In order to improve drug delivery, to
prolong the duration of action and thereby improve patient compliance, special
drug delivery systems are being tried. Drug targeting, i.e. to deliver drugs at
the site where it is required to act is also being aimed at, especially for
anticancer drugs. Some such systems are ocusert, progestasert, transdermal
adhesive units, prodrugs, osmotic pumps. Computerized pumps and methods using
monoclonal antibodies and liposomes as carriers.
Ocusert : Ocusert systems are thin elliptical units that contain the drug in a reservoir which slowly releases the drug through a membrane by diffusion at a steady rate, e.g. pilocarpine ocusert used in glaucoma is placed under the lid and can deliver pilocarpine for 7 days.
Progestasert is inserted into the uterus
where it delivers progesterone constantly for over 1 year.
Transdermal adhesive units:
Prodrug is an inactive form of a drug
which gets metabolized to the active derivative in the body. A prodrug may
overcome some of the disadvantages of the conventional forms of drug
administration, e.g. dopamine does not cross the BBB; levodopa, a prodrug
crosses the BBB and is then converted to dopamine in the CNS. Prodrugs may also
be used to have a longer duration of action, e.g, Bacampicillin (a prodrug of
ampicilin) is longer acting.
Osmotic
pumps are small tablet-shaped units containing the drug and an osmotic
substance in two different chambers. The tablet is coated with a semipermeable
membrane in which a minute laser-drilled hole is made. When the tablet is
swallowed and reaches the gut, water
enters into the tablet through the semipermeable membrane. The osmotic
layer swells and pushes the drug slowly out of the laser-drilled orifice.
This allows slow and constant delivery
of the drug over a long period of time. It is also called gastrointestinal
therapeutic system (GITS). Some drugs available in this formulation are iron
and prazosin.
Computerized miniature pumps: These are programmed to release drugs at a definite rate either continuously as in case of insulin or intermittently in pulses as in case of GnRH. Various methods of drug targeting are tried especially for anticancer drugs to reduce toxicity.
Monoclonal
antibodies are antibodies against the tumor specific antigens are used to
deliver anticancer drugs to specific tumor cells.
Liposomes are phospholipids suspended in aqueous vehicles to form minute vesicles. Drugs encapsulated in liposomes are taken up mainly by the reticuloendothelial cells of the liver and are also concentrated in malignant tumors. Thus site-specific delivery of drugs may be possible with the help of liposomes.
Nurses Responsibility:
Ensure that the correct drug is
administered by the right route and in the right dose.
History of allergy should be taken
particularly before parenteral administration of drugs
Monitor the adverse effects
Drugs should be kept in a safe place
Check the prescription, drug label
and the patient’s name before the administration of drugs.
SPECIAL DRUG DELIVERY SYSTEM – Ocusert, Transdermal adhesive units, Computerized miniature pumps, liposomes, nurse responsibility
Rectum has a rich blood supply and drugs
can cross the rectal mucosa to be absorbed for systemic effects. Drugs absorbed
from the upper part of the rectum are carried by the superior hemorrhoidal vein
to the portal circulation (can undergo first pass metabolism), while that
absorbed from the lower part of the rectum is carried by the middle and
inferior hemorrhoidal veins to the systemic circulation. Drugs
like-indomethacin, chlorpromazine diazepam abd paraldehyde can be given
rectally. Some irritant drugs are given rectally as suppositories.
Advantage
Gastric irritation is avoided
Can be administered by unskilled
persons
Useful in geriatric patients and
others with vomiting and those unable to swallow
Disadvantages
Irritation of the rectum can occur
Absorption may be irregular and
unpredictable
Drugs may
also be given by rectal route as enema.
Enema is the administration of a drug in a liquid form into the rectum. Enema may be evacuant or retention enema.
Evacuant enema: In order to empty the bowel, about 600 mL of soap water is administered rectum while soap lubricates. Enema is given prior to surgeries, obstetric procedures and radiological examination of the gut.
Retention enema: The drug is administered with about 100 mL of fluids and is retained in the rectum for local action, e.g. prednisolone enema in ulcerative colitis.
Drugs may be administered as suppository
for rectum, bougie for urethra and pessary and douche for vagina. Pessaries are
oval shaped tablets to be placed in the vagina to provide high local
concentrations of the drug at the site, e.g. antifungal pessaries in vaginal
candidiasis.
TOPICAL
Drugs may be applied on the skin for action as ointment, cream, gel, powder, paste, etc. Drugs may also be applied on the mucous membrane as in the eyes, ears and nose as ointment, drops and sprays.
