Increase in
body weight of 10-20% above the normal, caused by excess accumulation of fat is
termed obesity. Healthy young men and women have a total body fat content below
20 and 25% respectively. When excess calories are supplied in any form, they
are stored as fat.
In addition
to general appearance and weight, measurement of skin fold thickness over the
biceps, triceps, subscapular and suprailiac regions is helpful in the assessment
of obesity. The skin fold thickness over the triceps for normal Indian subjects
is below 20 mm. The proportion of body fat can be accessed from the skin fold thickness
using nomograms.
Obesity has
become the sixth common cause for disease burden worldwide. Adipose tissue in
the body, in addition to its role as a source of stored energy, is emerging as
an endocrine organ producing hormone and cytokines. In general the ideal weight
of an individual should be (height in cm minus 100) kg .For example an adult
male 175 cm tall should have a weight of 75 kg ± 5%.
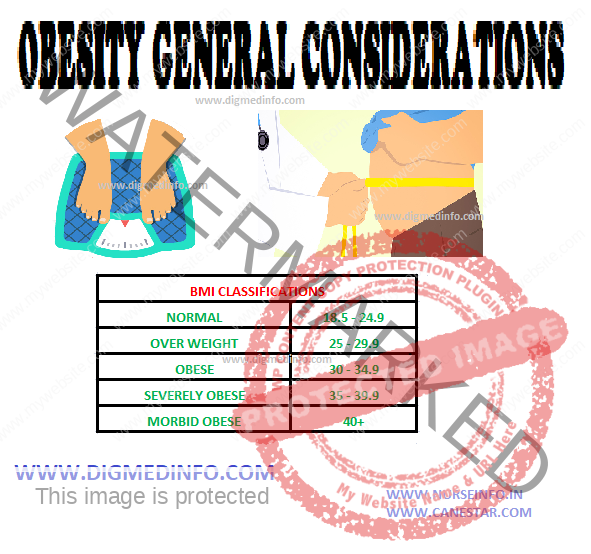
Body Mass
Index (BMI)
Body weight
is only a crude indicator of obesity. A more reliable parameter is the BMI.
BMI =
(Weight in kg)/height in m2)
Small community-based
surveys done in several parts of the country give figures ranging from 17-38%
BMI above 28 is associated with higher incidence of strokes, ischemic heart
disease and diabetes mellitus. The distribution of fat deposition in the body
is also important. For this purpose the circumference at the waist and the hip
are taken as reference measurements.
Waist is
measured after an overnight fast at the midpoint between the lower costal margin
and iliac crest. Hip is the widest part over the gluteal region. Waist hip
ratio above 1.0 in men and above 0.9 in women is an independent risk factor for
higher incidence of insulin resistance, hypertension, rise in LDL, lower levels
of HDL, hyperuricemia, cardiovascular disease, type 2 diabetes and stroke.
Ideal waist to hip ratio is below 0.85 in men and 0.75 in women. The waist circumference
above 102 cm (403) is an independent risk factor.
Abdominal obesity with accumulation of fat in the abdominal viscera is more associated with metabolic complications. The waist/hip ratio shows a graded and highly significant direct relationship with the risk for myocardial infarction.
OBESITY – CLINICAL FEATURES, COURSE AND PROGNOSIS and DIAGNOSIS
CLINICAL FEATURES
Middle-aged
persons are more affected though no age is immune. Women outnumber men and the
male to female ratio is 1:5. Multiparity is associated with increasing grades
of obesity. The patient may not complain of her obesity on account of its
gradual development and, therefore, it has to be identified during general
examination. Common symptoms include exertional dyspnea, sluggishness, angina, arthralgias
of knees and hips, or any of the complications.
Complications
These
develop invariably in all cases depending on the severity and duration of the
disorder.
1. Ill
effects of increased weight: Slowness of movement, proneness to falls and
accidents, osteoarthritis of weight-bearing joints like knees, hips, and spine.
2. Skin:
Abnormal skin folds develop and these give rise to fungal infection
(moniliasis), recurrent bacterial infections, and chafing of the skin of the
thighs and axillae. In extreme obesity, striae may develop.
3.
Cardiovascular system: Atherosclerosis, hypercholesterolemia, angina, ischemic
heart disease, hypertension, varicose veins, venous thrombosis, and recurrent
embolism. Increase of 10% of weight above the ideal weight leads to 30% rise in
the risk of heart disease.
4.
Respiratory system: Exertional dyspnea, reduction in vital capacity due to
restriction of diaphragmatic movements and the increased mechanical effort required
to move the thoracic cage, recurrent bronchitis, and in extreme cases,
respiratory failure. ‘Pickwickian syndrome’ is the condition where obesity is
associated with central depression of respiration and somnolence. Sleep apnea
and the related complications are more common in them.
5. Abdomen:
The skin over the anterior abdominal wall hangs down as a fold (“abdominal
apron”). Hernias develop owing to the increase in the intra-abdominal pressure.
Gallbladder lesions are more common.
6. Metabolic
complications: Diabetes mellitus, hyperlipidemias, gout, and cholesterol
gallstones are more common.
7.
Psychological abnormalities: Obese persons may develop depression because of
their unattractive physical appearance and mechanical disability. They tend to
avoid company and become socially isolated.
8. There is
evidence that cancer of the colon, breast, uterus, ovaries and prostate may be
more common in the obese.
