SvO2 MONITORING – Client
Preparation, Procedure, Interfering Factors, Complications and Steps to Prevent
Complication
In venous
oxygen saturation (SvO2) monitoring, a fiberoptic flow-directed
thermodilution pulmonary artery (PA) catheter measures SvO2. It
allows continuous monitoring of the body’s ability to deliver oxygen to
tissues. SvO2 measurements rapidly detect changes in hemodynamic
stability. They are also used to evaluate a client’s response to drug
administration, endotracheal tube suctioning, ventilator setting changes, and
positive end expiratory pressure. This technique can reduce the need for
frequent arterial blood gas levels, cardiac output, and other hemodynamic
measurements
CLIENT PREPARATION
Explain the procedure to the client
and his family
Make sure that they understand the
procedure’s risk (related to catheter placement, pneumothorax, and infection)
and expected outcomes
Inform the client that the catheter
placement procedure takes 15-30 minutes and that he must lie still during this
time
After catheter placement, his
movements will be restricted
Set-up and prime the equipment before
catheter insertion, according to the manufacturer instructions and facility
procedure and check catheter balloon patency and integrity
Turn on the co-oximeter and pressure
module for at least 10 minutes before insertion to allow them to warm-up. Set
the alarm parameters 10% above and 10% below the client’s baseline SvO2
PROCEDURE
During catheter insertion, monitor
the client’s vital signs and cardiac rhythm
Assess the changes in ventilator
status, possibly caused by the client’s dependent position and facial drapes
Talk to him during procedure to
provide reassurance and to assess for mental status changes
Record pressure reading during
insertion and any changes in the client’s condition
The PA catheter can be connected to
the optical module before or after insertion
Record the initial SvO2
recording and calibrate the o-oximeter to ensure accurate values
To calibrate, draw a mixed venous
blood sample for laboratory analysis; then compare the sample’s SvO2 reading
and attach selected strip to the chart as ordered
The nurse should watch carefully for
problems that can interfere with accurate testing, such as malfunctioning
recording device, loose connections, balloon rupture, and clot formation at the
catheter tip or in the fluid column
INTERFERING FACTORS
Excessive catheter movement (catheter
fling) caused by incorrect placement, leading to a dampened pressure tracing
Catheter migration against a vessel
wall, leading to constant occultation (permanent wedging) of the pulmonary
artery
Increased intrathoracic pressure,
which raises catheter pressure, caused by mechanical ventilation with positive
pressure
COMPLICATIONS
Pneumothorax
Pulmonary artery perfusion
Air emboli
Infection
STEPS TO PREVENT COMPLICATION
Change the sterile dressing every 24
hours. If the dressing becomes soiled, change it more often
Inspect the site for signs for
infection with each dressing change
Change the IV tubing every 24 hours
Maintain a heparin flush system by
verifying tight connections and gentle bubbling
Closely monitor the client’s
hemodynamic status
Be gentle when wedging the catheter
to prevent balloon rupture and pulmonary artery damages
SvO2 MONITORING – Client Preparation, Procedure, Interfering Factors, Complications and Steps to Prevent Complication
SKULL AND SPINAL X-RAY – General
Instructions, Procedure and After Care
A skull
X-ray is an imaging test doctors use to see the bones of the skull, including
the facial bones, the nose, and the sinuses. It is an easy, quick and effective
method that has been used for decades to help doctors view the area that houses
most vital organ. Skull X-ray studies reveal the size and shape of the skull
bones, suture separation in infants, fractures or bony defects, erosion,
calcification, sella turcica and pineal gland shift. Spinal X-ray studies show
fractures, dislocation, compressions, curvature, erosion, narrowed spinal cord
and degenerative processes
DEFINITION
Skull X-rays
are performed to examine the nose, sinuses, and facial bones. These studies may
also be referred to as sinus X-rays. X-rays studies produce films, also known
as radiographs, by aiming X-rays at soft bones and tissues of the body. X-ray
beams are similar to light waves, except their shorter wavelength allows them
to penetrate dense substances, producing images and shadows on film
Radiological
film taken at different planes of skull and various regions of spine is to
identify fractures, anomalies or possibly tumors
PURPOSES
Doctors may
order skull X-rays to aid in the diagnosis of a variety of diseases or injuries
Sinusitis:
sinus X-rays may be ordered to confirm a diagnosis of sinusitis, or sinus
infection
Fractures: a
skull X-ray may detect bone fractures resulting from injury or disease. The
skull X-ray should clearly show the entire skull, jaw bones, and facial bones
Tumors:
skull radiographs may indicate tumors in facial bones, tissues, or sinuses.
Tumors may be benign (not cancerous) or malignant (cancerous)
Other: birth
defects (referred to as congenital anomalies) may be detected on a skull X-ray
by changes in bone structure. Abnormal tissues or glands resulting from various
conditions or diseases may also be shown on a skull radiographs
Skull X-ray
To identify skull fracture
To detect the position of pineal body
To identify the unusual calcification
To conform the shape and size of
skull bones
To detect bone erosion
To identify abnormal vascularity
Spine X-ray
A
lumbosacral spine X-ray is a picture of the small bones (vertebrae) in the
lower part of the spine, which includes the lumbar region and the sacrum, the
area that connects the spine to the pelvis
To diagnose wedging of collapsed
vertebra
To detect erosion of bone called by
neoplasm
To identify irregular calcification
as a result of inflammatory process
To detect vertebral fractures and
dislocations
To detect spondylosis and spurs
To identify trauma to vertebral;
column
Description
Skull or
sinus X-rays may be performed in a doctor’s office that has X-ray equipment and
a technologist available. The exam may also be performed in an outpatient
radiology facility or a hospital radiology department. In many instances,
particularly for sinus views, the patient will sit upright in a chair, perhaps
with the head held stable by a foam vise. A film cassette is located behind the
patient. The X-ray tube is in front of the patient and may be moved to allow
for different positions and views. A patient may also be asked to move his or
her head at various angles and positions. In some cases, technologists will ask
the patient to lie on a table and will place the head and neck at various
angles. In routine skull X-rays, as many as five different views may be taken
to allow a clear picture of various bones and tissues. The length of the test
will vary depending on the number of views taken, but in general, it should
last about 10 minutes. The technologist will usually ask a patient to wait
while the films are being developed to ensure that they are adequate before
going to the radiologist
GENERAL INSTRUCTIONS
Some clients with neurological
disorders require nursing support throughout the X-ray study, especially
clients who are confused, combative or ventilator dependent
If the client has suspected spinal
fracture the neck is immobilized prior to moving the client to make X-ray films
Metal items should be removed from
body parts
Client
preparation: there is no preparation for the patient prior to arriving at the
radiology facility. Patients will be asked to remove jewelry, dentures, or
other metal objects that may produce artifacts on the film. The referring
doctor or X-ray technologist can answer any questions regarding the procedure.
