KWASHIORKOR – General Features, Pathology and Clinical Features
This name was coined by Dr Cicely Williams in 1933, to denote ‘disease of the child deposed from the breast by the conception of a new fetus’. Children between the ages of 1 and 3 years are affected more. The disease starts when the baby is weaned from the breast.
Pathology
Main changes are seen in the small intestines, liver, pancreas and thymus. Small intestinal mucosa shows blunting of villi and atrophy of brush border, so that the columnar epithelium appears to become cuboidal. The total absorbing surface is reduced. Lactose intolerance is common because of disaccharidase deficiency. Liver shows fatty infiltration of the parenchymal cells. The pancreatic acini are atrophic and enzyme activity is reduced. Thymus is markedly atrophied and this may contribute to deficiency of cell mediated immunity.
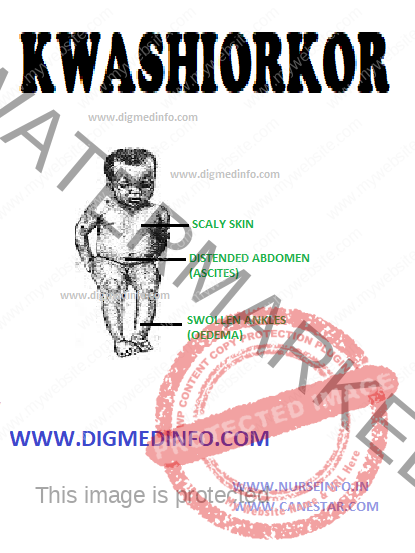
Clinical features
This child is stunted and skeletal muscles are wasted. The presence of fairly normal amounts of subcutaneous fat and edema give a deceptively plump appearance. Pitting edema is a prominent feature. The child is apathetic, irritable and drowsy. Characteristic skin changes occur in many and when present; these are diagnostic. These include flaky paint dermatosis seen over areas of pressure and trauma, fissuring and ulceration at the flexures and a mosaic like appearance (crazy pavement appearance). The hair becomes thin, sparse, brownish and lusterless. They may fall off. Regrowth of normal pigmented hair heralds nutritional recovery. Since periods of nutritional deprivation and partial correction of nutrition alternate in many cases, the hair shows alternate bands of pigmentation and depigmentation (flag sign). The appetite is poor. Diarrhea is a frequent feature. There may be concomitant deficiencies of iron, folate, fat soluble vitamins and B complex factors. Hepatomegaly occurs in a third of the cases. This is due to fatty infiltration. With recovery the liver reverts to normal without sequelae.