COURSE AND PROGNOSIS
The
condition is gradual in its progress. Complications increase the mortality in
them. Mortality rate is 30% higher in persons 25-30% overweight and 50% higher
in persons 35-40% overweight. Death is caused by cardiovascular, metabolic or
respiratory complications. Obesity is an independent risk factor for higher
mortality.
DIAGNOSIS
Clinical
diagnosis is based on weight, physical appearance and measurement of skin fold
thickness. Sophisticated methods are available to establish the diagnosis in a borderline
case. Dual energy X-ray absorptiometry (DEXA) imaging gives a reliable
assessment of the
adipose tissue mass. Increase in weight occurring during pregnancy, fluid retention, hypothyroidism, hypothalamic lesions, and other endocrine disturbances should be differentiated from obesity due to nutritional causes. So also overweight may be caused by excessive muscular development in wrestlers, weight-lifters and boxers. Estimation of BMI, and the waist to hip ratio help to assess the risk of complications further. The aim of management is to reduce weight, achieve metabolic and physical fitness, reduce morbidity and achieve cosmetic results. A negative balance of 8000-9000 calories has to be achieved to clear 1 kg of adipose tissue.
OBESITY – CLINICAL FEATURES, COURSE AND PROGNOSIS and DIAGNOSIS
1. Excessive
consumption of food accounts for the vast majority. Training in early childhood
and social factors influence eating habits. Both in anxiety and depression,
excessive eating may be resorted to. It is not uncommon to develop obesity
after recent bereavement or change of job. An increase of 0.5% in food
consumption above the optimal caloric intake can lead to an annual rise in
weight of 1 kg. Pregnancy and contraceptive pills tend to predispose to obesity.
Persons show strong genetic predisposition to obesity and the amount of food leading to obesity
varies widely between subjects. Therefore prescription of dietary management
has also to be individualized.
2. Hormonal
and other factors Obesity may be part of the clinical pictures of well-known
endocrine disorders such as type 2 diabetes, hypothyroidism, Cushing’s
syndrome, gigantism, acromegaly, insulinomas and others. In addition several
hormones regulate appetite and modulate intake of food and fat accumulation.
Insulin and cholecystokinin acting on the central nervous system retard the
appetite regulating mechanism.
3. Genetic
factors do play a role. Metabolically, some individuals are more efficient in
conserving energy and thus they put on fat, while others require more energy
for the same amount of work performed.
Moreover,
obesity may run in families. The role of leptins There is strong evidence that
body fat is biologically regulated. Most cases of obesity probably reflect a
multigenetic predisposition for excess intake of food, low level of physical
activity and accumulation of excess amounts of fat. Leptin encoded by the Lcp
gene is a cytokine-like molecule synthesized and secreted by adipose tissue in proportion
to adipose tissue mass. It has several biological effects, an important one
being reduction of food intake. Leptin deficiency leads to hyperphagia, obesity,
and several endocrine abnormalities such as infertility, diabetes, reduction in
metabolism, impairment of somatic growth and elevated levels of glucocorticoids.
Leptin deficiency and resistance to leptin may be genetically determined.
Several
other hormones also influence food intake and body weight. A gut hormone
fragment peptide-Y3-36 (pYY) reduces appetite by acting on the appetite centers
in the hypothalamus. Ghrelin is a hormone primarily secreted by the stomach and
duodenum. Plasma ghrelin levels are higher before meals and their levels fall
after meals. Ghrelin has been implicated in causing hunger at meal times and
also the long-term maintenance of body weight.
Drugs
Several
drugs lead to weight gain. Prominent among them are antipsychotics, anti
depressants anticonvulsants, oral contraceptives, progestogens, oral hypoglycemic
agents, insulin, corticosteroids, beta adrenergic blockers, antihistamines and
others.
Childhood
obesity occurring below 3 years of age without parental obesity is not a risk
factor for obesity in adulthood. On the other hand obesity which persists beyond
6 years of age it is a predictor of adult obesity irrespective of the parental
status. Presence of obesity in the parents doubles the risk.
4. Physical
activity which causes loss of calories is closely related to obesity. Modern
amenities such as automobiles and lifts which tend to minimize day-today physical
exertion favour the development of obesity. Obesity is more evident when there
is a sudden cessation of physical activity. Eating habits are also influenced
by physical work. Moderate work is associated with optimal food intake whereas
both physical inactivity and overexertion lead to overeating.
5. Alcohol
being a good source of non-diet calories tends to aggravate obesity in the mild
and moderate alcoholics. Cessation of smoking leads to recovery of appetite and
gain in weight.
PATHOLOGY
Obese
subjects have increase of both fat and non-fat mass. In obesity developing from
childhood, there is probably increase in the number of fat cells and a generalized
increase in adipose tissue.
In others there is hypertrophy of the fat cells. Distribution of obesity may be android (abdomen and shoulder predominantly) or gynoid (buttocks, thighs, breasts, arm and face predominantly. Obesity leads to impairment of carbohydrate tolerance, elevation of cholesterol level in blood, and mild elevation of blood pressure. It predisposes to premature atherosclerosis. Obesity is associated with an absolute increase in energy expenditure, lower respiratory quotient and insulinresistance. Though obese subjects have to spend more energy for the same amount of work done by their normal counterparts, they tend to restrict their physical activity further and accumulate more fat.
Nicotinic
acid forms an integral part of nicotinamide adenine dinucleotide (NAD) and its
phosphate (NADP) which acts as coenzymes in the metabolic pathways of glucose
and proteins. Nicotinic acid and nicotinamide have equal biological potency and
are together referred to as niacin. Tryptophan is converted into niacin in the body,
60 mg of tryptophan giving rise to 1 mg niacin.