Any woman who is or may be pregnant should tell the technologist
Explain the procedure to the client
in simple words
Remove jewelry, dentures, hairclips
and glasses
Send the client to X-ray department
in wheelchair or stretcher
Spinal precautions that are cervical
collar and strict maintenance of head alignment done for suspected neck
fracture
PROCEDURE
Place the client in proper
positioning
A lateral view of the cervical spine
is taken first with minimal movement to determine whether fracture has occurred
A C1 –C2 view is obtained by taking
the X-ray through the open mouth of the client
For C6-C7 views adequate
visualization often requires the nurse or technician to pull down firmly on the
client’s arms while the film is being taken
AFTER CARE
Transfer the client to the bed
Monitor the vital signs and
neurological status
Collect the X-ray and inform to the
consultant
Record the procedure in the nurse’s
record
Normal
results: normal results should indicate sinuses, bones, tissues, and other
observed areas are of normal size, shape, and thickness for the patient’s age
and medical history. Results, whether normal or abnormal, will be provided to
the referring doctor in a written report
Abnormal
results: abnormal results may include:
Sinusitis: air in sinuses will show
up on a radiograph as black, but fluid will be cloudy or white (opaque). This
helps the radiologist to identify fluid in the sinuses. In chronic sinusitis,
the radiologist may also note thickening or destruction of the bony wall of an
infected sinus
Fractures: radiologists may recognize
even tiny facial bone fractures as a line of defect
Tumors: tumors may be visible if the
bony sinus wall is distorted or destroyed. Abnormal findings may result in
follow-up imaging studies
Other: skull X-rays may also detect
disorders that show up as changes in bone structure, such as Paget’s disease of
the bone or acromegaly (a disorder associated with excess growth hormones from
the pituitary gland). Areas of calcification or gathering of calcium deposits,
or destruction may indicate a condition such as an infection of bone or bone
marrow (osteomyelitis)
SKULL AND SPINAL X-RAY – General Instructions, Procedure and After Care
PULSE OXIMETRY – Types of Oxygen
Transducers and Nursing Consideration
Pulse
oximetry offers a reliable, noninvasive, painless alternative to frequent
needle sticks usually required for arterial oxygen monitoring. The pulse
oximeter continuously tracks arterial oxygen saturation levels using
noninvasive light. A transducer (sensor) shines red and infrared light through
tissues when attached to the client’s body (e.g. finger or toe). A photo
detector records the relative amount of each color absorbed by arterial blood
and transmits the data to a monitor, which displays the information with each
heartbeat. Alarms sound if the oxygen saturation level or pulse rate exceeds or
drops below limits set by the user
The oximeter
eliminates delays associated with laboratory analysis of blood samples and
instantly alters you to changes in the client’s oxygen saturation levels so the
nurse can take immediate action. It also monitors pulse rate and amplitude and
can detect changes in the client’s oxygenation status within 6 seconds
TYPES OF OXYGEN TRANSDUCERS
The type
oxygen transducer used depends on the client’s age, size and clinical condition
Neonatal foot transducer
Infant toe transducer
Pediatric finger transducer
Adult finger transducer for clients
engaging in limited activity
Adult nasal transducer for inactive
clients (typically used during surgery)
Ear transducer
Forehead reflectance transducer
NURSING CONSIDERATION
The site selected for transducer
requires no special preparation. For best results with the ear transducer,
attach it to the fleshy parts of the earlobe, not on the cartilage
Attach a finger transducer to the
client’s index finger and keep the finger at heart level
Do not attach any transducer to an
extremity that has a blood pressure cuff or an arterial catheter in place; the
reduced blood flow will yield erroneous data
Protect the transducer from exposure
to strong light
Check the transducer site frequently
to make sure the device is in place and examines the skin for abrasion and
circulatory impairment
Rotate the transducer at least every
4 hours to avoid skin irritation
If oximetry has been performed
properly, the oxygen saturation readings are usually within 2% of arterial
blood gas values when saturations range between 84% and 98%
PULSE OXIMETRY – Types of Oxygen Transducers and Nursing Consideration
LUNG SCAN/PULMONARY SCINTIPHOTOGRAPHY
– Abnormal Finding, Client Preparation, Perfusions Scan, Ventilation Scans,
Post-Procedural Care, Contraindication and Interfering Factors
This nuclear
medicine procedure is used to identify defects in blood perfusion of the lung
in client’s with suspected pulmonary embolism. Blood flow to the lungs is
evaluated using a macroaggregated albumin (MAA) tagged with technetium (Tc),
which is injected into the patient’s peripheral vein. The diameter of the radionuclide aggregates
larger that of the pulmonary capillaries, the aggregates become temporarily
lodged in the pulmonary vasculature. A scintillator (gamma camera) detects the
gamma rays from within the lung microvascular. With the use of light
conversion, a realistic image of the lung is obtained on film
The chest
X-ray film aids in assessing the perfusion scan, because a defect on the
perfusion scan seen in the same area as an abnormality on the chest X-ray film
does not indicate pulmonary embolism. Specificity of a perfusion scan also can
be enhanced by performance of a ventilation scan, which detects parenchymal
abnormalities in ventilation (e.g. pneumonia, pleural fluid, emphysematous bullae).