RECTAL & TOPICAL ROUTE OF DRUG ADMINISTRATION – Advantages & Disadvantages
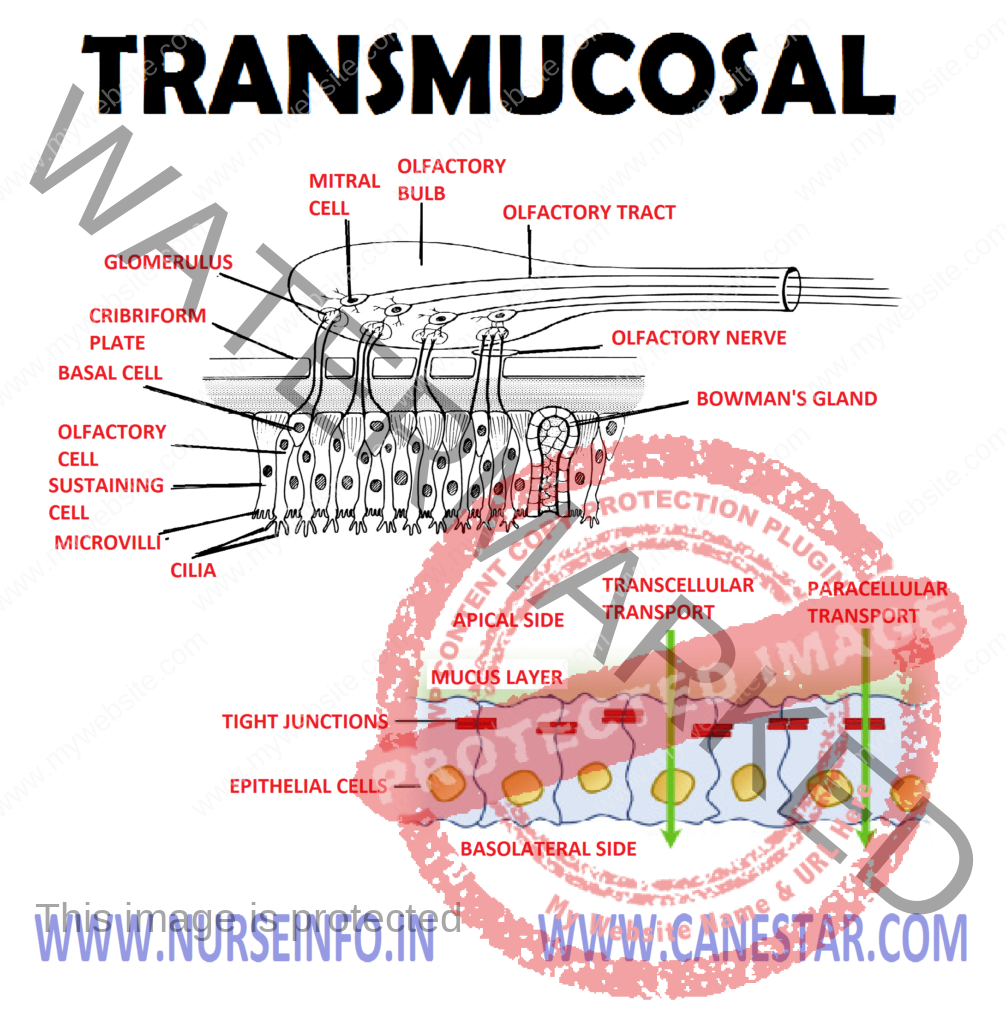
Transmucosal administration includes
sublingual, nasal and rectal routes
Sublingual: here the tablet or pellet
containing the drug is placed under the tongue. It dissolves and the drug is
absorbed across the sublingual mucosa, e.g. nitroglycerine, nifedipine,
buprenorphine
Advantages
Absorption is rapid – within minutes
the drug reaches the circulation.
First pass metabolism is avoided
After the desired effect is obtained,
the drug can be spat out to avoid the unwanted effects.
Disadvantages
Buccal ulceration can occur.
Nasal drugs
can be administered through nasal route either for systemic absorption or for
local effects. For example:
Oxytocin spray is used for systemic
absorption
For local effect – decongestant nasal
drops, e.g. oxymetazoline; budesonide nasal spray for allergic rhinitis.
Highly lipid
soluble drugs can be applied over the skin for slow and prolonged absorption,
e.g. nitroglycerine ointment in angina pectoris. Adhesive units, inunction,
iontophoresis and jet injection are some forms of transdermal drug delivery.
Adhesive
units (transdermal therapeutic systems) are adhesive patches of different sizes
and shapes made to suit the area of application. The drug is held in a
reservoir between an outer layer and a porous membrane. This membrane is
smeared with an adhesive to hold on to the area of application. The drug slowly
diffuses through the membrane and percutaneous absorption takes place. The rate
of absorption is constant and predictable. Highly potent:
Pulmonary epithelium and mucous
membranes of the respiratory tract and are also absorbed through these membranes.
(because small quantity is sufficient) and short acting (effect terminates
quickly after the unit is removed) drugs are suitable for use in such systems
Sites of application are chest,
abdomen, upper arm, back or mastoid region, e.g. hyoscine, nitroglycerine
fentanyl, estrogen, testosterone transdermal patches
Advantages
Duration of action is prolonged
Provides constant plasma drug levels
Patient compliance is good
Inunction: in this route of
administration, the drug is rubbed into the skin and it gets absorbed to
produce systemic effects
Iontophoresis: in this procedure,
galvanic current is used for bringing about penetration of lipid insoluble
drugs into the deeper tissues where its action is required, e.g. salicylates.
