ZINC AND SELENIUM – SOURCES, SYNDROME AND SUPPLEMENTS
ZINC
Zinc is
present in many enzymes. Highest concentration occurs in the liver, voluntary
muscle, bone, prostate, and ocular structures. Foods such as meat, fish, peas
and cereals contain zinc. Daily requirement is not clearly known, but is around
15 mg. Dietary deficiency is very rare. Zinc deficiency leads to impairment of
maturation and immunodeficiency. In malnourished subjects zinc deficiency may
result in thymic atrophy.
A syndrome
of dwarfism and hypogonadism seen in Egypt and Iran has been attributed to zinc
deficiency. Oral zinc sulphate corrected this clinical picture. Acrodermatitis
enteropathica is an inherited disorder resulting from the malabsorption of
zinc, probably due to an enzymic defect.
Administration
of zinc sulphate 30-150 mg/day results in complete remission. Oral zinc
sulphate 100 mg/day has been found to stimulate the growth of granulation
tissue in chronic ulcers. Oral supplementation of zinc 10 mg (5mg) in children
less than 1 year of age for 16 months reduced overall all-cause mortality by
7%.
SELENIUM
Selenium is a constituent of selanoproteins. It has structural and enzyme roles and it acts as an important antioxidant. It is a catalyst for the production of thyroid hormone. Other functions include: (1) proper functioning of the immune system, (2) sperm motility, (3) maintenance of proper mood and mental state, (4) resistance against cancer. Selenium retards the progress of AIDS. Daily requirement is 400-450 μg/day. Dietary sources include Brazil nuts, kidney, crab, liver, shellfish, fish, meat, poultry, wheat and some vegetables. In animal foods selenium is present as sclenocystine. In vegetable sources it occurs as sclenomethionine.
ZINC AND SELENIUM – SOURCES, SYNDROME AND SUPPLEMENTS
YELLOW FEVER – Etiology, Distribution and Incidence, Distribution and Incidence, Transmission and Epidemiology, Pathogenesis and Pathology, Clinical Features, Diagnosis, Treatment and Prevention
Yellow fever
is an acute mosquito-borne infection of varying severity characterized by the
triad of hepatitis, hemorrhagic diathesis and proteinuria.
Etiology
The
causative virus is an arbo virus belonging to the genus Flavivirus, in the
family Flaviviridae.
Distribution and Incidence
Yellow fever
is prevalent in many parts of Africa, tropical parts of South America and
Panama. The presence of the efficient vector Aedes aegypti mosquitoes and the
non-immune population pose a threat of the disease spreading, if the virus is
introduced.
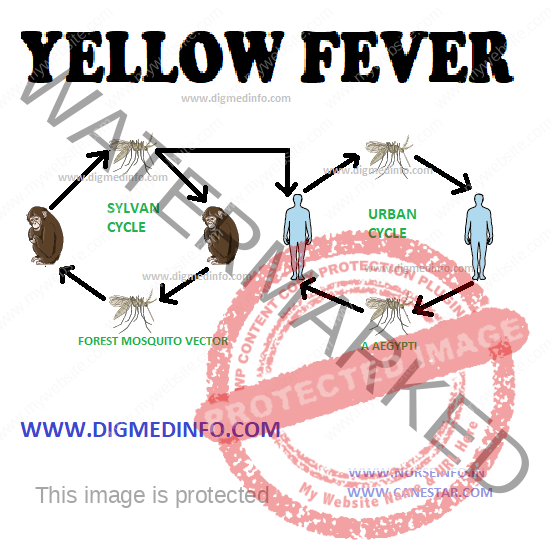
Transmission and Epidemiology
Epidemic
(urban) yellow fever is transmitted from human to human by Aedes aegypti
mosquitoes. Infected monkeys and the vector mosquitoes maintain the reservoir
of infection in the jungle. These act as a source of infection when the humans
intrude into endemic areas.
Pathology and Pathogenesis
The
incubation period after an infectious mosquito bite is 3 to 6 days. Liver and
kidneys show maximal lesions but hemorrhage may occur in all organs. Hepatic
changes include widespread necrosis, and degeneration of liver cells. Renal
changes include acute tubular necrosis and subcapsular hemorrhages. Bleeding
diathesis is due to depletion of hepatic clotting factors, intravascular
coagulation, and platelet abnormalities. Direct damage to the myocardium,
kidneys and other organs and the effects of vasoactive cytokines, lead to fatal
complications such as multi-organ failure and shock.
CLINICAL FEATURES
In the
majority of cases, the disease is a self limited with fever and myalgia. 25 to
50% of cases may develop the full syndrome with complications such as
hemorrhages, jaundice, renal involvement and shock.
The first
stage (i.e. period of infection) is due to the direct effect of the virus. It
starts abruptly with fever, headache and myalgia. In severe illness there is
nausea vomiting, abdominal pain and distressing pain in the back, and limbs.
There is relative bradycardia. This stage lasts about 3 days and by 4th day the
temperature comes down and the second stage (period of remission) starts.
Many cases
recover without going to the third stage. Some progress to the third stage
(period of intoxication). It starts after a day or a few days, with resumption
of high fever, body pains, nausea, vomiting, abdominal pain and changes in the
level of consciousness. Bradycardia, jaundice, wide spread hemorrhages and
renal failure may supervene. Death is due to hepatic or renal failure and
shock.
Diagnosis
In endemic
areas, fever, leukopenia and proteinuria with or without jaundice should
suggest the possibility of yellow fever. Specific diagnosis is established by
the isolation of the virus from the blood in the first few days of fever or
demonstration of rising titer of antibodies in serum.
Treatment
There is no
specific antiviral treatment. Symptomatic and supportive measures should be
instituted. Hepatic and renal failure has to be anticipated and managed accordingly.
Prevention
Vaccination using live attenuated vaccine (17D strain) is very effective. Vaccination gives immunity starting from ten days and full protection for 10 years. Though side effects are generally negligible, children below 9 months may develop encephalitis. Pregnancy is not a contraindication for vaccination. Many countries insist on yellow fever vaccination for persons entering the country or remaining during transit, if they come from endemic areas. Persons travelling to endemic areas have to take vaccination.
YELLOW FEVER – Etiology, Distribution and Incidence, Distribution and Incidence, Transmission and Epidemiology, Pathogenesis and Pathology, Clinical Features, Diagnosis, Treatment and Prevention
X-linked Inheritance – Sex Chromosome Related Disorders, X-linked Recessive Inheritance and X-linked Dominant Inheritance
Sex Chromosome Related Disorders
In all
females one of the ‘X’ chromosome derived from either parent undergoes
inactivation at the early period of gestation, in a random manner governed by
the laws of probability Lyon’s hypothesis (1961). Females, therefore contain a
mosaic of tissue cells containing either the maternal or the paternal
X-chromosome. Inactivation of the X-chromosome is effected by the action of a
gene called the X-inactivation specific transcript which is located in the long
arm of the X-chromosomes. Since 50% of the X-chromosomes in carrier females are
normal, they do not manifest signs of the disease, but male offsprings suffer
from the disease.