The ventilation scan reflects the patency of the pulmonary airways, using
krypton gas or Tc-diethylnetriamine-pentaacetic acid (DTPA) as an aerosol
When
vascular obstruction (embolism) is present by perfusion, ventilation scan
demonstrate a normal wash-out of radioactivity from the embolized lung area. If
paranchymal disease (e.g. pneumonia) is responsible for the perfusion
abnormality, however, wash-in or wash-out will be abnormal. Therefore, the
mismatch of perfusion and ventilation findings is characteristic of embolic
disorders, whereas the match is indicative of parenchymal disease. When
ventilation and perfusion scan are performed synchronously, this is called a
ventilation/perfusion (V/Q) scan
ABNORMAL FINDING
Pulmonary embolism
Pneumonia
Tuberculosis
Emphysema
Tumor
Asthma
Atelectasis
Bronchitis
Chronic obstructive pulmonary disease
CLIENT PREPARATION
Explain the procedure to the client
Obtain informed consent if required
by the institution
Assure the client that he or she will
not be exposed to large amounts of radioactivity, because only tracer doses of
isotopes are used
Inform the client that no fasting is
required
Recent chest X-ray should be
available
Instruct the client to promote
jewelry around the chest area
PROCEDURE
The unsedated, nonfasting client
suspected of having a pulmonary embolism is taken to the nuclear medicine
department
PERFUSION SCAN
The client is given a peripheral IV
injection of radionuclide-tagged MAA
while client lies in the appropriate
position, a gamma ray detector is passed over the client and records
radionuclide uptake on Polaroid or X-ray film
the client is placed in the supine,
prone and various lateral positions, which allows for anterior, posterior,
lateral and oblique views, respectively
the results are interpreted by a
physician trained in diagnostic nuclear medicine
VENTILATION SCANS
the patient breathes the tracer
through a face mask with a mouthpiece
Less client cooperation is needed with
krypton tracer. Ventilation scans can be performed on comatose clients using
krypton. Krypton images can be obtained before during or after perfusion images
In contrast, Tc-DTPA images are
usually done before perfusion images and require client cooperation with deep
breathing and appropriate use of breathing equipment to prevent contamination
This test is usually performed by a
physician in approximately 30 minutes
Inform the client that no discomfort
is associated with this test than the peripheral venipuncture
POST-PROCEDURAL CARE
Apply pressure to the venipuncture
site
Inform the client that no radiation
precautions are necessary
CONTRAINDICATION
Clients who are pregnant, unless the benefit outweigh the
risks
INTERFERING FACTORS
Pulmonary parenchymal problems (e.g. pneumonia, emphysema, pleural effusion, tumors) will give the picture of a perfusion defect and stimulate pulmonary embolism
LUNG SCAN/PULMONARY SCINTIPHOTOGRAPHY – Abnormal Finding, Client Preparation, Perfusions Scan, Ventilation Scans, Post-Procedural Care, Contraindication and Interfering Factors
EVOKED POTENTIALS – Definition,
Purpose, Indication, Types of Evoked Potentials, Advantages, Client
Preparation, Procedure and After Care
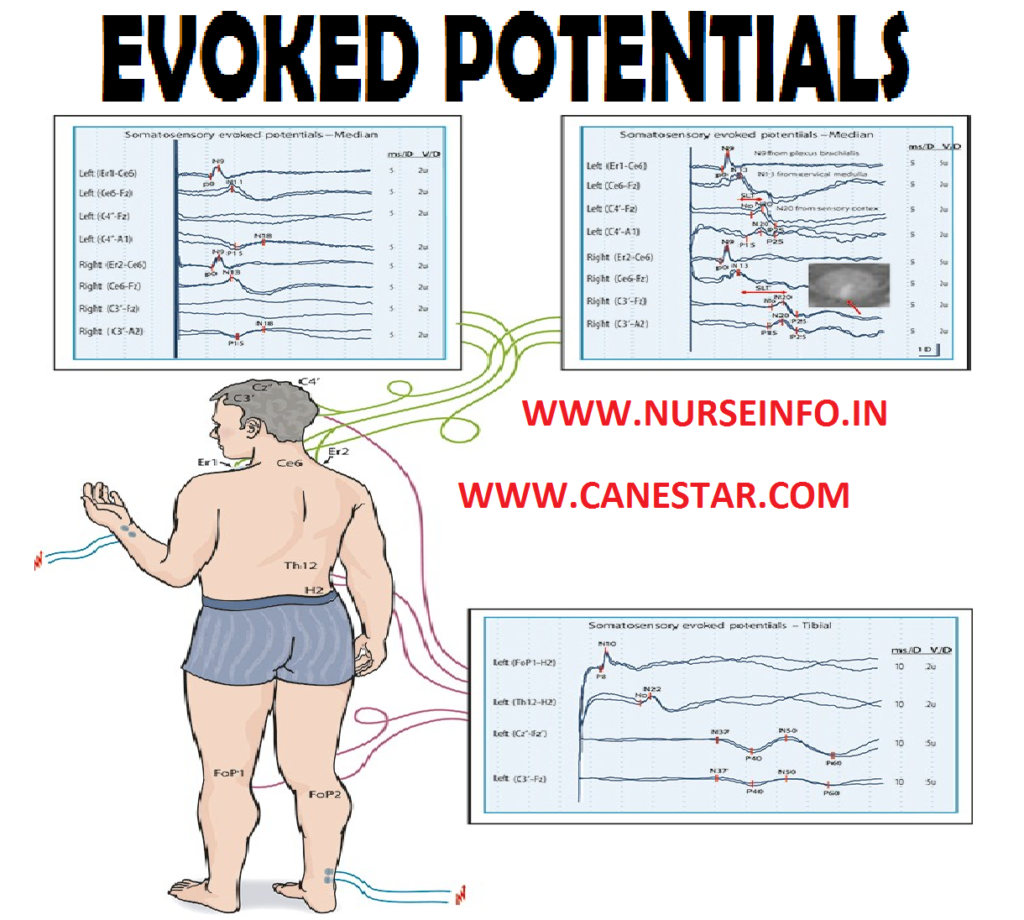
Evoked
potentials involve the recording of electrical impulses generated by a sensory
stimulus as it travels though the brainstem and into the cerebral cortex.