Fluoride iontophores is used in the treatment of dental hypersensitivity
Jet injection as absorption of drug
occurs across the layers of the skin, dermojet may also be considered as a form
of transdermal drug administration
TRANSDERMAL ROUTE OF DRUG ADMINISTRATION – Advantages and Purpose
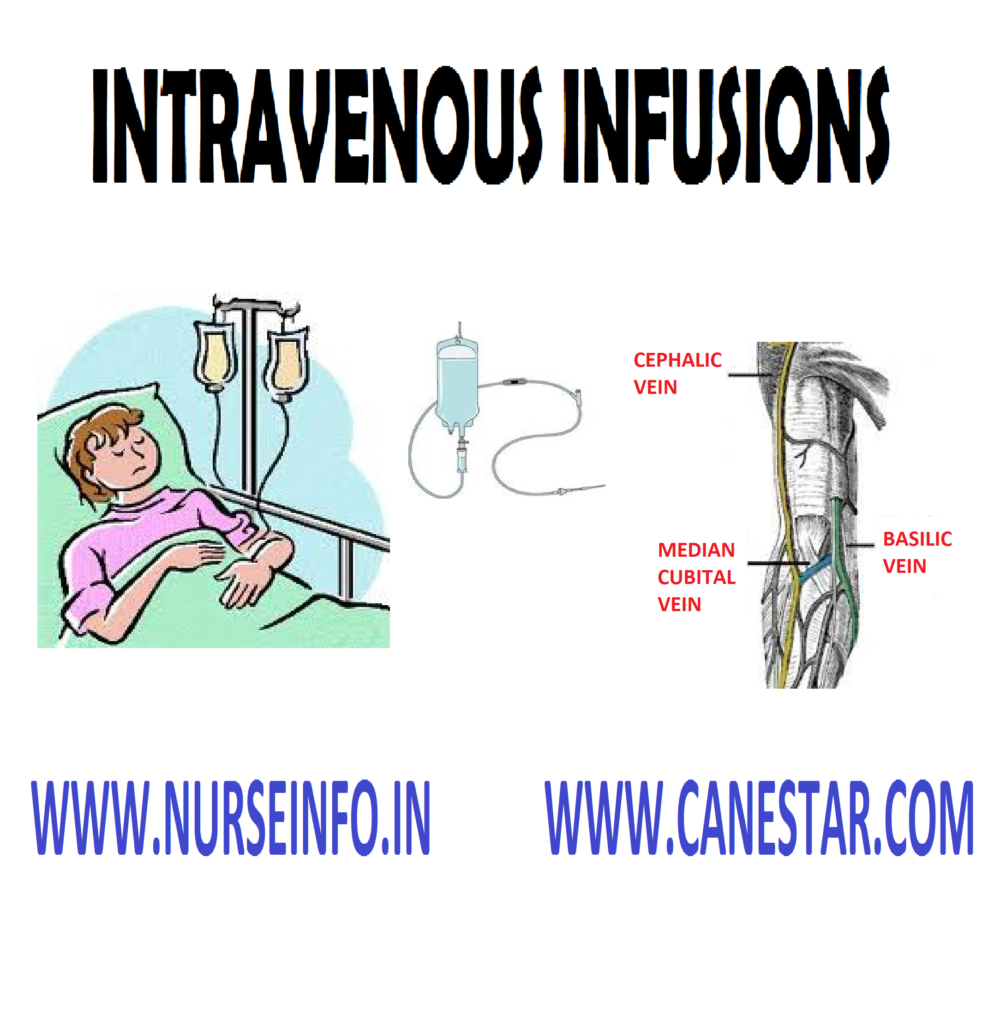
An
introduction of a large amount of fluid into body via veins is called as
intravenous infusion
Intravenous
infusion is puncturing vein with sterile cannula/needle into a vein to supply
the body with fluids electrolyte, nutrients and medication
Purpose
To supply fluids and electrolytes
To restore fluid volume due to
dehydration, hemorrhage, vomiting, diarrhea, etc
To meet patient’s basic requirements,
e.g. calories, vitamins, etc
To maintain homeostatic balance
To treat in emergency conditions some
medications are given intravenously
To prevent and treat shock and
collapse
Indication
To save the patients in
life-threatening situations, e.g. extensive burns
To introduce a drug into the
circulation for diagnosis purpose, e.g. IVP (intravenous pyelogram)
To supply fluids and nutrients to the
patients who are unable to digest or absorb a diet administered mouth or
through the nasal tube
To dilute toxins in case of toxemia
or septicemia
When blood or blood products are to
be given, e.g. anemia, hemorrhage
Solutions Used
Isotonic solutions: sodium chloride 0.9% commonly used
Hypotonic solutions or buffer substances sodium/potassium, calcium chlorides and lactic acid
Nutrient solutions dextrose 5, 10, 25, 50%
Alkalinizing and acidifying solutions
Blood volume expanders: plasma substitute and contains large molecular substances, e.g. dextran, lomodex, hemocoele, etc
Factors Affecting Fluid Movement
Diffusion molecules move from a solution of higher concentration to solution of lower concentration. Increase in the temperature increases the rate of diffusion
Osmosis: the diffusion water molecules through a permeable membrane from an area of lesser solute concentration
Hydrostatic pressure: it is the pressure exerted by a fluid within a closed system. Counter balancing the osmotic pressure of the plasma, which attract fluid into the vascular system
Dialysis: the diffusion of molecules of soluble constituents through a permeable membrane is known as dialysis
Filtration: it may be defined as the passage of fluids and dissolved substances across membranes because of differences in mechanical pressure on two sides of the membrane
Selective permeability of membranes: in body, the capillary and the cell membranes are described as selective permeable
Factors that Favors Absorption
Warmth: application of heat over the
site of injection or the use of warm solution
Massaging: massaging the part gently
increases the local supply and increase absorption
Diffusibility and solubility of the
drug
Venipuncture Site
The
selection of site depends upon following facts:
The condition of veins
The characteristics of tissues over
the vein
Purpose and durations of infusions
The type and amount of IV fluids
ordered
The diagnosis and general condition
of the patient
The commonly
used veins are:
Basilic and cephalic veins (forearm)
Median cubital, cephalic and basilica
veins (antecubital fossa)
Radial vein (radial area)
Dorsal metacarpal veins (the hand)
Veins in the foot
Femoral and saphenous veins (thigh)
Veins in the scalp (for infants)
Complications of IV Infusion
Circulatory overload: the intravascular compartment contains more fluid than the normal. Circulatory overload results in cardiac failure and pulmonary edema
Infiltration: it is the escape of fluid into the subcutaneous tissues due to dislodgement of needle
Hematoma formation: the walls of blood vessels may be damaged due to careless introduction of the needle into the body
Thrombophlebitis: it is caused by mechanical trauma to the vein or the chemical irritation of some substances introduced into the veins such as potassium chloride
Pyrogenic reactions: it is characterized by temperature elevation, chills, headache, nausea, vomiting and circulatory collapse in severe cases