DIETARY SOURCES
Dietary sources include liver, pulses, whole cereals, fish, meat, groundnuts, milk, eggs, and to a smaller extent, vegetables. Coffee contains appreciable amounts of this vitamin. Rice and other cereals contain this vitamin, major portion of which is lost by milling. In maize niacin is present in an unabsorbable form ‘niacytin’. Moreover, maize is poor in its content of tryptophan. One-fourth of the vitamin may be lost in washing and cooking, though cooking alone does not destroy it. Daily requirement is 6 mg/1000 kcals (15-18 mg/day). Deficiency of niacin causes pellagra.
MYIASIS – General Characteristics,
Classification, Cutaneous Myiasis (localized), Deep Myiasis, Ophthalmic
Myiasis, Intestinal and Urinary Myiasis
GENERAL CHARACTERISTICS
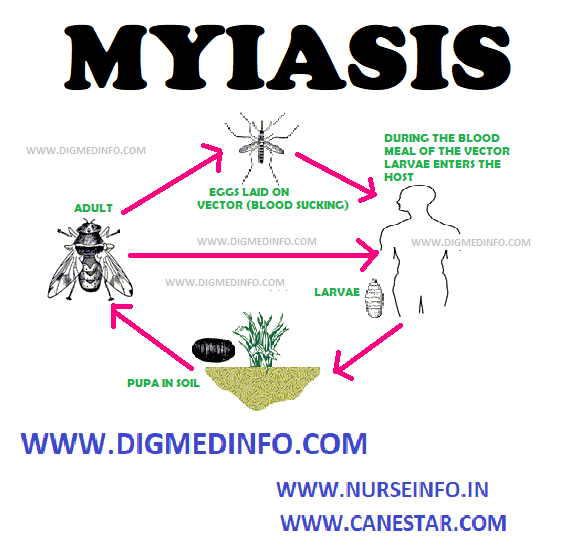
Invasion of
tissues or body cavities by the larvae (maggots) of dipterous flies is called
myiasis. Myiasis may be of either primary or secondary type. In primary myiasis
the human infection occurs as part of the obligate life-cycle of the parasite
and in secondary myiasis the human infection is accidental. Primary myiasis affects
persons in good general health, whereas secondary myiasis supervenes on dead or
necrotic tissues.
Classification:
In general,
the infection is of two types:
1.
Ectoparasitic, Auchmeromyia leuteola,
2.
Endoparasitic.
a. Cutaneous, e.g., caused by Dermatobia hominis
and Cordylobia anthropophaga,
b. Tissues or cavities, e.g., caused by
Sarcophaga, Wohlfartia, Fannia, Oestrus, Chrysomia, and Callitroga.
The maggots
are dull white or pink in colour, actively motile and have spines on their
body. The body is tapered and segmented, the narrow anterior end bears the
mouth parts, the thicker posterior end bears the opening of the spiracles which
are dark coloured and useful in identifying the genera. Their length varies
from 0.5 to 3 cm. The larvae feed voraciously on tissues or discharges and in 2
to 4 weeks develop and fall off to the ground to pupate.
Final
identification of the species can be done by allowing the larvae to complete
the life-cycle in vitro and examining the adult flies.
CUTANEOUS MYIASIS – ECTOPARASITIC
Auchmeromyia
leuteola (Congo maggot fly) This fly lays eggs on soil and crevices in the
floor. The larvae hatch out in 2 days. They can survive drying and starvation
upto one month. Once hatched out, they attach themselves to the skin of the
humans who sleep on the floor unprotected, suck blood for 20 minutes and drop
off leaving maculopapular lesions. This process is repeated several times
before the larva pupates in 2-12 weeks. Bites can be prevented by protective
clothing or insect repellents like dimethylphthalate or N-N diethyl benzamide.
Localised Cutaneous Myiasis
Dermatobia
hominis (Human bot fly or warble fly) The adult fly lays eggs on hematophagous
insects like mosquitoes, stomoxys and ticks or others such as housefly (Musca).
When the latter alights on man, the larvae hatch out and wriggle on to the
surface. They enter through the wound, produced by the insect or penetrate the
unbroken skin and develop in the subcutaneous tissues.
The initial
lesion is papular and pruritic. It becomes furuncle-like and painful later. The
posterior end of the actively motile larva may be seen in the lesion through the
opening. In 2-3 months the larvae mature and fall off to the ground. Lesions
are seen on the exposed parts. The disease is worldwide in distribution.
Cordylobia
anthropophaga (African tumbu fly) The adults lay eggs on clothes spread out for
drying or in dirty soil.
The larvae
develop in 24-48 hours and penetrate the human skin either from the clothes or
through the bare feet.
The lesion
is initially papular and pruritic and becomes painful in a short time.
Secondary infection may occur. Unlike the former, the life-cycle is shorter and
is completed in 2-3 weeks.
Treatment
The maggots
may be extracted surgically. A drop of mineral oil placed on the lesions
suffocates the larvae which wriggle out and can be extricated. Penicillin in
usual doses should be used to prevent secondary infection.
Migrating
lesions resembling cutaneous larva migrans are produced by the larvae of genus
Gastrophilus (horse bot flies) and Hypoderma (cattle bot flies), which develop from
eggs laid on the hairs. Man is an accidental host and the larvae penetrate the
skin, enter the subcutaneous tissues and wander producing eruptions similar to
larva migrans of Ancylostoma braziliense, but more painful. They survive for a
few weeks and die. Application of mineral oil over the lesions helps to
visualize the underlying larvae. Tissues of the eye may be affected. In addition
to surgical removal, symptomatic relief may be obtained by antihistamines.