Measuring evoked potentials is a sophisticated way of observing the status of
sensory pathways as they enter the central nervous system, travel through the
midbrain and reach the cerebral cortex
DEFINITION
Evoke
potentials is a recording of electrical activity in central sensory pathways
produced by placing electrodes over the scalp or the spine and using a computer
to average and amplify the signal which results in characteristic pattern of
wave from peaks that have approximate anatomic correlates
PURPOSE
To observe the sensory pathway as
they enter the central nervous system, travel through the brainstem and reach
the cerebral cortex
Evoked potentials also used during
therapeutically induced comas such as barbiturate coma
Evoked potentials used in the
determination of the existence of brainstem or spinal cord injury in the
traumatically injured patient
It is used to assess the function of
the cerebral hemispheres and the brainstem
It is also used to assess blindness,
deafness and brainstem injury
INDICATIONS
Used in the diagnosis of multiple
sclerosis
Hypoxic coma
Spinal cord injury
Brainstem lesions
Acoustic neuroma
TYPES OF EVOKED POTENTIALS
Visual evoked responses (VER): it
involves monitoring of the visual pathways through the brainstem and cortex in
response to the patients viewing a shifting geometric pattern on a screen or
placing a mask, which sends a flashing light stimulates over the eye
Brainstem auditory evoked responses
(BAERs): It involves monitoring of the auditory pathway through the brainstem
and cortex in response to a rhythmic clicking sound sent through earphones placed
over the patient’s ears
Somatosensory evoked response (SSER):
it involves monitoring of sensory pathways from the extremities ascending the
spinal cord through the brainstem and into the cortex
ADVANTAGES
Evoked potential studies can detect
abnormalities even if the client is sedated or paralyzed with neuromuscular
blocking agents
Evoked potential studies are more
reliable than clinical assessments in predicting neurological recovery in
comatose, head-injured clients
CLIENT PREPARATION
Explain the procedure and provide
emotional support
Head should be washed with soap
Inform the client that he should be
awake during procedure
Do not apply oil over the head after
the bath
Provide good breakfast one hour
before evoked potentials
Provide hospital cotton dress to wear
PROCEDURE
Place the client comfortably on the
examination table
Evoked potentials studies are carried
out in the same fashion as EEGs
Clients brain waves are monitored by
giving various stimuli
A variety of types of stimuli are
used, such as auditory, somatosensory and visual
Typical stimuli include flashing
lights, buzzing tones and peripheral nerve stimulation
AFTER CARE
Monitor the vital signs and
neurological status
Record the entire procedure in
nurse’s record
EVOKED POTENTIALS – Definition, Purpose, Indication, Types of Evoked Potentials, Advantages, Client Preparation, Procedure and After Care
ELECTROENCEPHALOGRAM – Purpose,
Mechanism, Wave Patterns, Preliminary Assessment, Preparation of the Patient
and the Environment, Equipment, Procedure, Interpretation and Nursing
Implications
Electroencephalogram
(EEG) is a noninvasive procedure, in that electrodes are placed over the skull
in many areas and the electric activity of the various segments of the brain is
recorded
Electroencephalogram
is painless and a safe technique for evaluating the brain pathology such as
brain tumors, brain abscess and epilepsy
PURPOSE
To detect any abnormality in the
brain such as space occupying lesion (SQL)
EEG serves best to identify seizure
disorders by type and area of origin within the brain
To measure the cerebral oxygen,
glucose, and blood flow in the brain
MECHANISM
An EEG is an
instrument of electrical activity of the superficial layers of the cerebral
cortex. It demonstrates the electrical potentials from neuron activity, within
the brain in the form of wave patterns. The intensity and pattern of electrical
activity is influenced by the reticular activating system. The characteristics
of the wave depend on the degree of cortical activity
Brain
activity as recorded on an EEG correlates with the cerebral blood flow
A constant
supply of oxygen, blood and glucose is needed to meet the metabolic demands of
the brain. Decrease cerebral blood flow causes changes in mentation and
decreased electrical activity on the EEG
WAVE PATTERNS
Alpha: alpha waves are found during
period of wake-fullness, prominent over the cortical and parietal areas
Beta: beta waves are recorded with in
turns activation of the CNS, prominent over frontal and parietal areas
Theta: theta waves are recorded
during periods of emotional stress or drowsiness, prominent over the temporal
and parietal areas
Delta: delta waves are recorded
during periods of deep sleep
EEG Measures
in Seizure
Breathing deeply for several minutes
to produce alkalosis
Producing a sleep deprivation syndrome
Producing a sleep either naturally or
by drugs
Photostimulation by flashing lights,
etc
PRELIMINARY ASSESSMENT
Check
Doctors order for any specific
instructions
General condition or diagnosis of the
patient
Mental status of the patient to
follow instructions
PREPARATION OF THE PATIENT AND THE ENVIRONMENT
Explain the procedure to the patient
to gain cooperation. This procedure talks half an hour to two hours