Air embolism: the vascular collapse occurs due to occlusion of the vessel by embolism. The signs of pulmonary embolism are dyspnea, cyanosis, low blood pressure, shock and collapse, tachycardia and unconsciousness
Infection at the needle site: contamination occurs during insertion or left exposed for a long period
Serum hepatitis: infectious hepatitis has been attributed to improperly disinfected syringes and needles
Allergic reaction: this may due to certain drugs administered along with the IV fluids
Fluid Rate Calculation
Flow rate = total
volume infused in ml (multiply) drops/ml //total time of the infusion in
minutes
Total volume
infused = 200 ml in 24 hours
Drops per ml
= 15
Total time
in minutes = 24 (multiply) 60 = 1440 minutes
Flow rate =
2000 (multiply) 15 /144 = 16.6 drops
General Instructions
Follow strict aseptic technique
throughout the procedure
Administer IV fluids only with a
clearly written prescription
Maintain the specified rate of flow
to prevent circulatory overload
Constant and continuous observation
for any unfavorable symptoms
Observe the rights during
administration
Check the expiry date before opening
the bottles
If fluids are discolored, cloudy in
appearance that should not be used for infusion
Do not use any site that is tender,
red, edematous and inflamed
Never allow the bottle to get empty
completely to prevent the entry of air into the tissues
Keep the patient warm and comfortable
with blankets if necessary
Immobilize the joints with splints
when the needle is placed near a joint
Frequent observation of the vital
signs throughout the procedure will help to detect many complications
Allow the patient to void before the
IV infusion is started
Observation Needed Throughout the Procedure
Flow rate and potency of IV tubing
Dislodgement of needle
Signs of circulatory over load
Urinary output
Needle site
Fluid level in the bottle
Vital signs at frequent intervals
Preliminary Assessment
Check
Patients name, age, bed number and
diagnosis
Purpose of infusion
Doctors order
Level of consciousness
General conditions
Abilities and limitation
Need for additional restraints
Articles available
Previous experience
Equipment
A tray
containing
Sterile IV solution
Sterile IV infusion set
Sterile needle of choice (butterfly
or cannula)
Sterile syringe (2 or 5 ml)
Sterile transfer forceps in a jar
Sterile cotton swabs and gauze pieces
Surgical spirit
Kidney tray and paper bag
Bowl with water
Tourniquet
Adhesive tape and scissors
Specimen bottles
Mackintosh and towel
IV pole
Restrainer (Splint with roller
bandages)
Preparation of the Patient and Environment
Explain the procedure
Sent the visitors outside
Provide privacy
Allow the patient to empty the
bladder
Check the vital signs
Adjust the height of the bed
Arrange the articles at the bedside
Place the patient in comfortable and
relaxed position
Provide adequate light in the room
Procedure
Hand wash
Prepare the IV solution; insert the
drip set, and the air vent into the bottle openings
Hand the bottle on the IV pole about
18 to 24 inches high
The patient is placed in supine or
sitting position with head titled back
Draw the lower lid and ask the
patient to look up
Instill the ordered number of drops
in the center of the lower lid 2 cm above the eyes
After instillation, ask the patient
to close the eye and move eye balls from side so that medications will spread
all over the sac
Wipe of excess medication
After Care
Dry lids with dry cotton swabs
Make the patient comfortable
Remove articles from bed side
Hand wash
Record the procedure in the nurse’s
record
Patient Education
If the patient is on self-medication,
give him clear instructions and make sure that he is clear of it
Ask the patient to consult the doctor
regularly
Do not massage the eyeball after
instillation of medications
Complications
Improper dressing and procedure may lead to further serious infection
INTRAVENOUS INFUSIONS – Purpose, Instructions, Equipment, After Care, Procedure, Complications, After Care, Patient Education, Assessment