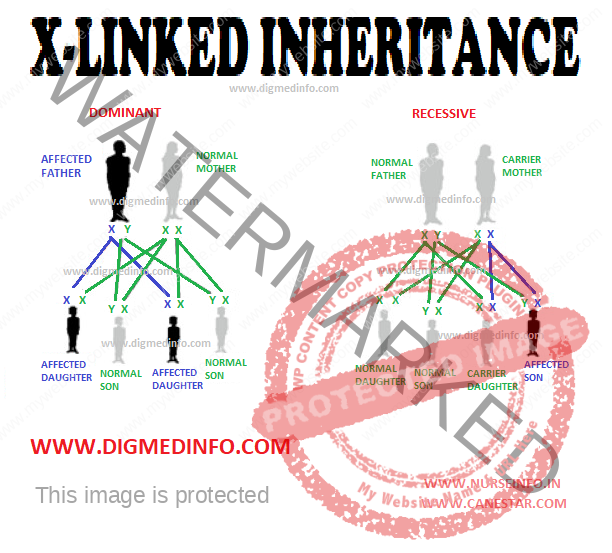
X-linked Recessive Inheritance
1. There is
‘oblique’ transmission, i.e., in the pedigree a line drawn through the affected
persons is oblique.
2. Only
males are affected, females are only carriers.
3. For the
offsprings of a carrier female there is a 50% chance of sons being affected and
a 50% chance of daughters being carriers.
4. Among
offsprings of an affected male, none of the sons will carry the trait, while
all the daughters will be carriers.
A female may
manifest an X-linked trait if the normal X-chromosome is inactivated during
early fetal life or if she is the offspring of a carrier female and affected
male, or if the unaffected X-chromosome is structurally abnormal, as in
Turner’s syndrome, e.g., hemophilia, Christmas disease, pseudohypertrophic
muscular dystrophy.
X-linked Dominant Inheritance
1. The
number of females affected is double the number of affected males.
2. The
affected male passes Y-chromosome to his sons (and not the X-chromosome).
Therefore, all sons of an affected male are normal, whereas all daughters of an
affected male are abnormal.
3. The
affected female passes the mutant X-chromosome to half her daughters and to
half her sons and, therefore, half the daughters and half the sons are affected.
The disease is usually milder in the female, because of the normal gene on the other X-chromosome, e.g. hypophosphatemic type of vitamin D resistant rickets.
X-linked Inheritance – Sex Chromosome Related Disorders, X-linked Recessive Inheritance and X-linked Dominant Inheritance
The term
pertussis, which means intensive cough, is an acute respiratory infection, seen
more commonly in young children. The disease is also more serious in them. The term
“whooping cough” is derived from the occurrence of progressive repetitive
paroxysms of cough followed by inspiratory whoop. Natural pertussis infection
and vaccination do not produce life-long immunity. The immunity wanes over a
few decades. Since there is almost complete coverage of DPT vaccination in
children, adolescents and adults may become susceptible to infection
increasingly. It is therefore possible that adults develop pertussis infection.
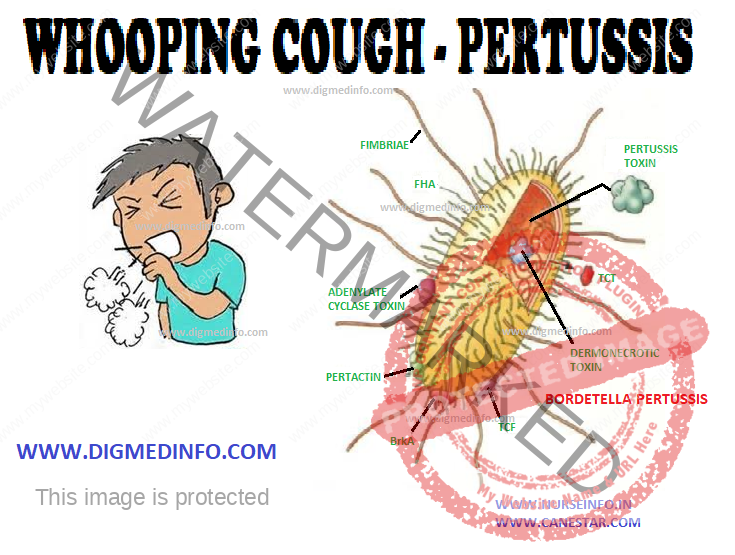
Pertussis is
caused by Bordetella pertussis which is highly infective. Bordetella
parapertussis and B. bronchiseptica are members of the same genus, rarely
causing disease in man. Maximum incidence is seen in children below five years
and the mortality is highest for children below 1 year of age. The organisms
are spread by droplet infection and the route of entry is the respiratory
tract.
The
infectious period is the catarrhal prodrome and for three weeks after the onset
of illness. Bordetella are small gram-negative coccobacilli, exclusively
pathogenic to humans. The genome of B.pertussis has been sequenced.
Pathology
The mucosal
lining of the respiratory tract shows inflammation. Peribronchial lymphoid
hyperplasia occurs initially and this is followed by necrosis of the midzonal and
basilar layers of the bronchial epithelium. This leads to the accumulation of
tenacious mucus, atelectasis and eventually bronchiectasis.
Clinical
Manifestations
The
incubation period is usually 7-14 days but may be prolonged to 20 days. Three
stages can be distinguished—catarrhal, paroxysmal and convalescent—each lasting
up to 2 weeks so that the course of the disease extends to 6-8 weeks.
The catarrhal stage manifests with
rhinorrhea, mild fever, and cough. During this stage, clinical recognition of
the disease is difficult. This is the most infective stage.
In the paroxysmal stage cough starts,
increases in severity, and becomes repetitive and explosive. Each paroxysm is
followed by a whoop produced by a sudden massive inspiratory effort through a
narrowed glottis. During the paroxysms of cough the infant develops facial
congestion, distension of neck and scalp veins, lacrimation, cyanosis, and
clouding of consciousness. The paroxysm ends with the onset of vomiting. The
whoop may not be distinctly made out in younger infants, but they may become asphyxiated
and develop anoxic convulsions. Physical examination may reveal periorbital
edema. In the uncomplicated cases lung signs are usually absent. Pertussis occurring
in adults causes prolonged cough. With increasing age the manifestations also
become more severe.
Convalescence is marked by the decrease in
frequency and severity of the paroxysms. Vomiting subsides and the patient’s
appetite improves. At this stage the child is very susceptible to develop
superinfections by other respiratory pathogens and this may lead to recurrence
of the
paroxysms of
cough. When this occurs it may last for several months.