The purpose of the test an procedure
should be explained to the client and the family
The client and family may need to be
reassured that electricity does not enter the brain
Air shampoo is indicated on previous
day, this helps the jelly to be fixed in the scalp
This test can be done in sitting or
lying position, so place according to the technician’s instructions
The client will be asked to relax
during the test, because anxiety can block alpha rhythms
The nurse should be sure to send
adequate supplies (i.e. intravenous fluids or oxygen to the laboratory)
The EEG room should be kept – quite,
minimum light, appropriate temperature and less distraction
The client may keep awake the night
preceding the test or sedation to induce sleep
EQUIPMENT
EEG machine with electrodes
Jelly
Tissue paper
Cotton balls
Bed with adequate linen
PROCEDURE
The patient is taken to an EEG room,
where the technician does this test
Electrodes are attached to the
client’s scalp
Electrodes are applied to the scalp
and the ear loop with collodion
Lead scan also be placed in
nasopharynx to assist disorders in the temporal lobe
The first portion of the test is
performed with the clients as relaxed as possible to obtain a baseline
recording
Further readings are taken while the
client is hyper-ventilating, sleeping or viewing flickering lights
The wave forms are amplified and
recorded on a moving paper strip, similar to an ECG
EEGs are interpreted according to
brain wave characteristics, frequency and amplitude
If the client is comatose or unable
to move, EEG can be performed at the bedside
Sleep may evoke abnormal EEG patterns
not present while the client is awake
Absence of EEG waves (flat line) on
EEG may be one of the criteria for defining brain death
NURSING IMPLICATIONS
The preparation of the patient for
EEG is extremely important because it can directly affect the accuracy of the
test results. The patient should be explained about the procedure and reassured
that EEG is no way painful and dangerous. He should be told tha tit is not a
form of shock treatment or a way of hypnotizing the patient
The explanation should be
satisfactory to the patient to win his confidence and cooperation. ‘TO RECORD
EEG, a relaxed and cooperative patient is necessary
Withhold all medications, especially
the nerve stimulants and depressants for 3 days prior to the test. This should
include tranquilizers, anticonvulsions, analgesics, hypnotics, and sedatives
The patient should not take coffee,
tea, alcohol, alcoholic beverages, etc. on the day of the test, since these are
stimulants to the central nervous system
The patient should not be disturbed
mentally before the test. Mental excitement and depression can alter the EEG
tracings
The patient should not sleep prior to
the test this may induce sleep in the patient during the procedure. Sometimes,
a sleep EEC is indicated to detect temporal lobe epilepsy. In such cases,
sedation is administered 45 minutes prior the EEG and the procedure is
performed when patient is sleeping
The hair should be cleaned thoroughly
with a shampoo. No oil or metal appliances should remain in the hair. No need
to cut the hair
ELECTROENCEPHALOGRAM – Purpose, Mechanism, Wave Patterns, Preliminary Assessment, Preparation of the Patient and the Environment, Equipment, Procedure, Interpretation and Nursing Implications
DOPPLER IMAGING – Definition,
Indications, Purposes, Advantages, Types, Client Preparation, Equipment,
Special Consideration, Procedure and After Care
Ultrasound
technology provides information about the flow velocity of blood through
cerebral vessels using non-invasive technique. A Doppler is placed externally
over the vessel, where ultrasonic waves are generated and blood flow velocities
are calculated
DEFINITION
Doppler
imaging is a noninvasive diagnostic method to study the flow velocity of blood
through cerebral vessels, specifically the circle of Willis
INDICATION
This procedure is used in the
intensive care unit to monitor clients who have experienced cerebrovascular
disorders, such as stroke, head trauma or subarachnoid hemorrhage
It can help detect intracranial
stenosis, vasospasm and arteriovenous malfunction as well as assess collateral
pathways
PURPOSE
To detect carotid artery disease such
as atherosclerosis arterial occlusion
To detect vertebral artery disease
such as stenosis or reversal of flow
To detect jugular vein disease such
as thrombosis or recanalization
ADVANTAGES
It is a noninvasive procedure, which
causes no pain
It is a safe procedure
It is relatively inexpensive
It has high accuracy
TYPES
Extracranial Doppler studies:
extracranial Doppler studies are used as a routine screening. It is used
monitor the intraluminal narrowing of the common and internal carotid arteries
as a result of arteriosclerotic plaques or atheromata
Transcranial Doppler studies:
transcranial Doppler studies monitor cerebral blood flow velocity through
cranial windows or thinned areas of the skull. One such area, the most popular
is the temporal bone
CLIENT PREPARATION
Prepare the client physiologically
and psychologically
Explain the entire procedure in
simple words
Inform the client not to move during
the procedure
EQUIPMENT
Transcranial Doppler unit
Transducer with an attachment system
Terry cloth headband
Ultrasonic coupling gel
Tissues
SPECIAL CONSIDERATION
Velocity changes in the transcranial
Doppler signal correlate with changes in cerebral blood flow. Parameter the