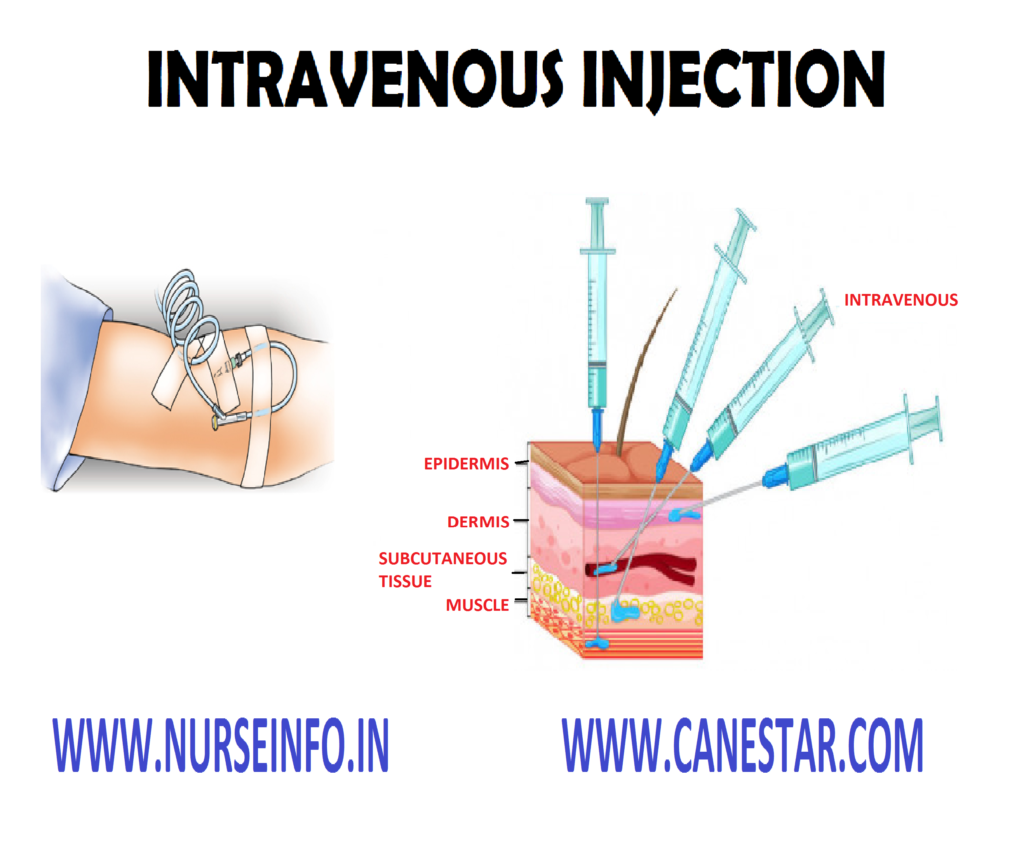
Intravenous
injection (IV) is the introduction of a small quantity of drug into the vein by
venous puncture
Introduction
of drug directly into the bloodstream is called intravenous injection
Purpose
To have a fast action of the medicine
as in emergency
To give medicines those are
irritating or ineffective when given by other routes
To have the action of medicines on
the blood stream or the blood vessels
Common Sites for IV Injection
Ventral aspect of elbow or forearm
median cubical, basilica or cephalic veins
Doral aspect of hand – branchial,
cephalic or metacarpal veins
In the infants the scalp vein is used
General Instructions
Expel the
air from the syringe before giving the injection by holding it in upright
position and gently pressing the piston until a drop of solution comes to the
tip of the needle
Always dissolve the drug in correct
amount of fluid to minimize the risk of adverse effect of the medicine
Observe the patient closely for the
signs of adverse reaction of the medicine and have emergency drugs and the
antidote in hand while injecting the medicine
Do not give the medicine if the
injection site shows any edema or intravenous solution is not following
properly to avoid accidental administration of medicine into the surrounding
tissues
When giving iron preparation always
confirms that the patient is not sensitive to it by giving a test done
Types of IV Administration
Adding the medicine in intravenous
solution bottle (intravenous infusion)
Existing intravenous line for
continuous infusion
Bolus: direct intravenous push for
immediate or fast action
Selection of Syringe and Needle
The size of syringe used for
intravenous infusion depends upon the amount of fluids to be injected
Size of the needle used are 18 to 21
gauge or 1 to 2 inches
Preliminary Assessment
Check
The diagnosis and age of the patient
The purpose of injection
The doctors order for the type,
dosage, time and route of administration
The patient’s name and bed number
The nurses record to find out the
time at which the last dose was given
The symptoms of overdose or allergic
reaction
The necessity for giving test dose
The form of the medicine available
and correct method of administration
The level of consciousness of the
patient
The site and previous experience of
the patient
Equipment
A tray
containing
Syringe and needles of various sizes
according to the need in a covered tray (sterile)
Transfer forceps in a jar containing
antiseptic solution
Sterile cotton swabs and gauze pieces
in sterile containers
Methylated spirit in a container
Bowl with water
Tourniquet
Water for injection
Drug order sheet
File to cut open the ampoules
Small covered tray (sterile)
Preparation of the Patient and Environment
Identify the patient correctly
Explain the procedure to the patient
Provide privacy
Place the patient in comfortable and
relaxed position suitable of intravenous injection
Select a site suitable for the route
of administration, quantity of medication to be given and characteristics of
medication
Procedure
Read the doctors order and select the
medication
Wash hands
Select appropriate syringe and needle
and check whether they are in good working order
Recheck the order, medicine card with
the label of the medicine, expiry date, etc
Mix well and take out the required
amount of solution in the syringe
Carry medicine to the patient
Method of Administering IV Infection
Apply a tourniquet on the upper arm
Ask the patient to clench and
unclench the hand
Pull the skin taut and place the
needle in line with vein at a 15 to 45 degree angle
Insert the needle, a bit below the
point where the needle will pierce the vein
When the back flow of blood occurs
into the syringe release the tourniquet and injects the medicine very slowly
Pressure with swab at the puncture
site after the needle is withdrawn to prevent bleeding
After Care
Observe the area for bleeding if
bleeding occurs apply pressure but do not massage
Give comfortable position to the
patient
Ask the patient to take rest at least
