AVIAN FLU (INFLUENZA GROUP A H5N1 VIRUS) – General Characteristics, Clinical Features, Diagnosis and Management
General Characteristics
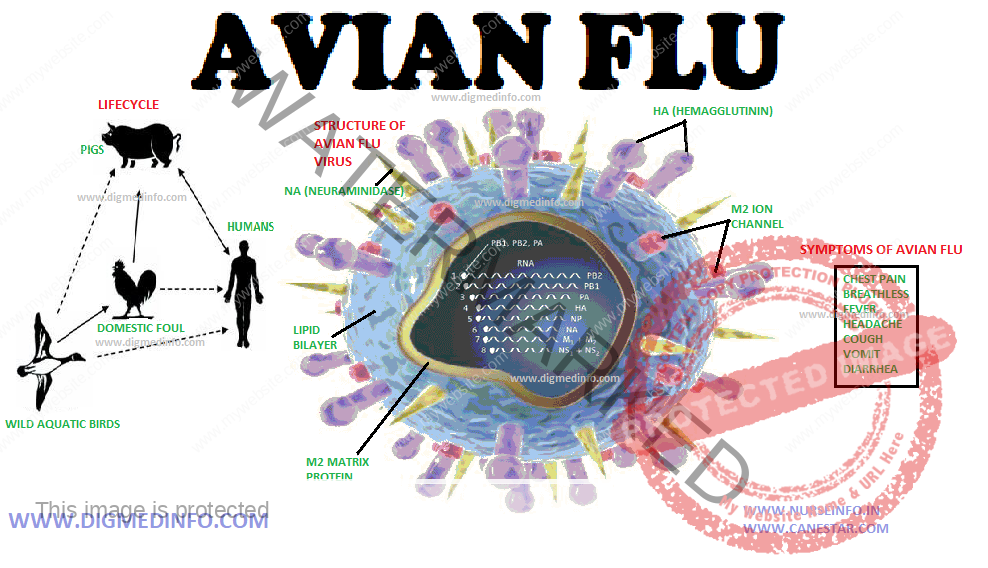
The subtype H5 N1 influenza virus is a natural pathogen of chicken, ducks, turkeys and others. Though it was thought to be pathogenic only to them, the subtype H5N1 has crossed over to infect humans and caused small outbreaks. Hong Kong (1977) Thailand, Cambodia, Indonesia and several other Asian countries have reported outbreaks in poultry by H5N1 virus.
If human to human transmission of the virus becomes efficient, devastating pandemic more severe than the previous ones is likely to breakout. Pathologically the lesions resemble those of classic influenza, but hemophagocytic histiocytosis may also be seen.
Clinical Features
The incubation period for human influenza viruses is short-2 to 3 days (range 1-7 days). However with influenza A H5N1 the median time between exposure and onset of illness is 3 days (range 2 to 4 days). Most cases have occurred in previously healthy children and young adults. Symptoms of bird flu in humans include fever, cough, and sore throat, pneumonia, acute respiratory distress, and lifethreatening complications. The symptoms of bird flu may vary depending on the type of virus. Primary viral pneumonia and multi-organ failure are common. In the present outbreak, more than half of those infected with the virus have died. Death is due to respiratory failure and multi-organ failure especially respiratory, renal and cardiac failure.
Criteria for suspecting avian flu
Persons with illness characterized by fever, (temperature > 38oC), cough and/or sore throat, severe respiratory symptoms and one or more of the following:
1. Contact with a confirmed case of influenza A H5N1 during the infectious period,
2. Recent (less than 1 week) visit to a poultry farm in an area known to have outbreaks of HPAI (highly pathogenic avian influenza), or
3. Worked in a laboratory that is processing samples from persons or animals suspected to be having HPAI infection.
DIAGNOSIS
Procedure to Establish the Diagnosis
1. Suspect the disease and start investigations. Virus can be isolated from pharyngeal secretions 2-15 days after the onset of illness. Nasal secretions, blood, CSF and feces also contain the virus. Children may continue to shed the virus in nasal discharges for over 2 weeks after recovering from the acute attack.
2. Positive immunofluorescence antibody (IFA) using H5N1 monoclonal antibodies can be demonstrated in serum.
Diagnosis is confirmed by the following tests:
1. Positive viral culture for influenza A H5N1.
2. Positive real time PCR for influenza A H5N1.
3. and/or four-fold rise in H5N1-specific antibody titer.
MANAGEMENT
Avian influenza virus is resistant to amantadine and rimantadine. Oseltamivir 75 mg orally twice daily for 5 days and zanamivir would probably be useful if started as early as possible. No vaccine is available now to protect against H5N1 virus for general use.
A 2 dose regimen of 90 μg of sub-virion influenza A (H5N1) given IM over the deltoid muscle at 28 days interval generates neutralizing antibody. This vaccine is under trial.
Infection Control Precautions for Hospital Staff
Patients who have visited endemic regions within 10 days and who present with severe febrile illness and respiratory symptoms should be observed for avian influenza, with isolation, barrier nursing and other precautions.
1. Proper hand washing before and after contact with the patient.
2. Use gloves and gowns for all patient contacts. Use separate equipment for individual patients.
3. Protection of the eyes with goggles or face shields.
4. Precautions against droplet infection: Patients should be isolated in monitored negative air pressure ventilation systems. Health care staff should use a fittested respirator, or approved N-95 filtering mask when entering the room.
5. Suspected poultry meat and eggs should be properly cooked so that the whole item reaches a minimum temperature 70oC which is needed to destroy the virus.