most clearly reflects this changes in the mean velocity
Embolus appears as high-intensity
transients that occur randomly during the cardiac cycle. Emboli make a
distinctive clicking, chirping or plunking sound
Various screens can be stored on the
system’s hard drive and can recall or printed
Before using the intracranial Doppler
system, be sure to remove turban head dressing or thick dressings over the test
site
PROCEDURE
Place the client comfortably on the
examination table
A Doppler probe is placed externally
over the vessel, where the ultrasonic waves are generated and blood flow
velocities are calculated
As the diameter of the vessel
changes, the velocity of the flow of the blood through the vessel changes
The Doppler probe represents the
velocity of the blood flow
These data are amplified, a graphic
and sound recording of the blood flow are produced
This procedure takes 15-45 minutes to
complete
AFTER CARE
Check the vital signs
Document the entire procedure in
nurse’s record
DOPPLER IMAGING – Definition, Indications, Purposes, Advantages, Types, Client Preparation, Equipment, Special Consideration, Procedure and After Care
COMPUTERIZED TOMOGRAPHY (BRAIN) –
Definition, Purposes, Indications, Preparation of the Client, Procedure, After
Care, Complications, Contraindications, Side Effects and Advantages
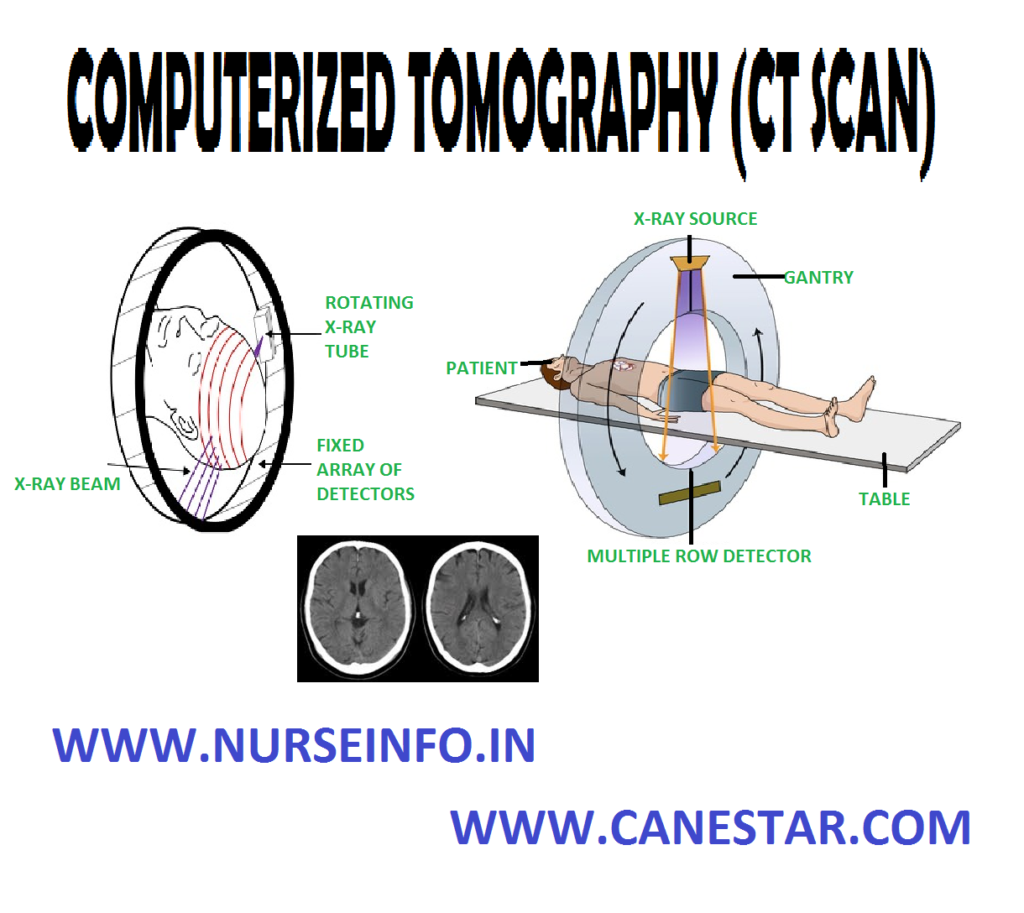
Computerized
tomography (CT) scan was developed by Godfry Hounsefield, a British physicist
in 1972, for this invention he was awarded Nobel Prize in 1978. In theoretical
basis of this technique was provided by Indian biophysicist Gopalsamudian N.
Ramachandran. CT scan is 100 times more sensitive than the conventional X-ray so
it detects a fine structure and small changes in density
DEFINITION
Computerized
tomography is a computerized X-ray procedure used to obtain detailed images of
structures within a selected plane of the body. The computer calculates the
amount of X-ray penetration of each tissue and displays this image in shades of
grey color
PURPOSE
It provides precise anatomical and
pathological information
Surgical procedures can be done by
using CT-guided procedure, e.g. biopsy
It provides a complete image which
helps to decide surgical intervention
To detect intracranial tumors
INDICATIONS
Space occupying lesions
Primary and secondary tumors
Cerebral edema
Intracranial hemorrhages
Arteriovenous malfunction
Infarctions and aneurysms
PREPARATION OF THE CLIENT
Explain the procedure to the patient
and to the relatives
Obtain a written consent form the
patient or relatives
Detailed allergic reactions such as
iodine
Jewelry, eye glasses and metal
objects shall be removed from the head
No dietary restrictions if contrast
is not given
If contrast is planned, the client
should keep fasting overnight
For children and restless patients,
sedation may be given
Explain the side effects, which may
occur during the procedure
Arrange emergency medications and
articles ready
For some children or adults who are
not cooperating or having involuntary movements, CT-scan may be done under
general anesthesia
Before radioplaque contrast medium is
administered, a skin test to be done to check the allergic reactions
During contrast administration ask
the client to take deep breathing till the injection is completed
PROCEDURE
Place the client comfortably on the
table
Inform the client not to move during
the procedure
Assist the administration of dye
Place the client’s face uncovered and
head immobilized
The head is scanned numerous times at
different angles
CT scan gives three-dimensional parts
The entire procedure lasts for 15-30
minutes
AFTER CARE
Observe the client who received
contrast medium for allergic reactions
Patients who had CT scan under
general anesthesia is kept on IV fluids and nothing per month for a few hours
Encourage more fluid intake to
minimize dehydration caused by fasting
Maintain an intake and output chart
promptly
Check the vital signs
COMPLICATIONS
Local and systemic allergic reactions
Spasm or occlusion of the vessels by
a clot
Bleeding at the injection site
Hematoma formation
Cardiac arrest
CONTRAINDICATIONS
Hyperthyroidism
Hypersensitivity to iodine contrast
media
SIDE EFFECTS
It mainly
caused due to the use of iodinated contrast
Nausea and vomiting
Erythematic and sensation of pain
A general feeling of warmth
Chills, fever, sweating and headache
Dizziness, weakness, and suffocation
ADVANTAGES
It is a painless and safe procedure
It provides detailed information for
diagnosis
The cost is reasonable
It can be performed on both conscious
and unconscious patients
Radiation exposure is relatively low
compared to that of skull films
COMPUTERIZED TOMOGRAPHY (BRAIN) – Definition, Purposes, Indications, Preparation of the Client, Procedure, After Care, Complications, Contraindications, Side Effects and Advantages
COMPUTERIZED TOMOGRAPHY – Reference
Values, Purposes, Indications, General Instructions, Nursing Considerations,
Nursing Care Before the Procedure, Procedure, Nursing Care After the Procedure,
Interfering Factors and Contraindications
Computed
tomography (CT) scan provides cross-sectional views of the chest by passing and
X-ray beam from a computerized scanner through the body at different angles and
depths. The CT scan provides a three-dimensional image of the lungs, allowing
the doctor to visualize the abnormalities.