DEEP TISSUE MYIASIS
Larvae of
the flies belonging to the families Callitroga (Cochliomyia), Chrysomyia,
Sarcophaga, Wohlfartia, Fannia and Oestrus invade tissues extensively when the eggs
are laid on open wounds, damaged tissues or discharging surfaces, by the adult
flies. The larvae of Wohlfartia can penetrate even unbroken skin.
The lesions
are commonly seen in the nasal cavities, paranasal sinuses, middle ear and
orbit. Cartilage and bone may also be destroyed by the screw-shaped larvae
which may extend intracranially leading to fatal meningitis. The lesions are
very painful and the larvae may be discharged from these sites.
TREATMENT
Treatment is
manual removal of larvae or extraction after spraying the area with chloroform.
Repeated sessions may be necessary.
Secondary
infection has to be treated with broad spectrum antibiotics like ampicillin.
OPHTHALMIC MYIASIS
Flies of the
genus Chrysomyia and Oestrus may lay their eggs in the conjunctival sac. The
larvae hatch out and produce lesions resembling acute conjunctivitis with severe
irritation. Rarely corneal ulceration and loss of sight may occur.
Removal of
the maggot after anesthetising the eye and application of topical antibiotic
drops will relieve the condition.
INTESTINAL MYIASIS
The larvae
or pupae of Musca, Fannia, Sarcophaga and Tubifera may be passed in stools or
appear in vomitus. The eggs may be laid by the flies around the lips or anus while
sleeping, especially if there foul smell discharges around these orifices.
The larvae
hatch out from a few hours to two days and are swallowed to reach the upper
gastrointestinal tract or they may crawl up into the rectum and large
intestine.
They develop
in the stomach or in the intestines. Sometimes larvae may be swallowed along
with infested foodstuffs. The larvae cause symptoms of gastritis or colitis
which may persist from weeks to months. If reinfection does not occur, the
condition is self-limiting. Treatment consists of administration of purgatives
and reassurance about the self-limiting nature of the illness.
URINARY MYIASIS
Larvae of Muscae, Fannia or Sarcophaga may enter the bladder, when the eggs are laid around the external genitalia and produce symptoms of lower urinary tract infection with proteinuria, pyuria and hematuria. The larvae may pass in urine. Rarely urinary system may be involved by maggots eroding their way from the gastrointestinal tract.
MYIASIS – General Characteristics, Classification, Cutaneous Myiasis (localized), Deep Myiasis, Ophthalmic Myiasis, Intestinal and Urinary Myiasis
MOTION SICKNESS – General Features, Clinical
Features, Courses and Prognosis, Prophylaxis and Treatment
General Features
The term
motion sickness refers to the clinical picture resulting from movement of an
individual on land, sea or air when journeys are undertaken. Repetitive
irregular movement as in a swing, a lift or even dancing, may bring on such
symptoms.
It is mainly
a disorder of gastric and intestinal functions brought on in susceptible
subjects while traveling. Irregular and unaccustomed stimulation of the labyrinth
causes nausea and vomiting and also disorders of function in the viscera
innervated by the vagus or parasympathetic system. During sea voyage the roll
and pitch of the ship causes excessive stimulation of the labyrinth. In the
case of car and aeroplane travel, labyrinth is subjected not only to the
effects of rotation of the body through planes to which it is not accustomed,
but also to rapid acceleration, deceleration and altitude changes.
Angular
acceleration of train and the linear-angular acceleration of turbulent flights
are important causes of motion sickness. Visual stimuli from moving objects and
proprioceptive stimuli from muscles and joints contribute to the final outcome.
Fear and anxiety make the condition worse.
Early
infancy is immune from this affection, since the orienting mechanism has not
attained full physiological activity and old age is relatively immune, probably
because of the lessened sensitivity of the nervous system. The signs and
symptoms of motion sickness occur when sensory information about the body’s
position in or movement through space is contradictory to prior experience.
Susceptibility and tolerance to motion sickness vary widely among individuals.
Motion sickness is more common in women, especially during pregnancy or
menstruation, in children aged 2-12 years, and in persons who have migraine
headaches.
Clinical features
The initial
symptoms include loss of usual sense of well being, abdominal and visceral discomfort,
salivation, nausea and yawning. The patient becomes pale and respiration
becomes irregular. These symptoms are followed by retching, vomiting and desire
to defecate. The vomiting may be mild and transient in some, while in others
this may be violent, distressing and recurrent. Headache, giddiness, continued
pallor, apathy, lassitude, weakness, dehydration and prostration follow.
The skin may
become cold and clammy, tongue coated, both breath and urine may contain
acetone bodies, pulse and respiration become rapid and the blood pressure drops.
Diagnosis is
easy when the symptoms are related to travel, but other causes of abdominal
disorders must not be overlooked.
Course and prognosis
The symptoms
usually subside when the travel or the movement causing the condition comes to
an end, but in some cases dizziness, headache and gastric symptoms persist for
a long time. In cases of long voyages by seas, the symptoms may subside in a
few days but may sometimes persist.