Complications
Complications
are common to develop
A. Respiratory:
Otitis
media, especially in infants
Bronchitis
Bronchopneumonia
Atelectasis
(segmental or lobar)
Interstitial
or subcutaneous emphysema or pneumothorax due to rupture of alveoli
Bronchiectasis
Flare-up of
tuberculosis
Sudden death
of the infant may occur
B. Central nervous system:
Convulsions
may occur due to anoxia, encephalopathy or rarely intracranial hemorrhage.
C. Gastrointestinal:
Severe
vomiting with dehydration, tetany, ulceration of the frenum of the tongue (due
to biting during a paroxysm), prolapse rectum, hernia.
D. Hemorrhages:
Epistaxis
Subconjunctival
hemorrhage
Hemoptysis,
hematemesis
E. Malnutrition:
Severe
emaciation occurs in most of the affected children. In poor communities it is
the starting point for marasmus and kwashiorkor.
Diagnosis
The disease
has to be suspected clinically, particularly in an unimmunized child with known
contact with the disease. Total leucocyte count is elevated to 20,000 to 50,000/cmm
with absolute lymphocytosis. A leukemoid reaction may sometimes occur. Chest
X-ray may show perihilar infiltrates or segmental collapse. Bacteriological diagnosis
is established by culturing the organism obtained from nasopharyngeal swabs.
Fluorescent antibody staining of pharyngeal specimens provides a rapid and
specific diagnosis. PCR using nasopharyngeal aspirate reveals the organisms. In
cases with duration above two weeks IgG antitoxic antibody can be demonstrated
in serum.
Treatment
Supportive
care is important to maintain nutrition, prevent aspiration into the
respiratory tract and maintain the airway. The airway is cleared by suction of
the exudates. Anoxic convulsions are managed by administration of oxygen and
anti-convulsants. Small, frequent feeds are tolerated if given soon after a
paroxysm of cough.
Intravenous
fluids may be required if the child is dehydrated. In general, administration
of antibiotics does not shorten the paroxysmal stage, once it is established. Erythromycin
50 mg/kg/day given for 5-7 days will reduce the period of communicability. It
may even abort or prevent the progress of the disease if given in the catarrhal
stage. Ampicillin, chloramphenicol and cotrimoxazole may also be used as
alternative drugs. Azithromycin 250-500 mg po, od for 7-10 days is effective in
controlling the infection if started early. Clarithromycin is a suitable alternative.
Antibodies
are not transferred transplacentally in the case of whooping cough. In most
patients, a single attack confers life-long immunity.
Prevention
Active immunization is achieved by the administration of the pertussis vaccine, usually given in combination with diphtheria and tetanus toxoids (DPT). The vaccine contains killed B. pertussis. The initial dose is given at 2 months, with 2 more doses at 4 week intervals. The first booster is given 1 year later and the next one at school entry.
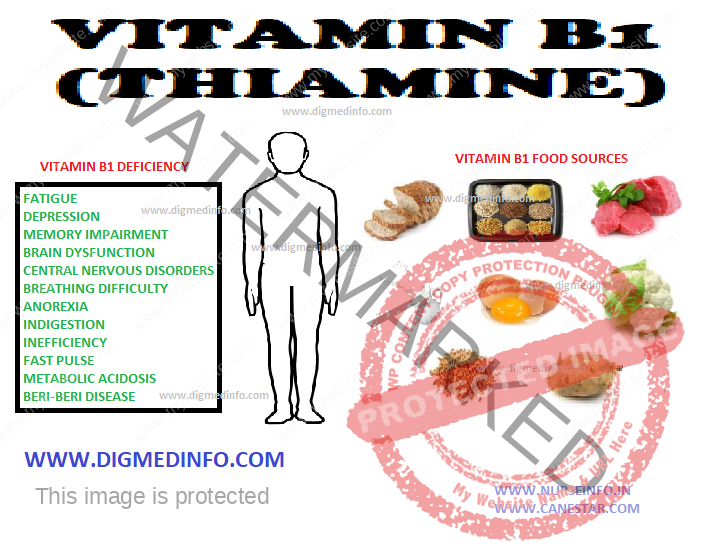
Thiamine
plays an essential part in the metabolism of carbohydrates by acting as a
coenzyme required for the decarboxylation of pyruvate to acetyl coenzyme A. It
also takes part in other steps of the Kreb’s tricarboxylic acid cycle. Cereals
contain the vitamin, which is maximal subjacent to the bran. Thiamine content
of rice is lost during milling and polishing. Parboiling allows the vitamin to
penetrate the grain and conserves it to some extent. Other good sources of the
vitamin are sprouting pulses, green leafy vegetables, liver, pork, and legumes.
Part of the vitamin is lost by washing or discarding the water used for
cooking. The daily requirement is 0.4 mg/1000 kcal, i.e. 1.2 mg/day.
Requirement is partially influenced by the intake of carbohydrates.
Deficiency States
Pathology of deficiency
In thiamine
deficiency the cells cannot utilize glucose aerobically. Nervous system is affected
first. Pyruvic and lactic acids accumulate and this leads to vasodilation. The
myocardium shows loss of striation, vacuolation of fibers, fragmentation and
edema. Cardiomyopathy, encephalopathy and peripheral neuropathy may develop.
Sensory, motor and autonomic nerves show demyelination and degeneration.
Clinical features
Cardiovascular
involvement results in ‘wet beriberi’ and nervous system involvement results in
‘dry beriberi’. Cardiovascular system Peripheral vasodilation leads to high
output circulatory state, myocardial failure and retention of sodium and water
leading to edema. The pulse is of high volume. The extremities are warm owing
to vasodilation and tender owing to neuropathy. Acute fulminant cardiac failure
may be rapidly fatal. Wet beriberi may occur in breastfed infants aged 2-8
months. The child presents with edema, oliguria and an aphonic cry. If not clinically
suspected, this condition may be missed. Sudden death may occur.
Neurological involvement
This
manifests as symmetrical sensori-motor polyneuropathy with muscle wasting. Foot-drop
and wrist-drop are common. Deep hyperaesthesia occurs and it manifests as calf
tenderness.
Wernicke’s encephalopathy
This is an
acute neurological manifestation which is more common in alcoholics. Pathological
changes occur in the upper part of the midbrain, hypothalamus and the walls of
the third ventricle which show congestion and petechial hemorrhages, most marked
in the mammillary bodies. The onset is sudden with vomiting, confusion,
bilateral ophthalmoplegia, loss of consciousness, nystagmus, ataxia and
psychological disturbances. Confusion proceeds to coma and death. Korsakoff’s
syndrome is characterized by retrograde amnesia, impaired ability to learn and
confabulation. Wernicke’s encephalopathy is associated with high mortality.
Prompt administration of thiamine rapidly restores normalcy.
