but in a few cases extensive destruction of mucosa and submucosa may
lead to severe hemorrhage and occasionally perforation. Rectalprolapse,
intussusception and colonic stricture may develop in some. Amebomas may develop
in the cecumor other parts of the colon and these may be mistaken for tumours.
These resolve completely with specific treatment.
Non-dysenteric Amebiasis
This is a
common mode of presentation in endemic areas. The condition starts insidiously
with abdominal discomfort, flatulence, intermittent diarrhea with constipation,
and the presence of mucus in stools. Asymptomatic intervals and periods of
dyspepsia alternate for many months or years. Vague general symptoms like feverishness,
mild depression, fear and anxiety may be prominent. Physical examination may
reveal palpable tender cecum and sigmoid and sometimes tender hepatomegaly. An
amebic granuloma (ameboma) may be felt as a sausage-shaped mass in the right
iliac fossa and this may be mistaken for malignancy or tuberculosis.
Mucosal
ulcers may be seen on sigmoidoscopy. Examination of the mucus collected by
sigmoidoscopy may show the active trophozoites. Repeated examination of fresh
stool or sigmoidoscopic specimen may be necessary to establish the diagnosis.
Sigmoidoscopic biopsy reveals the ulceration and the parasite in the mucosa.
HEPATIC AMEBIASIS
Hepatic
involvement used to be very common, almost all patients give a history of
alcoholism. Around 50% of patients suffering from hepatic amebiasis give
history of dysentery. Liver involvement manifests as insidious onset of pain in
the right hypochondrium or right lower chest with fever, chills and sweating.
Loss of weight and anemia may be pronounced.
In the early
stage the liver is enlarged as a whole. The pathological process is not
inflammatory, but it consists of multiple necrotic lesions caused by amebae
diffusely distributed in the liver. In this stage the organ is enlarged as a
whole and it is acutely tender. This stage may persist for varying periods and
may resolve either spontaneously or with treatment, without proceeding to
abscess formation.
At present
the occurrence of liver complications has come down. In those in whom abscess
develops, the liver is considerably enlarged and tender. When the abscess
spreads to the abdominal wall, there is superficial edema and severe local
tenderness. The majority of liver abscesses are in the right lobe. Left lobe
lesions are palpable over the epigastrium. Diaphragmatic involvement causes pleuritic
pain in the right lower chest.
Physical examination
reveals diminished air entry, impaired percussion note and crepitations over
the lower part of the right chest. Jaundice is rare. Blood shows mild
tomoderate leukocytosis (about 12-14.000/cmm) with polymorphonuclear cells
dominating the field. The ESR is usually high. Fluoroscopy reveals elevation of
the right dome of the diaphragm and diminished movement. Ultrasound, CT scan
and isotopic scanning help to locate the site of the abscess.
Complications
of liver abscess include rupture into neighbouring organs or cavities leading
to peritonitis, right sided empyema, bronchohepatic fistula, and pericarditis. Untreated,
the mortality may go up to 10%.
Cutaneous
amebiasis occurs over the genitalia, perianal region, opening of sinuses and
around colostomy wounds. Rarely metastatic lesions from the liver develop in
the lungs and brain. Rupture of a liver abscess into the peritoneum causes the
clinical picture of an acute abdominal emergency with shock.
Differential Diagnosis
Amebic
dysentery has to be differentiated from bacillary dysentery, ulcerative colitis
and tuberculous enterocolitis. Ameboma may closely resemble carcinoma. Chronic intestinal
amebiasis may be mistaken for irritable bowel syndrome, diverticulitis,
neurasthenia or malabsorption state. Hepatic amebiasis is a common cause of
prolonged fever in the tropics and when liver enlargement and tenderness are
not marked, it resembles enteric fevers, brucellosis or tuberculosis.
In an
endemic area, enlargement and tenderness of the liver should suggest the
diagnosis of amebic liver abscess. Other conditions such as alcoholic liver
disease, primary and secondary tumours of the liver, subdiaphragmatic abscess
and pyogenic liver abscess have to be differentiated. In case of doubt the
diagnosis is confirmed by ultrasonography and later, aspiration. Prompt
response to antiamebic drugs is a point suggesting a diagnosis of hepatic
amebiasis.
Laboratory Diagnosis
Examination
of the feces – Fresh stool examination by light microscopy invariably reveals
E.histolytica in dysentery. Active E. histolytica shows characteristic ameboid
movement and ingested erythrocytes. In chronic amebic colitis cysts are present
in feces in varying numbers. These can be identified in saline preparations but
cellular details are better demonstrable in iodine stained specimen. Unlike
bacterial dysentery, the feces does not contain innumerable leukocytes. Plenty
of erythrocytes are present. Stool occult blood may be present in invasive
intestinal disease. Stool enzyme immunoassay also will be useful.
Apart from
feces, vegetative E. histolytica can be demonstrated in the following specimen.
1. Liver
abscess pus.
2. Sputum in
pulmonary amebiasis.
3. Discharge
from cutaneous amebiasis.
Serological
tests – These tests are mainly used in extraintestinal disease. Indirect
hemagglutination antibody test is positive in 95% of extraintestinal and 70% of
intestinal amebiasis. Other tests also have been developed.
Indirect
immunofluorescence is positive in more than 60% of cases. Countercurrent
electrophoresis and agar gel diffusion are other methods employed.
Imaging
studies:
ultrasonography
– A single lesion in the posterosuperior aspect of the right lobe of the liver
is commonly seen. But, multiple abscesses may also occur in some patients. Deep
seated abscess may be missed on clinical evaluation. Multiple abscesses should
suggest the possibility of pyemic etiology.
CT scan – In
cerebral amebiasis, CT may show irregular lesions without surrounding capsule
or enhancement.
Other
investigations – Blood counts may show mild anemia, leucocytosis, elevated ESR
and elevated alkaline phosphatase.
Endoscopy –
Rectosigmoidoscopy and colonoscopy may reveal small mucosal ulcers covered with
yellowish exudates, and the intervening mucosa appears normal. For demonstrating
vegetative amebae the fresh mucus exudates should be examined as a saline
preparation, microscopically.
In chronic
intestinal amebiasis the feces show amoebic cysts, when the disease is
quiescent. With acute exacerbation, trophozoites appear from time to time. Charcot-Leyden
crystals may be seen as a result of chronic bleeding foci. These crystals are
needle shaped, refractile, and are made up of lysophopholipase.
TREATMENT OF AMEBIASIS
Drug
treatment consists of amebicidal drugs. These may act on the parasites found in
the lumen of the gut or on the invasive forms seen in the tissues. They are
grouped as luminal amebicides and tissue amebicides. Some drugs, however, have
action on both sites.
Prevention:
The most important steps are to observe food hygiene, provide safe drinking water and arrange for sanitary disposal of human excreta. Ordinary chlorination of drinking water does not kill the cysts. Cooks and food handlers should be periodically examined and the infection eradicated. Fruits and vegetables can be rendered safe by washing with soap and peeling off the skin wherever possible.
AMEBIASIS – General Characteristics, Pathology, Clinical Manifestations, Acute Amebic Dysentery, Hepatic Amebiasis and Treatment of Amebiasis