Prophylaxis and treatment
Reclining
posture, avoidance of visual stimuli and reduction in head movements to the minimum
help to minimize the condition. Mental
distraction may help to allay the symptoms. Antihistamines given in small doses 30–60 minutes before starting the travel prevent motion sickness, e.g., diphenhydramine 25-50 mg oral. phenothiazines such as trifluperazine 10 mg or hyoscine (0.3 mg) are good alternatives. To treat motion sickness higher doses of the same drugs have to be given. The choice of drug should be based on the underlying conditions if any.
MOTION SICKNESS – General Features, Clinical Features, Courses and Prognosis, Prophylaxis and Treatment
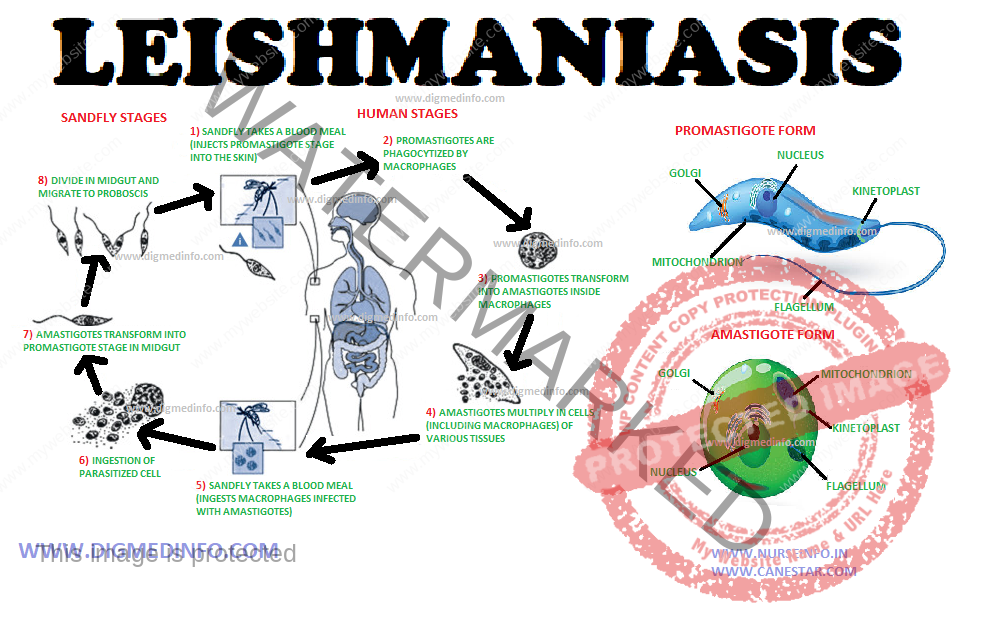
Infection by
the protozoan parasite of the genus Leishmania causes leishmaniasis. This may
take several forms. In India, the infection is prevalent in almost all states
sporadically. In the northern states it occurs in endemic and epidemic forms.
The main clinical presentations seen in India are visceral leishmaniasis (kala-azar),
post kala-azar dermal leishmaniasis and the primary cutaneous forms — tropical
sore; known by different names. India contains 70% of the global burden of
visceral leishmaniasis WHO has categorized leishmniasis as a category 1 disease
(i.e.) emerging and uncontrolled.
The parasite
affects mainly the reticuloendothelial organs and the related endothelial cells
primarily. Several vertebrate species may be affected by leishmania. In India, humans
form the main reservoir of infection. In the Mediterranean areas, Africa and
America other animalsalso harbour the parasites.
a. L.
donovani is the main species that causes visceral (VL) and post kala-azar
dermal leishmaniasis in India. In other countries other species also produce
the disease.
b. L.
tropica, L. major, L. aethiopica that cause oriental sore the primary cutaneous
form
c. L.
amezonensis – Mucosal form,
All these
species are morphologically similar but not immunologically. The parasite
exists in two forms
i. amastigote form, oval or rounded and nonmotile present in reticuloendothelial cells and ii. promastigote leptomonad or flagellate form seen in the vector – phlebotomus sand flies in which they develop and become infective in 7 days.