Diagnosis of thiamine deficiency
The
condition has to be suspected clinically. It can be confirmed by demonstrating raised
levels of blood pyruvate. Normal blood pyruvate is 62.5 to 125 mmol/liter and
it may rise to 375 mmol/liter (3.3 mg/L). Measurement of erythrocyte transketolase
activity, before and after the addition of thiamine pyrophosphate gives the
most reliable diagnostic test.
Treatment:
When
beriberi is suspected or diagnosed, 50 mg thiamine should be given
intramuscularly daily for several days. After controlling the acute symptoms 2.5-5
mg should be given orally as maintenance. Wet beriberi and Wernicke’s
encephalopathy have to be treated as medical emergencies. A dose of 25-100 mg
of thiamine should be given intravenously to save life. Dramatic recovery with
diuresis occurring within hours of injection confirms the diagnosis.
Infants with beriberi should be given 10 mg thiamine intramuscularly followed by oral doses. The mother also should be treated with oral doses of 10 mg twice daily for several days. Since polyneuropathy and Korsakoff’s psychosis are more resistant to treatment, the vitamin has to be given for prolonged periods. Once neuropathy is established, residual paralysis persists even after therapy. Adverse side effects to thiamine include sensitization and anaphylactic shock.
VITAMIN E AND K (Fat Soluble Vitamin)
– Dietary Sources, Clinical Features, Treatment and Prevention
VITAMIN E
(ANTI-STERILITY VITAMIN)
Vitamin E is
a tocopherol. Among the tocopherols alpha tocopherol is the most easily
absorbed and biologically most active compound. All vegetable oils, wheat-germ,
cotton seeds, egg yolk, butter and peas contain this vitamin and the average
Indian diet contains the daily requirement which is 15 IU or 5 mg. Vitamin E
which is a strong antioxidant prevents the peroxidation of cellular and subcellular
membrane phospholipids. It is probably involved in preserving the integrity of
cell membranes.
In cattle
and poultry, vitamin E deficiency may lead to infertility. Nutritional
deficiency of vitamin E is rare. Excess of free fatty acids in the diet
increases the requirement for vitamin E. In premature infants fed on artificial
diets containing iron and high concentrations of fatty acids, conditioned
deficiency may develop, leading to the production of hemolytic anemia.
In doses of
400-800 mg, vitamin E acts as an effective antioxidant, thereby retarding the
development of atheromatous changes in arteries.
VITAMIN K (COAGULATION VITAMIN)
This vitamin
which is chemically a substituted naphthoquinone is present in adequate amounts
in vegetable oils and green leafy vegetables as vitamin K1 (phytomenadione).
Vitamin K comprises of several molecular forms that have a common 2-methyl-l,
4-naphthoquinone ring, but different side chains at the 3-position. In green
leafy vegetables and legumes and vegetable oils such as rapeseed oil and
soyabean oil vitamin K occurs as phylloquinone (old name K1).
Bacteria
synthesize vitamin K which is named menaquinone (MK-n) which occurs in several
molecular forms. Milk is a poor source. The colonic bacteria synthesize this
vitamin (Vitamin K2) and this supplements the dietary source.
Naturally occurring vitamin K is fat soluble. The synthetic form of this
vitamin is vitamin K3 which is water-soluble. This can be given
intramuscularly or intravenously, unlike the oily preparations which can be
given only intramuscularly. Daily requirement is not clearly known, but is
probably 1 μg/kg body weight. Body sources are limited and, therefore, signs of
deficiency develop within 3 to 4 weeks of dietary deprivation. Oxidative
phosphorylation processes which take place in cellular mitochondria require the
presence of vitamin K. Vitamin K occurs in large amounts in liver and bone. In the
liver it takes part in the synthesis of precursors for coagulation factors,
protein C and protein S. Vitamin Kdependent coagulation factors (factors II,
VII, IX and X) are produced in the inactive form by the liver, and vitamin K is
required for their biological activation. The inhibitors of coagulation—Protein
C and Protein S are also produced in the liver and these are also vitamin K
dependent. Coumarins inhibit the enzyme vitamin K epoxide reductase and thereby
inhibit further actions of Vitamin K.
Prothrombin
(factor II) is synthesized in the liver as an inert precursor, termed protein
induced by vitamin K absence (PIVKA). This is carboxylated to form prothrombin
by the vitamin K dependent enzyme—gamma carboxylase. In the absence of vitamin
K or after
administration
of vitamin K antagonists such as coumarin PIVKA appears in the plasma.
Vitamin K is
needed for the formation of several proteins concerned with calcium
homeostasis. Vitamin K promotes the conversion of protein-bound glutamate residues
to gamma-carboxy glutamate (Gla). Proteins containing Gla are present in
several tissues such as bone, kidneys, placenta, pancreas, spleen and lungs.
Vitamin K
also takes part in bone metabolism—both bone formation and resorption. Two of
the important Vitamin K dependent proteins are osteocalcin and matrix Gla protein.
Vitamin K Deficiency
Vitamin K
deficiency occurs in conditions associated with malabsorption of fat such as
obstructive jaundice and malabsorption states. Prolonged treatment with broad spectrum
antibiotics destroys the colonic bacteria which synthesize this vitamin.
Deficiency manifests as mild or severe bleeding tendency occurring from
injection sites, mucous membranes, and skin. Injections of vitamin K in doses
of 5-10 mg corrects the defect, if hepatic parenchymal function is normal. In
the presence of hepatic failure, vitamin K may not be effective.
HEMORRHAGIC
DISEASE OF THE NEWBORN
Hemorrhage
may develop in newborn infants occasionally. Prematurity predisposes to this
condition. Vitamin K deficiency in the mother and anticoagulant medication aggravate
this disorder. Hemorrhagic tendency
develops on the second or third day of delivery. This is due to exaggeration of
the physiological hypoprothrombinemia which develops before the colon is
colonized by bacteria.
A dose of 1
mg of vitamin K1 given intramuscularly to the baby brings about relief.
Synthetic vitamin K is also effective. Larger doses have to be avoided since
these lead to hemolysis. Administration of 5-10 mg vitamin K to the mother in
late pregnancy abolishes this risk in the newborn.
Anticoagulant
therapy Use of coumarin drugs or warfarin leads to alteration in the synthesis
of coagulation factors. As a result proteins antigenically similar to factors
II, VII, IX and X are produced but they lack the procoagulant properties.
Excess of anticoagulants leads to hemorrhagic tendency.
Bleeding occurs from injection sites, urinary tract, gastrointestinal tract and uterus. Intramuscular injection of 10 mg vitamin K is usually effective. When the bleeding tendency is severe, large intravenous doses (50-75 mg) may be required. For severe cases transfusion of fresh blood or vitamin K-dependent coagulation factors may also be necessary.