15 to 30 minutes so that you can observe him for any reaction
Observe the patient for any allergic
reaction
Replace the equipment used for
injection
Clean all other articles and replace
them in their proper place
Wash hands
Record the procedure on the nurse
record sheet and medication sheet
Complications
Allergic reactions
Pain
Injection abscess
Injury to nerves
Air embolism
INTRAVENOUS INJECTIONS – Purpose, Sites, Instructions, Administration, Equipment, After Care, Procedure, Complications
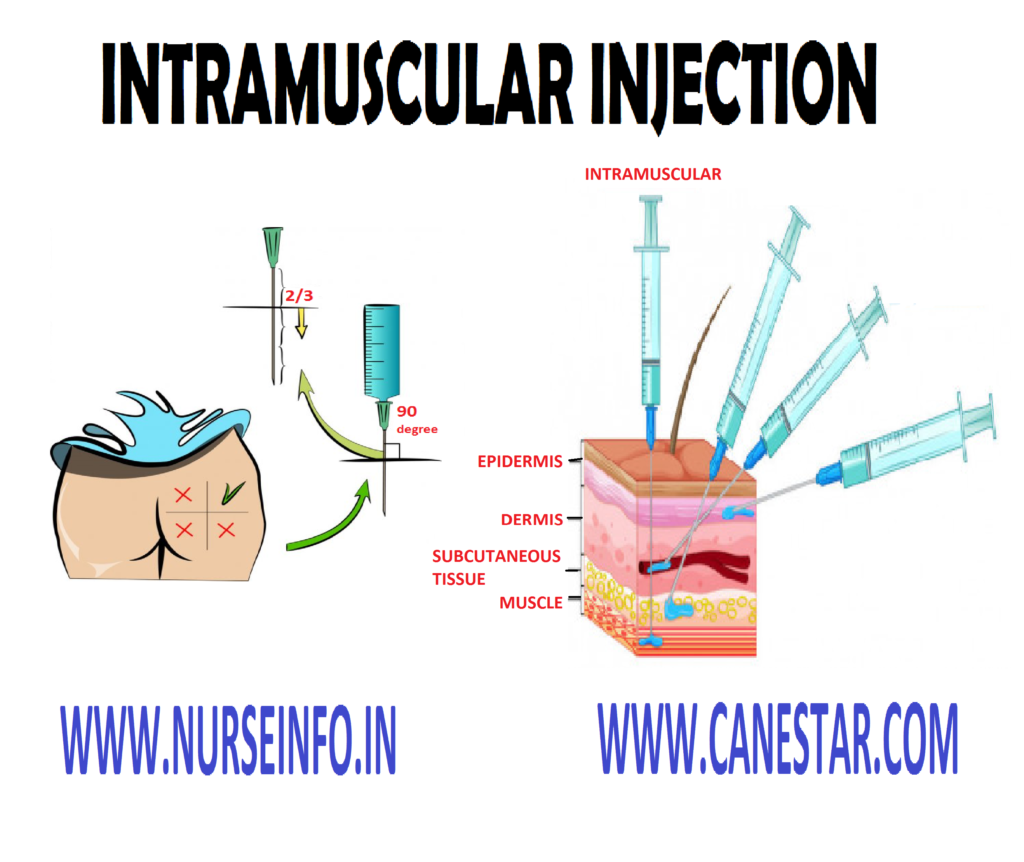
Intramuscular
injection is defines as introduction of medicine into the muscle in form of
solution
Purpose
To obtain a quick effect of medicine
than is obtained by oral administration and subcutaneous administration
Assures that the total dosage will be
administered and the same will be absorbed for the systemic action of the drug
The medicines that is not suitable
for intravenous administration
Principle
The knowledge of the anatomy and
physiology of the body is essential for the safe administration of the
injection
Injections are means of introducing
infection into the body, if carelessly given
Drugs that change the chemical
composition of the blood will endanger the life of the patient, if not used
cautiously
Any unfamiliar situation produces anxiety
Once a drug is injected it is
irretrievable. Antidote may be available for particular medications but the
best antidote is prevention
Organization and planning results in
the economy of time, material and effort
General Instructions
Give injections only on the doctors
written orders
Follow strict aseptic techniques
Syringes and needles used for
injections should be kept separate from those used for other purpose
Always have the syringe and needles
in good order
Change the needle after withdrawing
the drug from a rubber stopped container before giving injection to the patient
Observe the five rights of the
administration of medicines
Never use a drug whose expiry date is
over
Always have a patient relaxed and
placed in a comfortable position
Never allow the patient to walk soon
after the injection
Select the appropriate site for
giving injections
Rotate the site for patients getting
insulin to prevent lip dystrophy
Use correct technique of injection –
the needle inserted gently and quickly, and the drug injected slowly
After inserting the needle, always
withdraw the piston to make sure that it is not in a blood vessel in case of
intramuscular and subcutaneous injections
Solution for injection should be
clear, sterile, nearly neutral in reaction
Massage the area at the site of
injection except in case of intradermal injections
Injection should be charted
immediately
Site of Intramuscular Injections
Dorsal gluteal site: find out the
greater trochanter of the femur and the posterior superior iliac spine drawn an
imaginary line between these two bony prominences. Site will be upper and outer
quadrant
Vastus lateralis site: the site is at
the outer aspect of the thigh. It is the area between mid-anterior thigh and
mid lateral thigh one hands span from elbow and great trochanter to one hands
span above knee
Ventrogluteal site: place the tip of
the index finger on the anterior superior iliac spine of the patient the middle
finger just below the iliac chest
Mid deltoid site: locate the lower
edge of the acromion process and form a rectangle. The deltoid area is used to
inject very small quantities of non-irritating drugs
Methods of Intramuscular Injection Administration
Air lock method: expel the air from
the syringe leaving 0.2 ml, stretch the skin lightly with the index finger.
Insert the full needle quickly into the muscle. Withdraw the piston to confirm
that the needle is not in the blood vessel. Push the piston gently to give the
medicine very slowly
Z-tract method: expel the air from
the syringe; displace the skin laterally using the side of your left hand.
Insert the needle, aspirate the placement, inject the medicine very slowly,
marinating tissue displacement wait for ten seconds to allow the medicine to