LEAD POISONING – General Features, Treatment, Chronic Lead Poisoning – Diagnosis, Treatment and Prevention
General Features
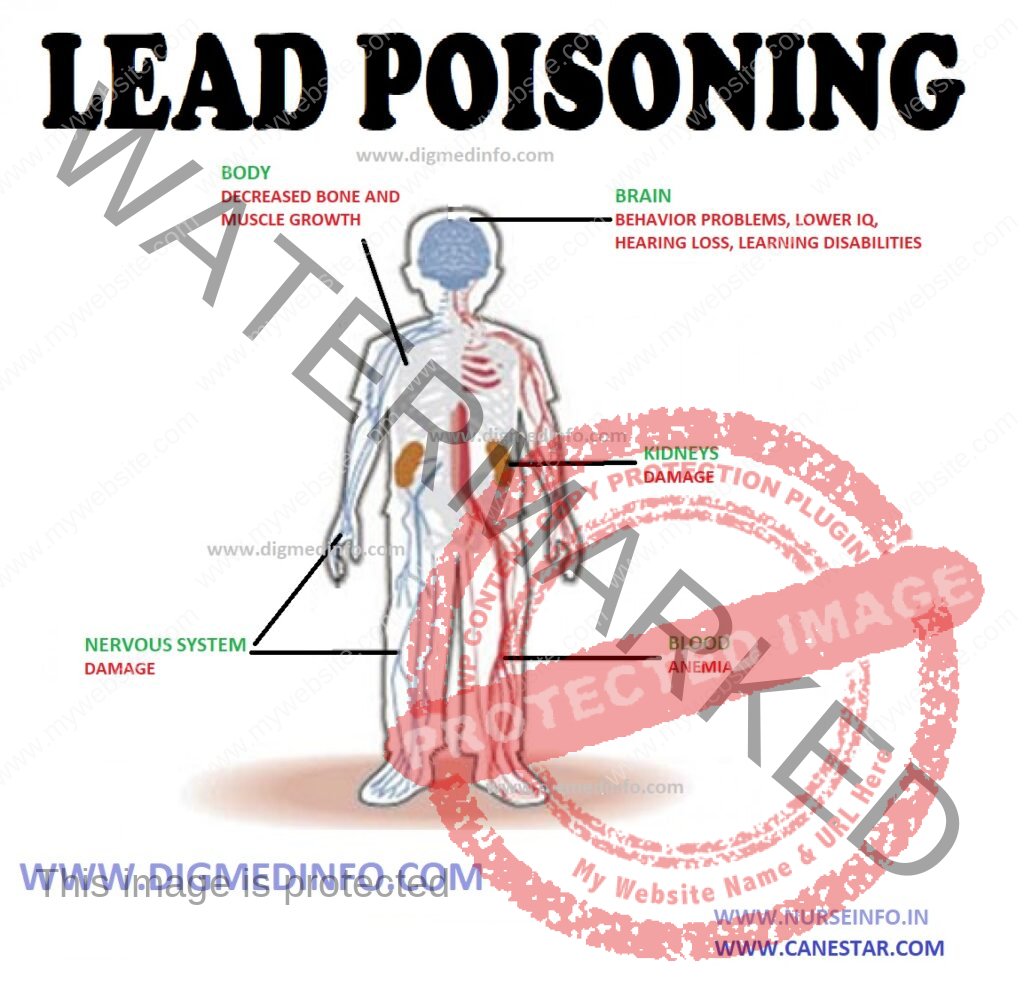
Lead
poisoning may occur in households among children and in industrial workers.
Lead is widely used in paints, storage batteries, petrol and several
industries. Ingestion, inhalation or absorption from the skin may lead to acute
poisoning. Workers engaged in printing, lead smelting, ship building, tank
cleaning are at risk of developing chronic toxicity. Children may eat flaked
paint as a form of pica. Lead accumulates in the body and it is deposited in
bone and other tissues.
Acute lead
poisoning Initial symptoms are metallic taste, irritation of throat, salivation
and intense thirst. These are soon followed by colicky abdominal pain, painful
spasm of abdominal muscles, hematemesis and constipation. The stools are black
due to the formation of lead sulphide. More serious cases develop drowsiness,
headache, and muscular cramps, and convulsions, paralysis of lower limbs, hemolysis
and renal failure.
Treatment
Calcium
disodium versenate (EDTA) in a dose of 1 g in 250 to 500 mL of 5% dextrose
intravenously twice daily (50 mg/kg/d) for 8-10 days or longer helps to eliminate
the lead. Symptomatic treatment is indicated as the condition warrants.
Chronic lead poisoning (Plumbism)
The main
symptoms are abdominal colic, constipation, hemolytic anemia, paralysis and
cerebral, cardiac and renal damage. It manifests initially as tubular damage
going on to chronic renal failure. There is no threshold level for lead to
initiate toxicity. Severe intestinal colic and constipation may be mistaken for
other alimentary disorders.
Most on the
lead and blood is present in erythrocytes. In chronic, lead poisoning the lead
is deposited in cortical bone. Lead impairs the enzyme delta-aminolevulinic
acid dehydrogenase which is needed for haem synthesis. Moderate to severe
hemolytic anemia occurs. The peripheral blood shows punctate basophilia and reticulocytosis.
In long term lead poisoning, the lead is deposited in cortical bone. Motor neuropathies
manifest as wrist drop and foot drop. Shoulder girdle muscles may be affected
rarely. Sensory symptoms are usually absent.
Lead
encephalopathy manifests as headache, loss of memory, epileptiform convulsions
and coma. Optic neuritis may occur. Urine may show protein, delta amino
levulinic acid, and coproporphyrin III. Blood pressure is elevated. Deposition
of lead in the gingival margins results in the formation of a black line in
people with poor oral hygiene.
In
edentulous subjects this lead line (Burtonian line) does not form. Chronic
renal failure may develop. It manifests initially as tubular damage, later,
tubular atrophy and interstitial nephritis. Exposure to lead during
intrauterine life leads to erosion of cognitive skills with subclinical but permanent
reduction in IQ. This may result is permanent impairment in performance
standards in adult life.
Diagnosis
The clinical
diagnosis is confirmed by the elevated levels of lead in blood. Levels above 80
mcg/Dl are diagnostic. A test for chronic lead accumulation is EDTA
mobilization test. Urinary loss of >600 mcg of lead in 72 hours indicates
lead poisoning.
Treatment
In severe
toxicity, EDTA is administered as described earlier. In less severe cases,
other than EDTA an oral chelator, Succimer (dimercaptosuccinic acid) has been
used in a dose of 10mg/kg orally every 8 hours for 5 days.
Prevention
Proper washing of the hands before eating and provision of protective clothing and masks reduce absorption of lead. Provision of 300 mL of milk to such workers may be helpful in reducing toxicity. Persons working in risky occupations should be periodically monitored. Pollution of the environment by lead salt is a major concern in recent years. The use of lead in automobile fuels has resulted in the discharge of appreciable amounts of lead into the atmosphere. In many states of India the use of leaded petrol is restricted.