VITAMIN E AND K (Fat Soluble Vitamin) – Dietary Sources, Clinical Features, Treatment and Prevention
VITAMIN – D – Biological Actions, Daily Requirements, Rickets, Clinical Features, Diagnosis, Treatment and Prevention
Vitamin D is
required for normal metabolism of calcium and phosphorus and for bone
formation. It enhances the absorption of these minerals from the gut, their mobilization
from bone and the reabsorption of phosphorus by the kidney. Vitamin D1 is the
essential precursor for 1-25 alpha dihydroxy vitamin D1 which is the steroid
hormone required for the development of bone, growth in children, maintenance
of bone mass in adults and also for the retardation of osteoporosis and
prevention of fractures in the elderly.
The two
different forms of vitamin D active in man are vitamin D (calciferol) obtained
by ultraviolet irradiation of ergosterol (also called ergocalciferol or
provitamin D2) which is of plant origin, and vitamin D3 (cholecalciferol) which
is formed by activation of 7-dehydrocholesterol present in the epidermal cells
of human skin as a provitamin D2. This activation is effected by the
ultraviolet rays ranging in wavelength from 296 to 310 A obtained from sunlight
naturally. Exposure to sunlight for 20-30 minutes daily ensures adequate supply
of Vitamin D. Excessive exposure does not lead to overdose of the vitamin. Skin
damaged by burns will not be capable of producing Vitamin D on exposure to sunlight.
Vitamin D2
is obtained from the diet and vitamin D3 is formed endogenously. On an average
the endogenous source supplies about 80% and diet about 20% of the total requirement.
Vitamin D2 and D3 which are identical in potency, differ only in the
configuration of the side chain. Vitamin D3, though formed in the skin is also
absorbed through the small intestine. Further metabolism of vitamin D2 and D3
is identical and these together are referred to as vitamin D.
Biological actions of vitamin D
metabolites:
1. Increase
the absorption of calcium and phosphate from the small intestine by promoting
active transport.
2. Increase
mobilization of calcium from bone by promoting osteoclastic activity.
3.
Stimulation of reabsorption of calcium and phosphate at the renal tubules.
The overall
result of all these processes is to increase serum calcium and phosphate.
Deficiency of vitamin D results in impairment of mineralization of bone leading
to nutritional rickets in children and osteomalacia in adults.
Dietary
sources of vitamin D are milk, butter, cheese, egg yolk and fish liver oils.
This vitamin is heat stable. One international unit (IU) is equivalent to 0.025
μg. The daily requirement varies depending on the age.
DAILY REQUIREMENTS
Infant and
children – 400 IU
Age 19-50
years – 200 IU
51-70 years
– 400 IU
71 and above
years – 600 IU
RICKETS
Prevalence
Rickets is prevalent in India, more so in the north than in the south.
Premature babies are more vulnerable. The disease is more florid during winter months
when exposure to sunlight is minimal. Prevalence is more among the poor and
illiterate classes. Indians who have emigrated to affluent countries still show
a higher prevalence of rickets. Osteomalacia is more common in multiparous
women who have nursed their babies repeatedly. Rickets has been ranked among
the most frequent childhood diseases affecting children in the developing
world. There is evidence that dietary deficiency of calcium may also lead to
rickets.
In rickets,
the arrangement and normal regenerative processes of cartilage are abnormal.
Subsequent calcification of the cartilaginous matrix and osteoid do not proceed
normally. The osteoid and cartilage which remain uncalcified are deposited
irregularly. These give rise to a wide irregular frayed zone of non-calcified cartilage
and osteoid termed rachitic metaphysis. These in turn account for many of the
skeletal deformities. In the subperiosteal region also, while resorption of
cortical bone continues normally, new bone is not laid down, resulting in
softening and rarefaction of the bone shaft. In vitamin D deficiency, since
absorption of calcium and, phosphorus from the gut is defective, serum calcium and
phosphorus levels fall. Lowered level of serum calcium stimulates the secretion
of parathyroid hormone which in turn, leads to mobilization of calcium from the
bone. Thus, the serum calcium is usually maintained normal for considerable
periods, tetany developing only rarely. Since parathyroid hormone (PTH)
decreases reabsorption of phosphorus by the renal tubule, the serum phosphorus
falls. The serum alkaline-phosphatase is elevated due to increased osteoblastic
activity.
CLINICAL FEATURES
Florid
rickets manifests by the age of 1-2 years. Early manifestations These include
irritability, flabbiness of muscles, prominence of abdomen and delay in the
appearance of milestones, except speech. Skeletal manifestations These are the
most characteristic features. They develop several months after the deficiency is
established. The bones which have the maximum rate of growth at the time of
onset of the deficiency show gross abnormalities.
In children
below the age of 1 year the lesion is craniotabes, characterized by abnormal
softening of the skull in the occipital region. In children aged 2 years or
more epiphyses of the wrists and ankles are widened and costochondral junctions
are enlarged and beaded. In advanced rickets, deformities of bones are aggravated
because of muscular action, gravity and weight bearing.
Head
Craniotabes
disappears by 1 year of age, but the excess of osteoid and non-calcified
cartilage gives rise to frontal and parietal bossing giving the skull a ‘hot
cross bun’ appearance. Due to softening of the skull bones the calvarium is
asymmetric. The head may be larger in size and closure of the anterior
fontanelle may be delayed. The teeth erupt late; show defective enamel, and are
more susceptible to develop caries. Permanent teeth also show grooving, pitting
and hypoplastic enamel.
Rib-cage
Costochondral
junctions are thickened (rachitic rosary) and the sternum projects forwards
(pigeon chest deformity). A horizontal groove (Harrison’s sulcus) develops
along the diaphragmatic attachment due to
muscular
pull of the diaphragm on the softened bone.
Spine
This shows
kyphosis and scoliosis when the baby starts sitting and later lordosis in the
erect posture.
Pelvis
In lordotic
subjects the pelvis shows a corresponding deformity. The pelvis is small and deformed
(triradiate pelvis), and in female subjects the obstruction caused to the
pelvic outlet gives rise to dystocia during parturition.
Extremities
The femur,
tibia and fibula bend producing deformities like knock knees, coxa vara, etc.
The thickened epiphyseal ends may be more prominent. Deformities of upper limbs
develop if rickets sets in when the infant is crawling. Long bones may develop
green stick fractures and pseudofractures. The sum total of bony deformities of
the spine, pelvis, and legs leads to rachitic dwarfism.
Other
general manifestations include hepatosplenomegaly, tetany, laryngysmus
stridulus, convulsions and frequent respiratory infections.
Diagnosis
Rickets
should be suspected in any child showing deformities of skull, long bones and
ribs and in those with apathy, flabbiness, delayed milestones of development,
laryngysmus stridulus or convulsions.