disperse. Withdraw the needle allowing the displaced tissue to return to its
normal position
Nurses Responsibility
Check
The diagnosis and age of the patient
The purpose of injection
The doctors order
The patient details
The nurses record about previous
The allergic reactions
The necessity for giving test dose
The levels of consciousness and
follow instructions
The site of injection
The patient’s previous experiences
Equipment
A tray
containing:
Syringe and needles of various size
(sterile)
Transfer forceps in a jar containing
antiseptic solution
Sterile cotton swabs and gauze pieces
in sterile container
Methylated spirit in a container
Bowl with water
Kidney tray and paper bag
Drug order sheet
Water for injection
File to cut upon the ampoules
Small covered tray (sterile) to carry
the prepared injection to the bed side
Preparation of the Patient and Environment
Identify the patient correctly
Explain the procedure to the patient
Provide privacy
Keep the patient’s attention away
from the injection by friendly conversation
Place the patient in a comfortable
and relaxed position
Select a site suitable for the route
of administration
Procedure
Select the medication
Hand wash
Prepare the medication
Keep the syringe with medications in
the sterile tray and cover it
Make sure that the medicine taken
right and correct dosage
Carry medication to the patient in a
sterile tray
Identify the right patient
Prepare the site of injection
Inject the medicine by correct
technique is essential for the safety of the injection
Spread the tissue between the thumb
and forefingers to make the skin taut
Needle is inserted at a 90 degree
angle holding the syringe back the piston with the left hand
Using a steady push on the needle and
aspirate by pulling back the piston with left hand
If no blood comes gives the
medication slowly by pushing the piston
Remove the needle quickly and massage
the site for quick absorption of the drug
After Care
Inspect the area for bleeding
Help the patient to dress up
Ask the patient to take rest for 15
minutes
Check the limb movement to confirm
there is no nerve injury
Watch for the signs and symptoms of
allergic reaction
Indication: treat mainly gram positive infection (e.g. otitis media), meningitis, endocarditis, pneumonia. Act by interfering with bacterial cell wall synthesis – well distributed. Poor penetrator to CSF (except inflamed one). Ineffective against penicillin’s producer bacteria. Safe in pregnancy
Side effect, contraindication (C/I): serious allergic reactions rarely encephalopathy with high dose or normal dose in renal impairment patients. Never to be given intrathecally. Encephalopathy could be fatal. Accumulation of Na+ or K+ for electrolyte restricted patient
Flucloxacillin: of narrow spectrum but effective against pencillinase producer bacteria of good effect against MSSA (Methicillin Sensitive Staph aureus). Piperacillin known as anti-pseudomonal penicillin. Its activity is extended to cover gram negative bacteria. Indicated when serious infection by P.aeruginosa is suspected
Drug Interaction of Penicillin
With probenecid,
reduced excretion of penicillin
Synergistic
effect with aminoglycoside against gram negative bacteria
Reduces
excretion of methotrexate, increases MTC toxicity
Cephalosporins: are classified into first, second and third generation and this is determined by the activity against gram negative
They are of broad
spectrum (positive and gram negative) act by the same way as penicillin does
Rochin (ceftriaxone) of longer half-life is given once bacteria and stability against betalactamase enzyme. Daily in preoperatively prophylaxis
Fortum (Ceftazadine) of good pseudomonal effect. Side effect and contraindication: allergic reaction
Amikacin-Gentamicin: bactericidal acts against gram negative bacteria including P. aeruginosa
Side effects:
Damage the 8th
cranial nerve leads to deafness, ototoxicity
Nephrotoxicity
Excreted via
kidneys in renal impairment, accumulation may occur (i) never exceed 7-10 days
treatment with Amikacin-Gentamicin. (ii) Never to be given more than TDS/daily.