Contrast
agents sometimes used to highlight blood vessels and to allow greater visual
discrimination. By using computer to regulate the layers or slices of tissue
examined, the camera rotates in a circular pattern and three-dimensional
assessment of the thorax (or other body area) is possible. Still photographs
are taken at each level. CT is able to visualize most abnormalities but small
early lesions may be missed
REFERENCE VALUES
Normal size, position, and shape of
chest organ tissue and structures; no tumors, cysts, infection or inflammation,
aneurysm, enlarged lymph nodes or fluid accumulation
PURPOSE
Often CT studies are done before and
after the intravenous administration of a contrast containing a radioactively
CT scans are particularly helpful in
identifying peripheral (pleural) or mediastinal disorders
Spiral or helical CT scan of the
chest is an alternative to the lung scan for identifying pulmonary emboli
INDICATIONS
Configuration of the trachea or major
bronchi and evaluate masses or lesions
Tumors and abscesses
Abnormal lung shadows
GENERAL INSTRUCTIONS
Computerized tomography scans
highlight differences in bone and soft tissue
The images are generated by
computerized synthesis of X-ray data obtained in many different direction in a
cross-sectional plane or slice
The computerized data are assembled
as three-dimensional images
CT is used to identify
space-occupying lesions (masses) and shifts of structures caused by neoplasm’s,
cysts, focal inflammatory lesions and abscesses of chest
To distinguish normal tissue from
abnormal masses, a contrast medium (dye) may be administered
The CT-scan can be performed quickly,
within 20 minutes
NURSING CONSIDERATIONS
Before a CT-scan, make sure that the
client has given informed consent and answer any questions about the procedures
Explain the fasting usually is not
required for a CT scan of the chest, but ask whether or not the client becomes
nauseated easily; if so, adjust foot and fluid intake accordingly
Inform the client, placed in supine.
The technician moves the table from a control room to direct the study to
different areas
Inform the client, he can expect to
hear mechanical noises coming from scanner
Some clients may feel claustrophobic
during the test, but assure them that it is possible to communicate with the
technician
Emphasize that the client must remain
still during the scan. Unable to comply, sedation is needed
After the test, assess the client for
reactions to the contrast agent, and the quality of pulses in the limb used for
injection of the contrast agent
The client may be resume normal
activities unless additional diagnostic tests are planned
NURSING CARE BEFORE THE PROCEDURE
Inform the client that the study
takes about 30 minutes to 1 hour
Obtain a history that includes
cardiac and pulmonary assessment findings, known or suspected pulmonary
conditions, and results of associated laboratory tests and diagnostic
procedures
PROCEDURE
The scanner takes images at different
levels and angles of the chest region, from the neck to the waist instead of
the whole body
Contrast-enhanced studies are
performed by the IV administration of an iodinated contrast medium for vessel
evaluation or by oral administration of a contrast medium for esophageal
evaluation
NURSING CARE AFTER THE PROCEDURE
Monitor
vital signs if the client has a acute or chronic cardiac or pulmonary condition
INTERFERING FACTORS
Inability of client to remain still
during procedure
Metal objects such as jewelry within
the examination field
CONTRAINDICATIONS
Pregnancy, unless the benefits of
performing the study greatly outweigh the risks to the fetus
Allergy to iodine, if an iodinated
contrast medium is to be used
Extreme obesity
Unstable medical status, i.e. vital
signs or dehydration
Extreme claustrophobic response that
prevents the client from remaining still during procedure, unless medications
are given before the study
COMPUTERIZED TOMOGRAPHY – Reference Values, Purposes, Indications, General Instructions, Nursing Considerations, Nursing Care Before the Procedure, Procedure, Nursing Care After the Procedure, Interfering Factors and Contraindications
ULTRASONOGRAPHY – Purpose,
Preoperative Care, Post-Procedural Care and Potential Complications
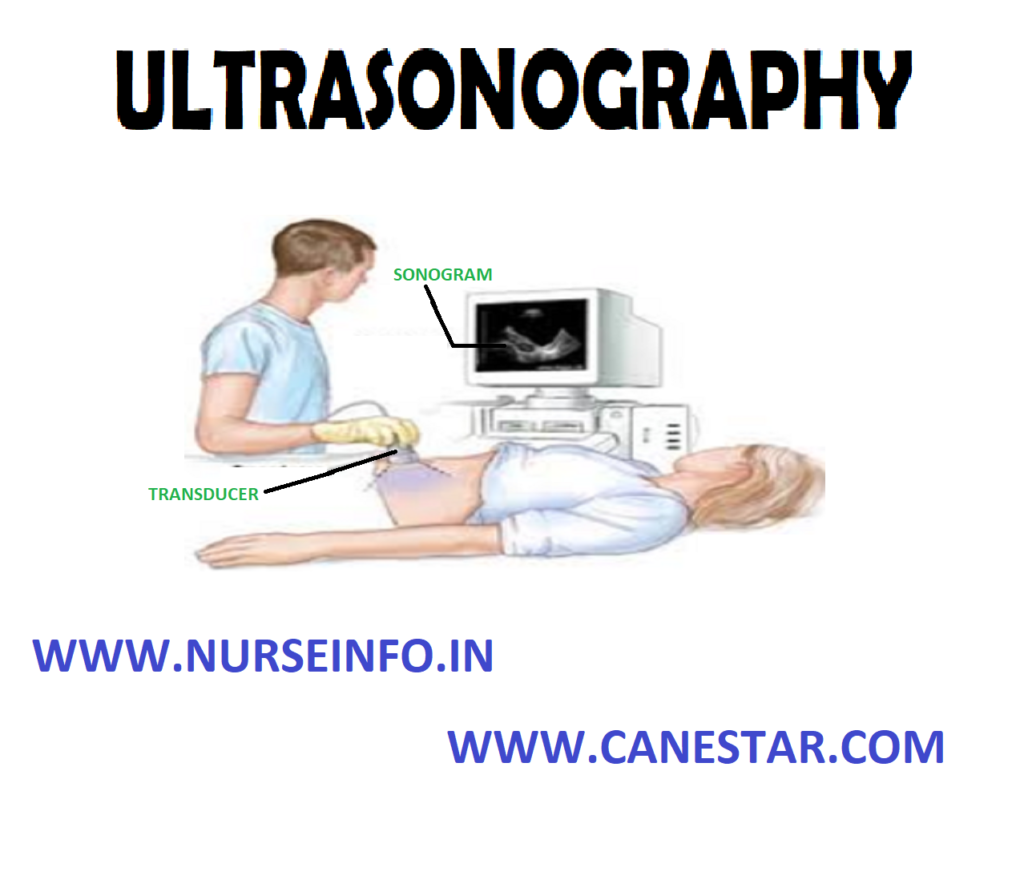
Ultrasonic