The clinical
diagnosis is supported by the history of inadequate vitamin D in the diet or
chronic diarrhea interfering with absorption of vitamin D, and it is confirmed by
radiological investigations and biochemical tests. X-ray findings in active
rickets Routine skiagrams of the wrists give clues in diagnosis and are helpful
for following the progress. The distal ends of radius and ulna appear concave
(cupping), widened (flaring) and irregular (fraying). The distance between the
distal ends of the ulna and the radius and the metacarpal bones is apparently increased
since the uncalcified rachitic metaphyses is translucent to X-ray. Shafts of long
bones show decreased density and prominent trabeculations. Subperiosteal osteoid
may give a double contour to the shaft.
With
treatment, the lesions tend to heal. A line of preparatory calcification (LPC)
appears. This is separated from the distal end of the shaft by a zone of
translucency caused by the uncalcified osteoid. As healing progresses, the
osteoid becomes calcified and shaft apparently grows towards the LPC and unites
with it.
Measurement
of serum 25 hydroxy vitamin D gives a reliable indication of the adequacy of
the nutritional status. Normal values are above 15 ng/mL. Values below 8 mg/mL
indicate severe deficiency.
Biochemical
changes
In florid
cases the serum phosphorus is low (1.5-3.5 mg/dL) Serum calcium may usually be
normal, but in advanced cases it is reduced especially in cases with tetany.
Serum alkaline phosphatase is raised to 20-60 KA units/dL (Normal 5-15). With
correction of the lesion alkaline phosphatase level falls and serum phosphorus
level goes up. Normal serum vitamin D levels range from 35 ± 3.5 ng/mL (80
nmol/L) and 1,25 (OH)2 D is 35 ± 3 pg/mL.
In active
rickets these levels are lowered.
Prognosis
for growth and cosmetic recovery is excellent if the condition is recognized
early and treated before deformities develop. Intercurrent infections make the prognosis
worse. If treatment is started after the bony deformities are established and
the epiphyses are ossified, the deformities tend to persist.
Treatment
Oral
administration of vitamin D in doses of 1500-5000 IU daily brings about rapid
improvement in the vast majority of cases. Radiological improvement will be
demonstrable in 2-4 weeks. A single dose of 600,000 units is preferable for
advanced cases. The dose may be given orally or as in intramuscular injection.
An oily preparation is available for intramuscular injection which is effective
for 3 months. Three to four injections are given at intervals of two weeks.
Parenteral administration is mandatory in cases showing malabsorption. If there
is no improvement even after two parenteral doses of vitamin D, the case is
considered to be resistant to vitamin D.
After
complete healing of the lesion vitamin D should be given in doses of 400 units
daily for preventing recurrence. Children should be encouraged to get exposure
to sun for 20-30 minutes daily. Early bone lesions will be corrected with
simple medical treatment. If treatment is started late and deformities are
permanent, orthopedic correction is indicated.
Vitamin
D-resistant rickets
This may be
acquired, as in chronic renal failure or inherited as in congenital enzyme defects.
In chronic
renal failure conversion of 25-OH D3 into the active metabolite
1,25(OH)2D3 becomes defective due to the progressive
deficiency of the enzyme in the renal tubules. Such patients develop features
of rickets (renal rickets) forming part of renal bone diseases.
Inherited
forms of rickets
Pseudo-vitamin
D deficiency: Two types are known. Rickets develop early in life. Hypotonia, weakness,
seizures and growth failure develop.
Vitamin D
dependent rickets type I
This is an
autosomal recessive trait in which the gene for expressing the renal enzyme 25
hydroxy vit D3 1-alpha hydroxylase is defective, and so this enzyme level is
low or absent. Plasma levels of 25(OH)D3 are normal, but 1,25 (OH)2D3
are low. The gene is located on chromosomes X 12 q 13.3.
Vitamin D
dependent rickets type II
Two forms
exist. In one form, the gene for vitamin D receptor is mutated. Hypocalcemic
rickets develops. In the second form, also known as X-linked hypophosphatemic
vitamin D resistant rickets the phosphate regulating gene (PEX gene) with
homology to endopeptidoses on the X chromosome is defective. All these forms
respond to 1,25(OH)2 vitamin D.
HYPERVITAMINOSIS D
Prolonged
administration of massive doses of vitamin D results in vitamin D intoxication.
This causes hypercalcemia. Symptoms include nausea, vomiting, constipation,
drowsiness, and signs of renal impairment. Metastatic calcification occurs in
several tissues including
the kidneys, lungs, gastric mucosa and blood vessels. Renal function may deteriorate before other signs of toxicity are manifest. Subjects receiving high doses of vitamin D should have regular monitoring of serum calcium and if it is above 2.6 mmol/liter (10.5 mg/dL), the intake of the vitamin should be stopped.
VITAMIN – D – Biological Actions, Daily Requirements, Rickets, Clinical Features, Diagnosis, Treatment and Prevention
UNARMED TAPEWORM (Taeniasis saginata) (Beef Tapeworm) – General Characteristics, Life Cycle, Clinical Features, Diagnosis, Treatment and Prevention
GENERAL CHARACTERISTICS
Taeniasis
saginata is infection caused by Taenia saginata. This is the commonest among
the large tapeworms found in man and is distributed worldwide. Prevalence is
highest in areas where beef is a major source of meat. The adult worm grows to
a length of 10 meters and may consist of over 2000 segments. It lies free in
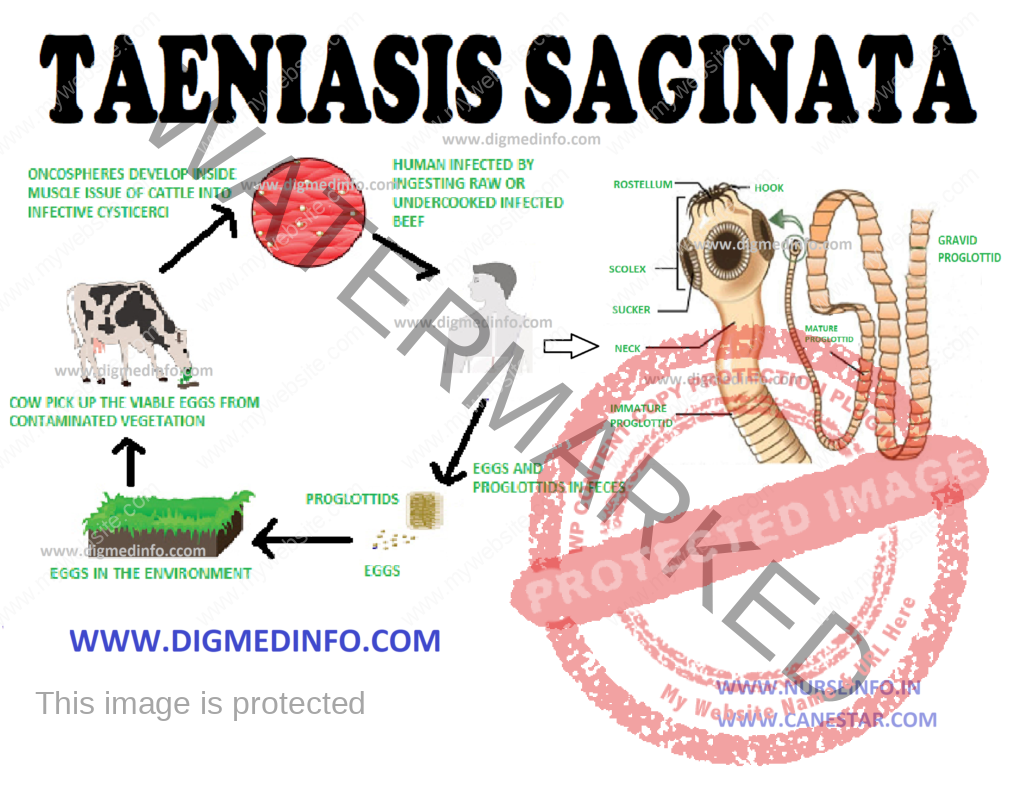
the jejunum and ileum, the head being attached to the mucosa. The scolex is 2 mm
in diameter and bears no hooklets, but has four suckers. The gravid segments
are actively motile and they come out in chains along with feces or wriggle out
singly due to their intrinsic muscular action. The uterus has about 20 lateral
branches.