It is given in combination with and hemolytic Streptococci pneumococci.
Contraindication in pregnancy. Plasma level monitoring is required for peaks
and troughs
Drug interactions
With
cyclosporin increase the risk of nephrotoxicity
With
cisplatin increase the risk of nephrotoxicity and ototoxicity
Erythromycin injection:
Indication: alternative to penicillin for penicillin hypertensive patients, good for upper respiratory tract infection, campylobacter enteritis, atypical pneumonia, legionella. Contraindicated, in liver disease (porphyria)
Side effects: if given for more than 14 days – cholestatic jaundice. Avoid concurrent administration of hisminal or teldane
Drug Interaction: erythromycin inhibits hepatic microsomal enzyme leads to increase plasma concentration of antiarrhythmic, carbamazepine, terfenadine, and cyclosporin
Vancomycin: drug of choice in treatment of pseudomembranous colitis. MRSA, prophylaxis for endocarditis
Side effects/Caution: avoid rapid infusion (anaphylactic shock. Rotate the infusion site. Renal toxicity. History of deafness. Blood disorder should be considered seriously with vancomycin
Vitamin K
Indication: vitamin K deficiency bleeding. Good antidote for bleeding due to overdose of oral anticoagulant
Patient with
fat malabsorption (obstructive biliary) are advised to take water soluble forms
Aminophylline
Indication: indicated alone or in addition to beta 2 agonist to relieve bronchospasm. The drug is metabolized by liver cirrhosis, viral infection – cimetidine, erythromycin. Aminophylline half-life decreased with rifampicin, smoking, phenytoin and carbamazepine. The significance of half-life is important as the therapeutic toxic margin of aminophylline is narrow. When initiating IV therapy with aminophylline we should make sure that the patient was not taking from oral of aminophylline
Side effects: arrhythmia due to hypokalemia, convulsion, GIT disturbance. Aminophylline toxicity is treated by correcting the hypokalemia with KCI (60 mmol/1 hour), tachycardia is treated with IV propranolol
Dopamine/Dobutamine
They are inotropic drugs, cardiac
stimulant, exerting their action through beta 1 receptor at the heart.
Indicated in case of cardiogenic shock
Side effects: tachycardia
Half-life: it is only 1-2 minutes as
they are destructed by MAO. This is why it should be given in continuous
infusion. Hypovolemia should be corrected first
Intrathecal Injections
Definition and purpose: medicine injected in the subcutaneous arachnoids space of the spinal canal drugs such as anti-infectious or anti-neoplastic used for treating meningeal leukemia are injected by this route as they do not travel in the bloodstream. It is also given for anesthesia such as lidocaine hydrochloride (for regional anesthesia)
Complications
Inflammation at the puncture site
Septicemia
Spinal deformities especially while
giving anesthesia
Note: care must be taken when preparing this kind of injections to ensure that they do not have any bacterial substance
Epidural Analgesia Administration
This
procedure is usually performed by the doctor
Purpose
It is used for pain in deteriorating
condition of joints
To relieve acute pain or chronic in
other areas of the body
Procedure: the medicine is injected into the epidural space, which is situated just outside the subarachnoid space where cerebrospinal fluid flows. Medicine get spread slowly into the subarachnoid space of the spinal canal then goes into the spinal fluid (CSF) which carries it directly into the spinal area bypassing (avoiding) the blood brain barrier. However, in some cases medicine may be injected into subarachnoid space intrathecally
Blood-brain barrier: it is a barrier membrane between circulating blood and brain. It prevents any damaging substance from reaching the brain tissues and cerebrospinal fluid
Intra-articular Injections
Intra-articular injections are used when drugs are introduced in inflamed
joint, hydrocortisone acetate suspensions are used in this way. Care must be
taken to ensure sterile technique
Intracardiac Injections
Intracardiac injections are used for cardiac arrests.
Drug used are: coramine; micron adrenaline 1-1000. They are given in precardial area inside the mid-clavicular space
COMMONLY USED INTRAVENOUS DRUGS – Indications, Side Effects, Injections, Nephrotoxicity, Drug Interactions