LEAD POISONING – General Features, Treatment, Chronic Lead Poisoning – Diagnosis, Treatment and Prevention
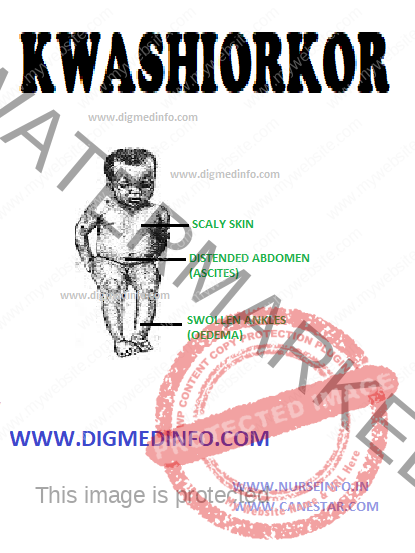
KWASHIORKOR – General Features, Pathology and Clinical Features
This name
was coined by Dr Cicely Williams in 1933, to denote ‘disease of the child
deposed from the breast by the conception of a new fetus’. Children between the
ages of 1 and 3 years are affected more. The disease starts when the baby is
weaned from the breast.
Pathology
Main changes
are seen in the small intestines, liver, pancreas and thymus. Small intestinal
mucosa shows blunting of villi and atrophy of brush border, so that the columnar
epithelium appears to become cuboidal. The total absorbing surface is reduced.
Lactose intolerance is common because of disaccharidase deficiency. Liver shows
fatty infiltration of the parenchymal cells. The pancreatic acini are atrophic
and enzyme activity is reduced. Thymus is markedly atrophied and this may contribute
to deficiency of cell mediated immunity.
Clinical features
This child is stunted and skeletal muscles are wasted. The presence of fairly normal amounts of subcutaneous fat and edema give a deceptively plump appearance. Pitting edema is a prominent feature. The child is apathetic, irritable and drowsy. Characteristic skin changes occur in many and when present; these are diagnostic. These include flaky paint dermatosis seen over areas of pressure and trauma, fissuring and ulceration at the flexures and a mosaic like appearance (crazy pavement appearance). The hair becomes thin, sparse, brownish and lusterless. They may fall off. Regrowth of normal pigmented hair heralds nutritional recovery. Since periods of nutritional deprivation and partial correction of nutrition alternate in many cases, the hair shows alternate bands of pigmentation and depigmentation (flag sign). The appetite is poor. Diarrhea is a frequent feature. There may be concomitant deficiencies of iron, folate, fat soluble vitamins and B complex factors. Hepatomegaly occurs in a third of the cases. This is due to fatty infiltration. With recovery the liver reverts to normal without sequelae.
KWASHIORKOR – General Features, Pathology and Clinical Features
JAPANESE ENCEPHALITIS – General
Characteristics, Transmission and Epidemiology, Pathogenesis and Pathology,
Clinical Features, Laboratory Diagnosis, Treatment and Prevention
Japanese
encephalitis (JE), a severe mosquito-borne infection of the CNS, is a leading
cause of childhood encephalitis in Asia.
GENERAL CHARACTERISTICS
Etiology and History
The
causative flavivirus is related antigenically to West Nile virus. The virus was
first isolated from human brain of an epidemic case in Japan in 1924 and its transmission
by mosquito was proved in 1936. It is an RNA virus. This disease has been
reported from several countries in both tropical and temperate zones.
Transmission and Epidemiology
The virus
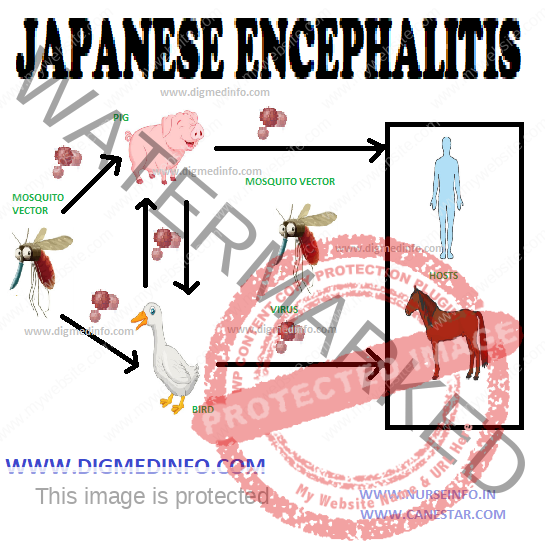
exists in reservoir hosts and man is affected from them. Pigs, birds such as
pond herons, cattle-egrets, bats, buffaloes, and cattle harbour the virus. In
India, pigs constitute the major reservoir in which the virus multiples. Migration
of birds accounts for the regional spread of infection. Though the virus is seen
in several animals, it is pathogenic only to man and a few other mammals like horses.
Poverty, unsatisfactory dwelling conditions and co-existance with cattle, birds
and pigs facilitate transmission.
The vector
Culicine mosquitoes act as the main vectors. Important among them are Culex
tritaeniorhyncus, C.pseudovishnui and C. vishnui. Anopheles barbirostris can also
transmit this virus.
The natural
transmission cycle of the virus is birds → mosquito → bird and pig → mosquito →
pig. Human infection occurs only when the mosquito population increases and man
– mosquito contact is established. Risk for infection is highest in rural
locations where rice fields, pigs and humans coexist.
In the vast
majority, the infection remains subclinical. The ratio of overt to inapparent
infection varies from 1:300 to 1:1000. Children below 15 years suffer more. The
peak incidence is between 2 to 10 years and males suffer more.