The eggs are
spherical measuring 30-45 μ in diameter and the egg shell is thick, striated
and bile-stained. The embryo or onchosphere bears six hooklets and it remains viable
for 4-8 weeks. The adult worm may live for 10-25 years.
Life Cycle
Man is the
definitive host and cattle and llamas form the intermediate hosts. Eggs passed
in feces contaminate soil. These are ingested by grazing cattle. The
onchospheres are liberated in the intestine and they penetrate the mucosa,
enter the blood stream, and reach various muscles, mainly those of the heart,
tongue, shoulder, neck and loins. On reaching these sites the onchospheres lose
their hooks and grow into the cystic stage known as cysticercus bovis in 60-70
days. The cysticercus is ovoid, measures 8 × 5 mm and contains a single
sprouting scolex. Cysticercus remains viable for 1-3 years within the muscles.
Heavily infected meat is easy to distinguish by the presence of numerous cysts.
On ingesting
undercooked meat, the cyst wall is digested and the head attaches itself to the
intestinal mucosa and rapidly grows to reach the adult size in 6-8 weeks. A
host usually harbors only one or two worms.
Clinical Features
Majority is
asymptomatic, though vague symptoms such as abdominal pain, diarrhea and
increased appetite may occur in a few. The motile segments emerging out of the anus
may cause pruritus and anxiety to the host. Appendicitis and biliary
obstruction have been reported rarely.
Diagnosis
History of
passing segments and seeing the segments in feces confirm the diagnosis. The
species can be identified by observing the number of lateral branches of the
uterus. An easy method is to press the segment between two glass slides and to
hold it against light. Taenia saginata segment has more than 15 lateral
branches, whereas Taenia solium has only less than 13. Eggs can be demonstrated
by microscopic examination of the feces or by examining perianal scotch tape
swab. The eggs of T. saginata, T. solium and T. echinococcus cannot be
differentiated from each other
Treatment
Both
niclosamide (Yomesan) and praziquantel are effective against T. saginata.
Niclosamide kills the scolex and segments on contact. Four tablets, each of 0.5
g, are given as a single dose to be thoroughly chewed in the morning with a
gulp of water. The worm is passed partially digested 24-36 h later. If the
whole worm including the scolex is not passed, the worm re-grows and segments reappear
in stools within 3 months. In this case the drug is repeated in the same dose. Praziquantel
in a dose of 10-15 mg/kg body weight given as a single dose orally is adequate
to dislodge the intestinal adult worm in almost all cases. The drug is generally
safe. Side effects include dizziness, headache, vomiting and allergy. It is
available as tablets of 500 mg and 600 mg.
Prevention
Taenia saginata infection can be prevented by avoiding infected beef, inspection of slaughterhouses and proper disposal of excreta.
UNARMED TAPEWORM (Taeniasis saginata) (Beef Tapeworm) – General Characteristics, Life Cycle, Clinical Features, Diagnosis, Treatment and Prevention
TOBACCO SMOKE AND CHEWING – GENERAL CHARACTERISTICS AND TREATMENT
Man has started
using tobacco from very ancient times. At present tobacco is consumed for
smoking (beedi, cigarette, pipe, cigar, hookah, etc.) or for chewing with or
without other constituents such as betel, arecanut, and lime or as snuff
applied to the nasal or oral mucosa. All
these habits are
very much prevalent in all societies in India.
GENERAL CHARACTERISTICS
Tobacco
smoke contains several constituents, which irritate the respiratory tract and
inhibit ciliary action. The tar that is produced is carcinogenic to the
respiratory tract. Depending upon the brand of cigarette and the manner of
smoking the level of carbon monoxide in the smoke may vary from 1-5%. Nicotine
present in tobacco is responsible for the addiction. Sympathomimetic effects of
nicotine give rise to higher heart rate, elevation of systolic and diastolic
blood pressure, increase in cardiac output and peripheral vasoconstriction. The
threshold for ventricular tachycardia and ventricular fibrillation is lowered.
By increasing platelet aggregation, platelet adhesion, plasma fibrinogen and
viscosity of blood, nicotine favors intravascular thrombosis. There is reduction
in platelet survival and clotting time. Atherogenesis is favored by the rise in
total cholesterol, low density lipoproteins and free fatty acids, and also fall
in high density lipoproteins (HDL) brought about by nicotine. Blood levels of
carboxyhemoglobin are elevated. Oxygen carrying capacity of blood is reduced.
Rise in blood carbon monoxide leads to intimal hypoxia, increase in the
permeability of arterial intima and lipid deposition.
Cigarette
smoking is associated with mild airway obstruction and impairment of lung
function in adolescents. Females are affected more. Heavy smokers suffer from
tachycardia, palpitation, cardiac arrhythmias, hypertension, tremors, anorexia,
agitation and insomnia. In those who practice the chewing habit, in addition to
absorption of nicotine from the buccal mucosa the local irritation caused by
the cud leads to precancerous and cancerous changes.
SMOKING
Tobacco is a
highly habit forming agent. Several studies have been shown that the first
cigarette exposes the individual and the addiction will occur even with the
second or third ‘smoke’. Children of smoking parents acquire this habit more
freely. The harmful ingredients taken up by the smoker and exhaled by him
depend upon several factors such as the number of cigarettes smoked and their
frequency, depth of inhalation, smoking the cigarette only partially or fully
and the environment in which the smoker smokes – whether open or confined
space. Inhalation of the exhaled smoke by others nearby is termed passive
smoking, which is also associated with adverse effects in various degrees.