waves (sound waves too high in frequency for a human ear or detect) are used
diagnostically to assess various body structures. The waves are directed at the
organ or structure, and as they vibrate back from the target, they are
transducer into oscilloscope tracing.
Sonography
may be used in conjunction with other pulmonary diagnostic procedures such as
thoracentesis or pleural biopsy to assess fluid or fibrotic abnormalities
PURPOSE
Ultrasonography is especially helpful
and very accurate in detecting the amount and location of 50ml or less of
pleural fluid. In comparison, a positive detection by chest radiography
requires at least 500 ml of liquid
If the technique is used in
combination with thoracentesis, the ultrasonographer can determine the best
location for the needle placement as well as the depth of the fluid
Ultrasonography facilitates obtaining
an adequate amount of fluid for laboratory analysis without unnecessary
punching and probing
PREOPERATIVE CARE
No special care is required before
ultrasonography. Explain the purpose of the test and what to expect
A gel is applied to the skin, a
transducer (a device that changes reflected high-frequency sound to electrical
energy) is moved on the skin surface above the target organ
Inform the client that the procedure
is painless and fairly quick
Procedure: a
lung angiogram is administered by inserting a thin tube, or catheter into a
vein leading to the lungs. This tube is then guided to the area that requires
studying after which the iodine is injected in order to provide a contrasting
color of the veins on the final X-ray. During the procedure, you are probably
going to be asked to put on a lead gown to protect the genital and pelvic areas
from X-ray exposure and a round cylinder or rectangular box that captures the
images will be passed over the targeted area
The clients are placed on an X-ray
table in the supine position
Electrocardiography electrodes are
attached for cardiac monitoring
The catheter is placed into the
femoral vein and passed into the inferior vena cave
With fluoroscopic visualization, the
catheter is advanced to the right atrium and the right ventricle
The catheter is manipulated into the
main pulmonary artery, where the dye is injected
X-ray films of the chest are immediately
taken in timed sequence. This allows all vessels visualized by the injection to
be photographed. If filling defects are seen in the contrast-filled vessels,
pulmonary emboli are present
If bronchial artery is performed, the
femoral artery is cannulated instead of the vein
During injection of dye, inform the
client he or she will feel a burning sensation and flush throughout the body
POST-PROCEDURAL CARE
Observe the catheter insertion site
for inflammation, hemorrhage and hematoma
Assess the client’s vital signs for
evidence of bleeding (decreased blood pressure, increased pulse)
Apply cold compress to puncture site
if needed to reduce swelling or discomfort
Inform the client that coughing may
occur after this study
Educate the client regarding the need
for bed rest for 12 to 24 hours after the test
POTENTIAL COMPLICATIONS
Allergic reaction to iodinated dye
Hypoglycemia or acidosis may occur in
clients who are taking metformin (glucophage) and receive iodine dye
Cardiac arrhythmia: premature
ventricular contractions during right-sided heart catheterization may lead to
ventricular tachycardia and ventricular fibrillation
Contraindication:
CT pulmonary angiogram (CTPA) is less desirable in pregnancy due to the amount
of ionizing radiation required, which may damage the breasts, which are
particularly sensitive during pregnancy, and because of concerns of the effects
of iodine on the fetus’ thyroid gland. Nevertheless, CTPA is generally
preferred to isotope studies in pregnancy, due to the lower radiation dose to
the fetus.
Diagnostic algorithms for pulmonary embolism in pregnancy vary; however, a common compromise is to perform ultrasound testing for deep vein thrombosis of the legs, and if this is positive, make the diagnosis of pulmonary embolism on the basis of symptoms and presence of the DVT. CTPA would then only be performed if exhaustive non-radiation based testing could not make a positive diagnosis
ULTRASONOGRAPHY – Purpose, Preoperative Care, Post-Procedural Care and Potential Complications