Pathogenesis and Pathology
After an
infective bite by the mosquito, the virus propagates locally and in the
regional lymph nodes. Viremia leads to affection of several organs mainly the brain
unless the infection is modulated by prompt immune response. Neuroinvasion
probably occurs as the virus grows through vascular endothelial cells to the parenchymal
side. The virus enters the neurons and leads to widespread degenerative and
necrotic changes. Most marked lesions occur in the cerebral cortex, thalamic nuclei,
corpus striatum, and brainstem with relative sparing of the white matter.
Cerebellar cortex and spinal motor neurons may also be affected, but the
affection is less marked. There is occlusion of the smaller arterioles leading
to extensive focal ischemia and necrosis. Perivascular hemorrhages and
mononuclear infiltration are seen.
CLINICAL FEATURES
The
incubation period ranges from 5-15 days. Three stages are recognizable-
prodrome, acute encephalitis and convalescence.
Prodromal stage:
The onset
may be gradual (4-5 days) or acute (12-24 hrs) or abrupt (1-6 hrs). The disease
starts as fever with chills, headache, meningism, convulsions, psychotic
behaviour and coma. Majority of cases recover in 4-5 days and clinical
diagnosis can be made initially, only during epidemics.
Acute encephalitic stage:
The fever
persists at 40-41o C, the pulse is rapid and neurological
manifestations predominate. Symptoms such as convulsions (70%), altered
sensorium (90%), focal neurological deficits, signs of meningeal irritation
(30%) and coma supervene. Supranuclear ocular palsies are common. Cranial nerve
palsies and papilledema are uncommon. These features help to identify JE from
tuberculous meningitis. Rapid onset of paralysis such as hemiplegia or
monoplegia is characteristic. Plantar responses are bilaterally extensor.
Other
manifestations of brain involvement include cerebellar signs, extrapyramidal
signs and dystonic postures.
Convalescence:
Neurological
function is regained gradually over several weeks, most of them by 6-12 weeks. For
the rest further recovery occurs after discharge over intervals of months to
years.
Laboratory Findings and Diagnosis
Leukocytosis
may be present and liver enzymes may be mildly elevated. CSF shows lymphocytic
pleocytosis. The cell count varies from 10-1000 cells/cmm, with an average of
100-200 cells. CSF protein may be raised to 50-250 mg/dL; sugar is usually
normal. EEG abnormalities are present in the acute phase. These include a
pattern of diffuse delta wave activity and rarely, spike and wave discharges.
EEG findings are not helpful in predicting the outcome. ECG may show nonspecific
ST-T changes indicating myocarditis.
MRI reveals
diffuse white matter edema and abnormal signals mainly in the thalamus, often
with evidence of hemorrhage in the basal ganglia, cerebellum, midbrain, pons
and spinal cord. The clinical diagnosis is easy during epidemics. Since this
disease often occurs sporadically, JE should always be considered in cases of
encephalitis.
LABORATORY DIAGNOSIS
Laboratory
diagnosis in most cases depends principally on the serologic testing of the
serum and also CSF by antibody capture enzyme linked immunosorbent assay
(ELISA). IgM and IgG antibodies can also be detected by indirect
immunofluorescence assay. The assay is more than 95% sensitive when serum
specimens are tested 7 to 10 days after the onset. Hemagglutination inhibition
(HI) or complement fixing antibodies can be demonstrated in paired sera and these
give evidence of infection in retrospect. Neutralizing antibody titer of 80 in
the serum is suggestive. Fourfold rise in titer is confirmatory. CSF neutralizing
antibody titer of 10 is confirmatory.
The virus
can be isolated from blood only during the first few days of illness, usually
preceding the onset of neurologic symptoms. Isolation of the virus from the CSF
indicates the absence of protective antibodies and therefore, poor prognosis.
TREATMENT AND PREVENTION
Treatment
There is no
specific treatment. Supportive treatment includes the correction of fluid and
electrolyte abnormalities, measures to control cerebral edema, anticonvulsants and
maintenance of nutrition. Use of human immunoglobulin in a dose of 150-200
mg/kg bw early in the disease has been claimed to reduce the severity and mortality
of the disease. There are preliminary data on the possible effectiveness of
alpha-interferon for treatment of JE. Further studies are required to confirm
the effect.
PREVENTION
Killed
vaccine using Nakayama Yoken strain of the virus is available for prophylaxis.
It is a formalin-inactivated vaccine. It is supplied as freeze dried vaccine,
which has to be stored below 10oC. The reconstituted vaccine should be
used within eight hours if kept cold. It should not be frozen. The recommended
schedule for adults in JE endemic areas is two doses of 1 mL each given SC at
an interval of 1-2 weeks. Protection starts one month after second dose. A
booster dose should be given after one month but within one year. One more
booster should be given after three years for full protection. In nonendemic areas
repeated booster doses should be given every three years.
For children
below three years the dose of vaccine is 0.5 mL, other conditions remaining the
same. The vaccine is immunogenic, and safe with only rare side effects. A live
attenuated cell culture derived vaccine (SA14 14-2 strain) has been used safely
and with high effectiveness in China.
Anti-mosquito measures help to limit the spread. Travelers to endemic areas should protect themselves against mosquito bite.
JAPANESE ENCEPHALITIS – General Characteristics, Transmission and Epidemiology, Pathogenesis and Pathology, Clinical Features, Laboratory Diagnosis, Treatment and Prevention