There is
irrefutable evidence that smoking is a major risk factor for chronic
bronchitis, emphysema and cancers of lung, larynx, esophagus, bladder, kidney,
pancreas and cervix uteri. Coronary heart disease, hypertension, strokes, peripheral
vascular occlusions, thromboangitis obliterans, peptic ulcers and several other
conditions are directly or indirectly attributable to tobacco. Tobacco is the
most important cause of cancer and cancer death, affecting several organ systems.
Both main stream and second hand smoke are group-1 carcinogens, i.e. included
among the highest cancer causing agents in humans. Lung cancer is several times
more common in smokers compared to nonsmokers. 90% of bronchogenic carcinoma is
related to smoking, either direct or passive. Smoking contributes to 50% of the
death of cigarette smokers, with half of these deaths occurring in middle life.
Smokers lose 10 years of their life expectancy, compared to non-smokers.
Smoking by
parents has an adverse effect on their children. Smoking mothers have an
increased risk of spontaneous abortion and their children have lower birth weights,
higher perinatal mortality and a greater risk of sudden infant death syndrome.
Medical associations of several countries have urged their governments to undertake
measures to restrict the spread of tobacco habit. These include restriction of
sales of tobacco to those below the age of 18 years, ban on advertisement,
education in schools and through public media, prohibition of smoking in public
places and public transport, heavy taxation on cigarettes and withdrawal of
aids to tobacco industry.
Tobacco Chewing
There are
recent reports from India that chewing tobacco is also associated with
increased risk of cardiovascular morbidity. Further studies are needed. Betel
chewing as a cause of oral cancer is well known. Several brands of such proprietary
preparations (Pan Masalas) are available in the Indian market. These are being
used by a large number of persons, especially the youth. Their role in the
genesis of oral cancer and other systemic diseases is not yet fully assessed.
OCCUPATIONAL HEALTH PROBLEMS AMONG
TOBACCO WORKERS
The
varieties of tobacco include Virginia tobacco (cigarette tobacco) and
non-virginia tobacco. Persons may be exposed to tobacco during agricultural operations
or curing processes. Ill effects of tobacco are considered to be due to
absorption of nicotine through the skin or respiratory tract. The levels of
nicotine and its metabolic product cotinine are increased in urine.
The symptom
complex occurring in the exposed workers is collectively known as green
symptoms. These consist of neurological symptoms like headache, giddiness,
nausea, vomiting, prostration and respiratory symptoms such as cough and
dyspnea. Usually, these symptoms are transient. The occurrence of green
symptoms is associated with raised urinary levels of nicotine and cotinine.
Virginia tobacco is less toxic than the non-virginia variety. The respiratory
symptoms may be aggravated by aero-allergens such as pollen and fungi belonging
to the species Gladosporium and Altemaria. The nature of contact with tobacco
also partly determines the clinical manifestations. Persons who pluck the
leaves generally get headache and giddiness, while those carrying the leaves
for curing get nausea and vomiting. In agricultural workers engaged in curing,
entry of tobacco is through the respiratory tract.
Treatment
Since the symptoms are usually mild, and last only for a few hours, removal from the surroundings is itself curative. The local practice among the workers is to take tea and jaggery followed by rest.
STARVATION – General Characteristics, Clinical Features and Treatment
GENERAL CHARACTERISTICS
Severe
starvation on a mass scale occurs during special situations like prolonged war,
drought, and other natural or political calamities. Chronic starvation of
different grades affects large number of people in the developing countries,
even during normal times. Several famines have occurred during the 19th and
early part of the 20th centuries. Famines were a regular occurrence
in Bengal during the colonial rule. Though acute and chronic food shortage
occur from time to time in various parts of India as a result of floods,
drought or earthquakes, widespread famine has not occurred in the latter part
of this century.
In addition
to food shortage, inability to ingest or digest and absorb food also results in
starvation. Individuals may resort to starvation voluntarily or this may result
from psychiatric abnormalities.
Loss of
weight amounting even up to 50% of body weight is the most prominent feature.
The weight loss is initially caused by the loss of fluid. Later on it is owing to
catabolism of tissues to meet energy needs. The body stores of carbohydrate
(liver and muscle glycogen) are depleted within two to three days and fat is
mobilized in the form of free fatty acids which is used as fuel by the muscles.
Glucose is spared for the brain. Tissue proteins are also broken down in order
to meet the energy needs. Protein synthesis is diminished and alanine is
released by the muscles to the liver for conversion to glucose, which is made
available to the brain. During prolonged starvation, brain metabolism can adapt
to use betahydroxybutyrate and acetoacetate also as fuel. Generalized emaciation
results. Liver and intestines are the first to lose
tissue, and
this is followed by muscles and skin. The brain is preserved right till the
end.
CLINICAL FEATURES
The patient
is apathetic and irritable. The loss of fat around the buttocks, thighs, back,
and buccal region gives the characteristic appearance with prominence of bones and
dry, thin, inelastic, loose skin. A brownish, patchy pigmentation is generally
encountered. The hair becomes characteristically dry and easily pluckable.
During cold weather cyanosis of extremities may develop. Systemic disturbances
Cardiovascular changes include bradycardia, lowered systolic and diastolic
pressure, and reduction in venous pressure and cardiac output. The heart size
is also reduced. Respiratory rate is lowered, so also the vital capacity.
Growth hormone level is decreased.
Basal metabolism
is lowered. Corticosteroid is normal. In both sexes sexual function is
diminished leading to loss of libido in males and amenorrhea in females. Hypothermia
may develop on exposure to cold. Though personality changes may be manifest,
the intellect usually remains clear till the end. Capacity for work is reduced due
to loss of muscle mass. Mild normocytic normochromic anemia is not uncommon.
In some
individuals dependent edema appears even without lowering of plasma albumin.
Nocturnal polyuria is common though the renal function is not grossly affected.
TREATMENT
The course
of treatment should depend upon the severity of the disorder. Mild cases of
starvation require only oral feeds. Overzealous dietary supplementation may
lead to diarrhea and death. In the early stages, gradual introduction of easily
absorbable and predigested food may be necessary till the alimentary functions
return to normal. Fats and fatty foods have to be avoided to prevent diarrhea.
Skimmed milk is superior to whole milk.
Skimmed milk
powder reconstituted to give 10-15% strength is well tolerated if given as
small feeds (up to 100 mL) frequently. A daily intake of about 3,000 kcal and
100 g proteins should be aimed at. Severely debilitated patients should be fed
using an intragastric tube in order to ensure adequate intake. After the
initial rapid gain in weight due to correction of dehydration, a steady increase
of 1-1.5 kg/week can be considered as adequate response. In all cases of severe
starvation especially if complicated by intercurrent illnesses and diarrhea, parenteral
nutrition should be resorted to without delay.
If starvation occurs on a wide scale, relief camps have to be organized to provide shelter, food, potable water and general sanitation. Community kitchens may have to be set up to provide food. In these endeavours, the medical personnel have to work in close liaison with social service organizations and governmental agencies.
STARVATION – General Characteristics, Clinical Features and Treatment